Outcome Measures in Spine Surgery: How Far Can we Go Building Evidence?
There is an imperative need to alleviate the actual and predictably harder burden of spine disorders and particularly the share due to chronic nonspecific low back pain, both at the individual and community-based viewpoint. Studies on global health trends charge a relevant part of the onus to the proposed invasive procedures, raising concern over its inappropriately high and growing use, counteracting clinical guidelines recommendation of a prudent selection of patients, based on clear-cut indications. Part of this gap between evidence and practice stands from questionable assumptions regarding the usefulness of surgery. Uncertainty on relative benefits and harms in the face of increased risk of adverse events, or the higher costs and health care resources involved, results in controversial decision-making to plan the intervention. Improvement of knowledge about these questions can be provided by the inclusion in the research agenda of comprehensive and standardized evaluation of outcomes after spine surgery. Such a protocol procedure would enable future systematic reviews to perform a consistent meta-analysis of data from trials, mandatory for high-quality evidence gathering. Outcome evaluation requires both subjective and objective assessments. This review aims to clarify the role of outcome measures in support of the need to build reliable information on the effectiveness of surgical treatment of spinal disorders.
Introduction
Despite the increasing body of evidence on the management of spinal disorders, studies on global health trends reveal a concerning spread of disability due to low back pain, with a considerable burden both to individuals and community.
This review starts to point out updated information on the global impact of back pain and how clinical guidelines implementation fails to promote best practice to quality care.
Controversial issues on the use of spinal disorders surgery are discussed regarding benefits and harms.
The role of outcome measures is clarified supporting the need to provide stronger evidence on the effectiveness of surgical treatment of these conditions.
The Global Burden of Spinal Disorders
According to the 2016 Global Burden of Disease study, the prevalence, incidence, and impact associated with low back and neck pain rose up to 50% more since it was first measured in 1990, with low back pain remaining the single leading cause of years lived with disability, and neck pain the fourth [1]. About one billion people worldwide suffer from these conditions throughout a period greater than three months duration [2]. Such an impact is predicted to rise, as mortality rates decline, life expectancy increases and global population ages, associated with the growing prevalence of risk factors for overall musculoskeletal conditions [3].
A substantial burden on society also derives after estimation of the total economic costs associated with the consequences and management of spinal conditions. Studies from many countries attempted to provide useful data, but methodological heterogeneity made it difficult to retrieve a clear global picture from them [4]. Particularly critical is the limited quality of the scarce studies carried out in less-developed rural communities, medically underserved areas and low- and middle-income countries, precluding a more comprehensive knowledge of the subject [5] (Figure 1).
Studies providing data on estimates of total costs associated with back or neck pain reveals that the most significant share is related to indirect costs resulting from lost work productivity [4]. As an example, in the USA, 25.5 million adults lost an average of 11.4 days of work due to back or neck pain in 2012, adding up to 290.8 million lost workdays in that year alone. The same report estimates 284 billion dollars of annual direct costs treating these conditions in the year before, a quarter of this amount being spent on hospitalizations, with discharge to long- term care nearly twice as those for any other health condition [6].
Such a significant impact on people’s lives, health-care systems, and community resources, demands a call for action [7], being the global challenge the prevention of harmful or wasteful practices while providing equitable access to adequate and affordable support to whom may need it. In fact, many international initiatives already address back pain as a significant problemfor the public health in overall setting [8].
Clinical Practice Guidelines to Improve Care
There is a widespread agreement on the need to alleviate the consequences of the actual and predictable future burden by increasing high-quality research on risk factors assessment and prevention, and identifying patient-centered, evidence-based, cost-effective and context-specific strategies for the management of spinal conditions. Many recommendations arising from clinical practice guidelines [CPGs] were therefore made available around the world to inform all the protagonists involved [9].
However, in a recent review, the overall quality of CPGs for musculoskeletal pain conditionswas identified as generallypoor, with only eight out of 34 rated as high quality [10], two of which for low back pain [11, 12] and one for neck pain [13]. The authors also mentioned how other spinal conditions are under-addressed:only four CPGs addressed neck pain (even being the fourth leading cause of disability as reported above), and no CPGs for thoracic spine pain (although a point prevalence of 72% in young females and one month prevalence estimates of 15.8% to 34.8% [14]).
Spinal Disorders Treatment and The Gap Between Evidence and Practice
While these efforts take place, a profound contrast exists between recommendations from best practice guidelines, in line with the evidence for the cost- effectiveness of strategies proposed to prevent and treat spinal disorders, and what happens in the real practice, whatever the income setting [9].
The most habitual obstacles are pointed out both to health professionals and population in general, as lack of awareness or an uneven distribution of available guidelines and existing knowledge [10, 15]. On the other hand, adherence to known guidelines seems to be a broad issue among clinicians, with substantial average delays as 17 years being reported for the adoption of evidence from randomized control trials into clinical practice [16], representing a consistent resistance to change (Figure 2).
Common examples of cost-ineffective, health staff over workload and non-evidence based practices are presentations toemergency services and liberal use of diagnostic imaging, opioid prescription, and invasive treatment like spinal injections or surgery, without an improvement in patient outcomes due to patient selection mismatches at primary care level [9, 15, 17, 18]. CPGs should reflect these discrepancies and highlight the crucial role of primary care assistance to promote optimal management pathways of spinal disorders at the baseline, and coherent follow-up at referral levels.
Spine surgery for back pain is one of the most controversial issues, regarding uncertainty on relative profits and risk of adverse events [19], in the face of the much higher amount of costs and health care resources involved. Instead, a broader consensus is achieved whenever the referral is based on the presence of severe or progressive neurological impairments [20], or conservative treatment has failed, and there is a clear association of symptoms with imaging findings of structural trouble/pathology, like herniated discs or spinal stenosis [12].
Although limited evidence exists to support this treatment option, the widespread and growing use of invasive procedures in the management of low back pain, especially in high-income countries [9] is adding some concern over these trends. In contrast with conservative approaches, the higher costs and the probability of immediate or late complications, which are inseparably tied to any surgery, request straightforward and explicit indications to the right treatment pathway, driven by updated and high-quality recommendations from CPGs. In fact, indicationsforsurgeryare advocated following unambiguous criteria.
The most usual surgical techniques proposed for back pain show conflicting evidence about their outcomes:
- Discectomy for a herniated disk with radiculopathy results in a faster relief than conservative treatment, but the benefits diminish after a year [20].
- Laminectomy for symptomatic spinal stenosis tends to have some benefits, but improvement results with or without surgery [21].
- Spinal fusion for non-radicular low back pain associated with degenerated discsimaging has benefits similar to those achieved by intensive multidisciplinary rehabilitation and modestly higher than standard non- surgical management [19].
- Spinal fusion after decompressive surgery for symptomatic spinal stenosis, with or without degenerative spondylolisthesis, does not increase outcomes [22, 23, 24].
- Disc replacement instead of spinal fusion demonstrated no clinical difference for pain or function in both the short and long-termand showed higher numbers of adverse events below four months [12].
- Interspinous process device decompression instead of conventional decompressive surgery is not supported by sufficient evidence about any advantageous beneficial effect [25].
These procedures have an insufficient evidence in cases of acute low back pain (less than six weeks), and only represent a second-line or adjunctive treatment option in cases of persistent low back pain (more than 12 weeks), where spinal fusion have an uncertain role [17, 26] and only offered to patients if part of a randomized controlled trial [12]. Disc replacement should not be offered at all [12] (Figure 3).
Clinical research on this subject seems to be biased by a marked tendency to analyze variations in surgical technique instead of looking to clarify what are the indications, if any, for surgery of spinal disorders. In this way, addressing the wrong question by missing the focus on the key problems is pointed out as having a little impact on patient outcomes and lesser evidence to help them regarding surgical intervention [27]. As a result, a paradigm shift about the role of back pain surgery is being delayed.
Current recommendations propose a shared decision- making process between clinicians and patients, to clarify the best choice considering benefits and harms, costs and effectiveness, different surgical techniques, and treatment alternatives. Although toughly implanted in modern approaches driven by patient-centered healthcare and argued as a way to facilitate clinicians use and patient adoption of CPGs with results in outcome improvement, no studies to date support or reject its use in the musculoskeletal pain field [28].
Building Evidence upon the Right Outcome Measures
There is a general agreement that trustworthy CPGs are based on high-quality systematic reviews of evidence [29]. In turn, quality of systematic reviews depend on the methodology used to assemble, appraise and summarize all relevant studies that address a specific clinical question, in a way that limit bias, which in the end mirrors the value of the research methods used by the individual studies, ideally in the form of a randomized controlled trial [30].
Trial selection in clinical research results after the application of inclusion and exclusion criteria. At that stage, a choice is made about the reported outcomes to be extracted and reviewed and those to be excluded, if any [30], from the whole set of measures that the trial team decided to report to quantify changes related to the subject under research. At both levels of decision, erratic or missing outcome data can lead to significant reporting bias, affecting the quality of evidence within a systematic review [31].
Outcome selection should be relevant to patients, clinicians, policy-makers, and stakeholders if systematic reviews of clinical research trials intend to influence practice, future research, and funding. Meta-analyses of clinical trials are unable to include data from all the relevant studies if outcome measures have not been consistently chosen. Outcome measures heterogeneity is a problem across back pain trials, affecting the consistency of reporting and completeness of the description, rendering difficult to accomplish a systematic review, hampering comparisons between studies [32].
The COMET (Core Outcome Measures in Effectiveness Trials) Initiative [http://www.comet-initiative.org/] developed a standardized approach to reporting, to be agreed and pursued among researchers in the form of a core outcome set [COS] that would benefit the systematic review process by increasing the amount of disposable information for use in a meta-analysis [33]. The agreement ensures that important outcomes are consistently assessed but does not preclude the choice of primary or secondary outcomes out of the COS. Only a small number of trials distinguish primary and secondary outcomes or fail to indicate a single primary outcome, which presents a major issue of reporting bias. Recommendations for interventiontrial protocols already include the need to identify primary and secondary outcomes [34].
The lack of an outcome classification system resulting in inconsistency and ambiguity across different studies, and inefficiency in searching published literature, was solved by a proposed new workable outcome taxonomy, the robustness of which has been demonstrated in reliable databases [35].
The initiative joined an international multidisciplinary panel to develop a COS applicable to clinical trials in patients with non-specific low back pain [nsLBP], having reached a consensus on four core outcome domains [36]:
- Physical functioning;
- Pain intensity;
- Health-related quality of life [HRQoL];
- Mortality.
More recently, a new study was conducted to build preliminary updating recommendations specifying a set of outcome measurement instruments for the first three core domains above mentioned, to be used in every clinical trial in patients with nsLBP, both acute and chronic, and updated as further evidence becomes available. An initial set of 25 potential patient-reported outcome measures [PROMs] were selectedregarding their measurement properties, feasibility, frequent use and approval in clinical trials from the nsLBP literature [33]. After a Delphi process to build consensus, only five achieved a place in the recommendations:
- The Oswestry Disability Index version 2.1a (ODI 2.1a [37, 38]) or the 24-item Roland Morris Disability Questionnaire for physical functioning;
- The Numeric Rating Scale with a 1-week recall period for pain intensity;
- The Short Form Health Survey 12(SF12 [39]) or the 10- item PROMIS Global Health (PROMIS-GH-10 [13]) for HRQoL.
Other initiatives like the International Consortium for Health Outcomes Measurement [ICHOM/http://www.ichom.org/] have conducted a survey to define a core set of standardized outcomes, having agreed with the basic three domains, but adding attention to work status, treatment complications, and medication requirements [43]. Psychosocial factors were excluded as they are probably reflected in the quality of life domain [50] (Figure 4).
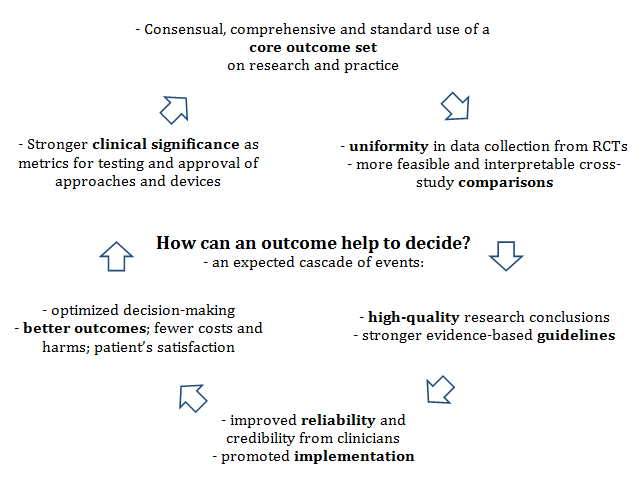
Standardization and uniformity in outcome data collection brought to spine surgery research the same advantages, with cross-study comparisons more feasible and interpretable, building a stronger evidence-base for spine treatments. Twenty year after the first major initiative proposed by Deyo and colleagues [40], PROMs are increasingly requireddue to their stronger clinical significance as metrics for testing and approval of approaches and devices [41, 42, 43, 44, 45, 46].
SPINE TANGO, an international spine registry system [https://www.eurospine.org /spine-tango.htm], with a large web-based spine surgery database, proposes an adaptation of previous core sets, focused specifically to back and neck surgical patients, with translated tools for the different languages of the participating countries [47, 48]. Determination of the “minimal clinically important difference” for improvement and deterioration after spine surgery, on the patient’s viewpoint is particularly stressed [49], as the standard for determining the effectiveness of a given treatment and describing patient satisfaction in response to that treatment.
The most recent UK guidelines on invasive treatments (including surgery) of low back pain and sciatica [12] agree with the previously mentioned core outcome set but consider psychological distress outcome measures equally critical for decision making. Responder criteria for pain and function, adverse events, revision rate, failure rate and healthcare utilizationwere also considered as important.
Pitfalls of Patient-Reported Outcomes
There is an implicit commitment from all the health community to focus on patient-centered care, assuming that is crucial to understand how each considers and assesses his health and quality of life [51]. In this sense, outcome measures based on the patient’s reportsare increasingly relevant to validate the effectiveness of therapeutic interventions. The confounding subjectivity of its nature ends up being its most powerful argument. Following the ICHOM statement: “… [patient-reported] outcomes are the ultimate measure of success in health care”. Economic costs and reporting of outcomes from providers with the participation of patients is driving some focus on the concept of “value-based healthcare” defined as the outcomes of care divided by the cost, with interesting effects on the quality of care [52, 53]. With evolving reimbursement systems, it may be conceivable that payment levels adjust based on outcomes [43].
Nevertheless, Schwartz and colleagues [45] account for pervasive paradoxical and counterintuitive findings when such evaluative rating scales are used, raising questions about what they assess and how scores should be interpreted. A good cited example is the “disability paradox”, where persons with significant disabilities report good to excellent quality of life. By integrating psychological factors along with patient attitudes and beliefs, PROMs have the potential to cause bias in outcome evaluations [54].
Inconsistent findings are also found in spine surgery in the form of discrepancies between clinical measures and self-reported ratings, affecting comparisons among individuals and within-persons over time [55]. Changes in the appraisal of well-being, symptoms, and functional health may reflect one’s values and conceptualization of quality of life induced by experience. In spinal surgery, this “response shift” phenomenon can cause the patient to use the same functional outcome report measure differently pre- and post-treatment [55]. These differences on estimates of treatment benefit may influence the conclusions of clinical trials and cost- effectiveness studies.
Another possible source of misleading interpretation of patient-reported data in spine surgery trials is the fact that patients could not reasonably be blinded to the intervention. Such a subjective outcome like pain can be modulated under the influence of significant placebo effects associated with the surgical procedure. Particularly in studies comparing surgery versus nonsurgical intervention, bias is likely to happen due to overestimation of benefits, challenging the interpretation of these outcomes [56].
Finally, patients with spine troubles have different clinical and behavioral presentations of their symptoms, according to the neurophysiological mechanisms underlying its origin or stage, experiencing either nociceptive, neuropathic, or central sensitization pain predominantly. This heterogeneityrequires careful interpretation of reported outcomes from ambiguous nature and subgrouping classification of this population to select preferable management strategies in clinical practice [57, 58].
The Need for Objective Outcome Measures
Without any detraction to the already praised advantages of patient-reported outcomes, provided that they are used systematically and combined in a consensual core set, it seems reasonable that more objective measures, assessing other issues less prone to uncertainty and bias, could reinforce evidence from trials looking for the effectiveness of spine surgery.
Objective assessment of body structure and functioning is performed for many purposes to quantify impairments or merely to evaluate integrity or measure the exertion of physiological systems. Biophysical factors are identified as importantcontributors to low back pain and disability [8], therefore sensitive to change under the effect of treatment strategies, including surgery, becomingpotential outcome dimensions (Figure 5).
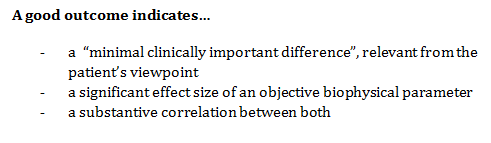
If a significant effect size between healthy controls and patients with spinal disorders is found during statistical data processing of a parameter, then it may be eligible as an objective outcome measure to assess the efficacy of surgery to that condition. It could be used to check how much does it improves and how long is it sustained after surgery; what are the baseline differences of that outcome between those who benefit from surgery and those who don’t; and finally what are the correlations between the level of a subjective outcome score and the measures of that parameter [59].
Unfortunately, potential pathoanatomical contributions to back pain and many physiological outcomes such as electromyogram activity, spine mobility, or straight leg raising results have a controversial or poor association with pain severity or functional status [41, 60, 61].
Pathoanatomical Factors
At first instance, back pain surgery aims to repair damaged tissue presumed as possible nociceptive source of pain in the spine, decompress compromised neural tissue, stabilize abnormal intersegmental movement, or correct alignment impairments or deformities. Disc herniations, Modic changes, annular tears, and spondylolisthesis, are examples of imaging findings (e.g.,Rx, TAC, MRI) commonly suggested as contributors to the problem [61]. The term “non-specific” used to classify the most prevalent form of low back pain points out the difficulties in confidently identifying a specific pathoanatomical cause like a vertebral fracture, malignancy, or infection, only present in a small proportion of patients [8, 62].
Evidence is missing on whether changes in that kind of imagingfindingsare associated with changes in clinical outcomes, although moderate evidence shows a favorable natural course of herniations and nerve root compression over a relatively shortperiod [61]. Furthermore, lumbar degenerative alterations are prevalent in the asymptomatic population [63], questioning the beliefs that spinal fusion should apply to solve degenerative pathology as a cause of back pain [27].
Postural Alignment
In a study of the general adult population, sagittal standing posture was not reliably related to quality of life in males, but females presenting high pelvic incidence and sacral slope showed increased odds of severe back pain [64]. Those parameters of spinopelvic angulationare determinants of the spine sagittal balance [65, 66] and highly correlated with back pain, by the influence of lumbopelvic alignment on vertebral mechanical stress and muscle workload during maintenance of posture [67].
Reconstructive fusion surgery of adult spine with degenerative deformities may result in a fixed sagittal imbalance, depending on the locked position of the fused vertebrae. The consequence is loss of lumbar lordosis with forward inclination of the trunk, decreased sacral slope, increased pelvic tilt and decreased thoracic kyphosis. This compensatory mechanisms aggravates previous damage due to physiological aging and may become a significant cause of chronic disability [68]. During lumbosacral arthrodesis, the mainchallenge is how it addresses optimal sacral alignment dealing with the risk of failing to correct or causing excessive retroversion of the sacrum [67].
On follow-ups, specific surgical alterations in this spinopelvic parameters are correlated with postfusion back pain and a higher risk of adjacent segment degeneration, and a predictive factor for degenerativespondylolisthesis. In contrast, restoration of normal lumbar lordosis and anterior pelvic tilt after surgeryis correlated with a good outcome [67, 68].
Sagittal alignment also plays an importantrole in outcomes after surgical correction of adolescent idiopathic scoliosis, but most of the significant correlations between spinopelvic parametersand clinical/functional outcomesfound in adult spinal deformity surgery, do not apply here [69]. Therefore, there is aneed for prospective comparative studies that consider pre- andpostoperative measures of radiographic spinopelvic parameters of sagittal balance and compare complicationrate and a standard core set of patient- reported outcomes, to prevent functional disability and provide more robust evidence on the effectivity of adolescent and adult spinal deformity surgery.
Postural Control and Balance
For any given task, several control strategies will ensure a stable spine, protecting against injury and pain, chosen to emphasize performance or reduced metabolic costs [70]. Evidence points out that people with low back pain have different control strategies than healthy individuals, using higher levels of trunk muscle co- activation as a protective coping scheme, exhibiting a rigid postural control with lesser variability in the range of options from their motor behavior repertoire [71, 72]. Structural and functional changes of the deep trunk muscles (transversus abdominis and lumbar multifidus) are also reported such as inhibition, delayed onset, atrophy, fatty infiltration and muscle fiber type mutation [73, 74, 75].
After spine surgery, studies also show that besides pain interference [76], patients may present some form of sensorimotor impairments compromising their motor performance [77, 78]. Proprioceptive deficit is referred as remaining from preoperative neural tissue compression or consecutive to surgical iatrogenicity by afferent denervation and dysfunctional central processing due to changes in spinal curvatures or insertion of rigid segments into a previously mobile linked system [79].
Assessment of postural control by measuring body sway during stance over a force platform is used to evaluate changes in motor performance due to spinal disorders or the outcomes of its management strategies [80, 81]. The trajectory of the center of pressure [CoP] of the ground reaction force under the feet is a measure strongly related to the movement of the body’s center of mass, and its quantification is applied to interpret balance behavior.
To our knowledge, only one systematic review was conducted on the use of postural control measures in spine disorders surgery. Yen and colleagues [82], analyzed the seven studies that met the full set of criteria, including the use of balance assessment tests pre- and post surgery (four on spinal fusion for scoliosis, two on decompression surgery for disc herniation, and one on spinal fusion for chronic low back pain). The most common parameters used were range/area, traveled distance, and velocity of CoP, assessed on force platform during upright stance.
Data analysis from spinal fusion for scoliosis surgery in adolescents revealed that body sway increased immediately following surgery but gradually reduced approaching the 1-year post spinal fusion assessment, denoting a prolonged period required for the proprioceptive system to adapt to changes in body posture and reach optimal truncal balance. For patients with disc herniation, all sway measures decreased immediately (3–4 days) post surgery. This improvement in postural balance is interpreted as patients having increased the role of hip strategy while standing, previously avoided due to increased back pain as a consequence of the heightened motion of the spine and its muscles [78].
Overall recommendations from this review indicate the need of longer follow-up times, assessed correlation with levels of reported pain, preference on time domain parameters over frequency domain (especially CoP velocity and sway area), and eyes-closed condition as more sensitive for identifying alterations in balance behaviors pre and post spinal surgery [82].
All studies in Yen’s review used standard linear measures to quantify the amount of sway read from posturographic data as an index of postural stability, assuming that less sway means better control. However, the magnitude of this variability around an average fails to account for the structured temporal organization of motor behavior, in the form of how a body sways to keep balanced or in the movement patterns during dynamic task performance [83, 84]. The concept of nonlinear dynamics suggests that complexity of motor behavior is the best measure of its variability, meaning to say that complexity can be revealed by nonlinear measures of the regularity and variability of motor output over a time series [85]. Combining linear and nonlinear tools (e.g., sample entropy, Lyapunov exponent, autocorrelation) can provide a comprehensive interpretation of the functionality of postural sway, useful to unveil different underlying motor strategies adopted in response to pain and other influences from pathology or treatment approaches [86], and become a significant set of outcome measures to apply in spine disorders/surgery patients.
A limited number of studies exist using other objective methods of motor performance assessments applied longitudinally following spinal treatment procedures. Examples include gait analysis [87, 59, 88] and other kinetic and kinematic analysis of range of motion and movement patterns using 3D video motion analysis [89], electromagnetic tracking systems [90], inertial sensors [91, 59], electronic inclinometers [60], EOS imaging system [91, 92], 3D CT scans [93, 94], digitized dynamic X- rays [95, 96, 97, 98, 99, 100] and motion analysis software (Figure 6).
Conclusions
Although implementation issues blur best practice based on already proven evidence, there is still a room for improvement of knowledge about the effectiveness of surgical treatment of spinal disorders, looking to optimize decision-making on those cases without a clear indication for surgery.
The inclusion of comprehensive and standardized evaluation of outcomes after spine surgery in the research agenda will enable future systematic reviews to perform a consistent meta-analysis of data from trials, mandatory for high-quality evidence gathering. Outcome evaluation requires both subjective and objective assessments.
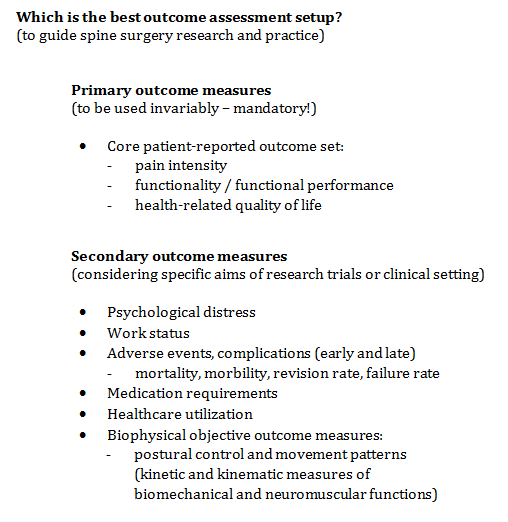
Subjective outcomes should be patient-reported and use consensual measures of pain intensity, functionality, health-related quality of life, defining a primary core set for systematic application. Psychological distress and work status should be considered if not accounted in global quality of life measures. Further effort is still required to develop a universal international set of outcomes, available and validated in many languages to be measured and compared as a part of standard clinical practice.
Mortality, adverse events, revision rate, failure rate and healthcare utilizationshould be consideredrelevant outcomes to include in spine surgery trials.
More studies should be encouraged to apply and develop objective outcome measures, harvesting stronger evidence of the impact of surgery on the patterns of posture and movement. Kinetic and kinematic measuring tools to study biomechanical and neuromuscular functions under the effect of constraints due to surgical procedures or subsequent rehabilitation approaches should have a more widespread diffusion. A better analysis of the correlations between subjective outcome scores and the measures of motor behavior parameters will provide reliable and useful information.
References
-
Vos T, Abajobir AA, Abate KH, Abbafati C, Abbas KM, et al. (2017) Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet 390(10100): 1211-1259.
-
Hurwitz EL, Randhawa K, Yu H, Côté P, Haldeman S (2018) The Global Spine Care Initiative: a summary of the global burden of low back and neck pain studies. European Spine Journal.
-
WHO (2018) Musculoskeletal conditions.
-
Dagenais S, Caro J, Haldeman S (2008) A systematic review of low back pain cost of illness studies in the United States and internationally. The Spine Journal 8(1): 8-20
-
Hurwitz EL, Randhawa K, Torres P, Yu H, Verville L, et al. (2017) The Global Spine Care Initiative: a systematic review of individual and community- based burden of spinal disorders in rural populations in low- and middle-income communities. European Spine Journal.
-
Bone_and_Joint_Initiative (2016) The Impact of Musculoskeletal Disorders on Americans- Opportunities for Action.
-
Buchbinder R, van Tulder M, Oberg B, Costa LM, Woolf A, et al. (2018) Low back pain: a call for action. Lancet 391(10137): 2384-2388.
-
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, et al. (2018) What low back pain is and why we need to pay attention. The Lancet 391(10137): 2356-2367.
-
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, et al. (2018) Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet 391(10137): 2368-2383.
-
Lin I, Wiles LK, Waller R, Goucke R, Nagree Y, et al. (2018) Poor overall quality of clinical practice guidelines for musculoskeletal pain: a systematic review. British Journal of Sports Medicine 52(5): 337- 343.
-
Globe G, Farabaugh RJ, Hawk C, Morris CE, Baker G, et al. (2016) Clinical Practice Guideline: Chiropractic Care for Low Back Pain. Journal of Manipulative and Physiological Therapeutics 39(1):1-22
-
NICE_UK (2016) Low Back Pain and Sciatica in Over 16s: Assessment and Management. National Institute for Health and Care Excellence (UK).
-
Côté P, Wong JJ, Sutton D, Shearer HM, Mior S, et al. (2016) Management of neck pain and associated disorders: A clinical practice guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. European Spine Journal 25(7): 2000-2022.
-
Briggs AM, Smith AJ, Straker LM, Bragge P (2009) Thoracic spine pain in the general population: Prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskeletal Disorders 10: 77.
-
Werber A, Schiltenwolf M (2016) Treatment of Lower Back Pain-The Gap between Guideline-Based Treatment and Medical Care Reality. Healthcare (Basel) 4(3): E44.
-
Casey DE (2013) Why don't physicians (and patients) consistently follow clinical practice guidelines? JAMA Intern Med 173(17): 1581-1583.
-
Debono B, Sabatier P, Koudsie A, Buffenoir K, Hamel O (2017) Managing spine surgery referrals: The consultation of neurosurgery and its nuances. Neurochirurgie 63(4): 267-272.
-
Layne EI, Roffey DM, Coyle MJ, Phan P, Kingwell SP, et al. (2018) Activities performed and treatments conducted before consultation with a spine surgeon: are patients and clinicians following evidence-based clinical practice guidelines? The Spine Journal 18(4): 614-619.
-
Chou R, Baisden J, Carragee EJ, Resnick DK, Shaffer WO, et al. (2009) Surgery for low back pain: a review of the evidence for an American Pain Society Clinical Practice Guideline. Spine (Phila Pa 1976) 34(10): 1094-1109.
-
Deyo RA, Mirza SK (2016) Herniated lumbar intervertebral disk. New England Journal of Medicine 374: 1763-1772.
-
Weinstein JN, Tosteson TD, Lurie JD, Tosteson A, Blood E, et al. (2010) Surgical versus Non-Operative Treatment for Lumbar Spinal Stenosis Four-Year Results of the Spine Patient Outcomes Research Trial (SPORT). Spine 35(14): 1329-1338.
-
Chen Z, Xie P, Feng F, Chhantyal K, Yang Y, et al. (2018) Decompression Alone Versus Decompression and Fusion for Lumbar Degenerative Spondylolisthesis: A Meta-Analysis. World Neurosurg 111: e165-e177.
-
Försth P, Ólafsson G, Carlsson T, Frost A, Borgström F, et al. (2016) A Randomized, Controlled Trial of Fusion Surgery for Lumbar Spinal Stenosis. New England Journal of Medicine 374: 1413-1423.
-
Rampersaud YR, Fisher C, Yee A, Dvorak MF, Finkelstein J, et al. (2014) Health-related quality of life following decompression compared to decompression and fusion for degenerative lumbar spondylolisthesis: a Canadian multicentre study. Can J Surg 57(4): E126-E133.
-
Gazzeri R, Galarza M, Alfieri A (2014) Controversies about Interspinous Process Devices in the Treatment of Degenerative Lumbar Spine Diseases: Past, Present, and Future. BioMed Research International 2014: 975052.
-
Peul WC, Bredenoord AL, Jacobs WCH (2014) Avoid surgery as first line treatment for non-specific low back pain. BMJ : British Medical Journal 349: 4214.
-
Andrade NS, Flynn JP, Bartanusz V (2013) Twenty- year perspective of randomized controlled trials for surgery of chronic nonspecific low back pain: citation bias and tangential knowledge. The Spine Journal 13(11): 1698-1704.
-
Tousignant-Laflamme Y, Christopher S, Clewley D, Ledbetter L, Cook CJ, et al. (2017) Does shared decision making results in better health related outcomes for individuals with painful musculoskeletal disorders? A systematic review. The Journal of Manual & Manipulative Therapy 25(3): 144-150.
-
Qaseem A, Forland F, Macbeth F, Ollenschläger G, Phillips S, et al. (2012) Guidelines international network: Toward international standards for clinical practice guidelines. Annals of Internal Medicine 156(7): 525-531.
-
Brown PA, Harniss MK, Schomer KG, Feinberg M, Cullen NK, et al. (2012) Conducting Systematic Evidence Reviews: Core Concepts and Lessons Learned. Archives of Physical Medicine and Rehabilitation 93: S177-S184.
-
Kirkham JJ, Gargon E, Clarke M, Williamson PR (2013) Can a core outcome set improve the quality of systematic reviews? A survey of the Co-ordinating Editors of Cochrane review groups. Trials 14: 21.
-
Gianola S, Frigerio P, Agostini M, Bolotta R, Castellini G, et al. (2016) Completeness of outcomes description reported in low back pain rehabilitation interventions: a survey of 185 randomized trials. Physiotherapy Canada 68(3): 267-274.
-
Chiarotto A, Boers M, Deyo RA, Buchbinder R, Corbin TP, et al. (2018) Core outcome measurement instruments for clinical trials in nonspecific low back pain. Pain 159(3): 481-495.
-
Cella D, Yount S, Rothrock N, Gershon R, Cook K, et al. (2007) The Patient-Reported Outcomes Measurement Information System (PROMIS): progress of an NIH Roadmap cooperative group during its first two years. Med Care 45: S3-s11.
-
Dodd S, Clarke M, Becker L, Mavergames C, Fish R, et al. (2018) A taxonomy has been developed for outcomes in medical research to help improve knowledge discovery. Journal of Clinical Epidemiology 96: 84-92.
-
Chiarotto A, Terwee CB, Deyo RA, Boers M, Lin CW, et al. (2014) A core outcome set for clinical trials on non-specific low back pain: study protocol for the development of a core domain set. Trials 15: 511.
-
Baker D (1989) The Oswestry Disability Index revisited. Back Pain: New Approaches to Rehabilitation and Education 174-186.
-
Fairbank JC, Couper J, Davies JB, O'Brien JP (1980) The Oswestry low back pain disability questionnaire. Physiotherapy 66(8): 271-273.
-
Ware JE, Kosinski M, Keller SD (1996) A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Medical Care 34(3): 220-233.
-
Deyo RA, Battie M, Beurskens AJHM, Bombardier C, Croft P, et al. (1998) Outcome Measures for Low Back Pain Research: A Proposal for Standardized Use. Spine 23(18): 2003-2013.
-
Bombardier C (2000) Outcome Assessments in the Evaluation of Treatment of Spinal Disorders: Summary and General Recommendations. Spine 25(24): 3100-3103.
-
Cieza A, Stucki G, Weigl M, Disler P, Jäckel W, et al. (2004) ICF Core Sets for low back pain. Journal of rehabilitation medicine (S44): 69-74.
-
Clement RC, Welander A, Stowell C, Cha TD, Chen JL, et al. (2015) A proposed set of metrics for standardized outcome reporting in the management of low back pain. Acta orthopaedica 86(5): 523-533.
-
Deyo RA, Dworkin SF, Amtmann D, Andersson G, Borenstein D, et al. (2014) Report of the NIH Task Force on Research Standards for Chronic Low Back Pain. Pain Medicine 95(2): e1-e18.
-
Schwartz CE, Sajobi TT, Lix LM, Quaranto BR, Finkelstein JA (2013) Changing values, changing outcomes: the influence of reprioritization response shift on outcome assessment after spine surgery. Qual Life Res 22(9): 2255-2264.
-
WHO (1999) Low back pain initiative. Low back pain initiative.
-
Mannion AF, Elfering A, Staerkle R, Junge A, Grob D, et al. (2005) Outcome assessment in low back pain: how low can you go? Eur Spine J 14(10): 1014-1026.
-
Röder C, Chavanne A, Mannion AF, Grob D, Aebi M (2005) SSE Spine Tango-content, workflow, Tango. Eur Spine J 14(10): 920-924.
-
Mannion AF, Porchet F, Kleinstück FS, Lattig F, Jeszenszky D, et al. (2009) The quality of spine surgery from the patient's perspective: part 2. Minimal clinically important difference for improvement and deterioration as measured with the Core Outcome Measures Index. Eur Spine J 18(S3): 374-379.
-
Chapman JR, Norvell DC, Hermsmeyer JT, Bransford RJ, DeVine J, et al. (2011) Evaluating common outcomes for measuring treatment success for chronic low back pain. Spine (Phila Pa 1976) 36: S54- S68.
-
Ibsen C, Schiøttz-Christensen B, Melchiorsen H, Nielsen CV, Maribo T (2016) Do Patient-reported Outcome Measures Describe Functioning in Patients with Low Back Pain, Using the Brief International Classification of Functioning, Disability and Health Core Set As a Reference? Journal of Rehabilitation Medicine 48(7): 618-624.
-
McGirt MJ, Resnick D, Edwards N, Angevine P, Mroz T, et al. (2014) Background to understanding value- based surgical spine care. Spine 39: S51-S52.
-
Porter ME (2009) A Strategy for Health Care Reform — Toward a Value-Based System. New England Journal of Medicine 361: 109-112.
-
McGregor AH, Doré CJ, McCarthy ID, Hughes SP (1998) Are Subjective Clinical Findings and Objective Clinical Tests Related to the Motion Characteristics of Low Back Pain Subjects? Journal of Orthopaedic & Sports Physical Therapy 28(6): 370-377.
-
Schwartz CE, Finkelstein JA (2009) Understanding inconsistencies in patient-reported outcomes after spine treatment: response shift phenomena. Spine J 9(12): 1039-1045.
-
Johnson AG (1994) Surgery as a placebo. The Lancet 344(8930): 1140-1142.
-
Nijs J, Apeldoorn A, Hallegraeff H, Clark J, Smeets R, et al. (2015) Low back pain: guidelines for the clinical classification of predominant neuropathic, nociceptive, or central sensitization pain. Pain Physician 18: E333-E346.
-
Smart KM, Blake C, Staines A, Doody C (2012) Self- reported pain severity, quality of life, disability, anxiety and depression in patients classified with ‘nociceptive’, ‘peripheral neuropathic’ and ‘central sensitisation’ pain. The discriminant validity of mechanisms-based classifications of low back (±leg) pain. Manual Therapy 17(12): 119-125.
-
Toosizadeh N, Harati H, Yen TC, Fastje C, Mohler J, et al. (2016) Paravertebral spinal injection for the treatment of patients with degenerative facet osteoarthropathy: Evidence of motor performance improvements based on objective assessments. Clin Biomech (Bristol, Avon) 39: 100-108.
-
Mannion AF, Dvorak J, Muntener M, Grob D (2005) A prospective study of the interrelationship between subjective and objective measures of disability before and 2 months after lumbar decompression surgery for disc herniation. Eur Spine J 14(5): 454-465.
-
Panagopoulos J, Hush J, Steffens D, Hancock MJ (2017) Do MRI Findings Change Over a Period of Up to 1 Year in Patients With Low Back Pain and/or Sciatica?: A Systematic Review. Spine 42: 504-512.
-
Maher C, Underwood M, Buchbinder R (2017) Non- specific low back pain. The Lancet 389(10070): 736- 747.
-
Hicks GE, Morone N, Weiner DK (2009) Degenerative Lumbar Disc and Facet Disease in Older Adults: Prevalence and Clinical Correlates. Spine 34(12): 1301-1306.
-
Araujo F, Lucas R, Alegrete N, Azevedo A, Barros H (2014) Sagittal standing posture, back pain, and quality of life among adults from the general population: a sex-specific association. Spine (Phila Pa 1976) 39(13): E782-E794.
-
Le Huec JC, Leijssen P, Duarte M, Aunoble S (2011) Thoracolumbar imbalance analysis for osteotomy planification using a new method: FBI technique. European Spine Journal 20(S5): 669-680.
-
Roussouly P, Gollogly S, Berthonnaud E, Dimnet J (2005) Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976) 30(3): 346-353.
-
Lazennec JY, Ramare S, Arafati N, Laudet CG, Gorin M, et al. (2000) Sagittal alignment in lumbosacral fusion: relations between radiological parameters and pain. Eur Spine J 9(1): 47-55.
-
Le Huec JC, Faundez A, Dominguez D, Hoffmeyer P, Aunoble S (2015) Evidence showing the relationship between sagittal balance and clinical outcomes in surgical treatment of degenerative spinal diseases: a literature review. International Orthopaedics 39(1): 87-95.
-
Ilharreborde B (2018) Sagittal balance and idiopathic scoliosis: does final sagittal alignment influence outcomes, degeneration rate or failure rate? European Spine Journal 27(S1): 48-58.
-
Reeves NP, Cholewicki J, Pearcy M, Parnianpour M (2013) How can models of motor control be useful for understanding low back pain? In: Hodges PW, Cholewicki J, van_Dieen JH (Eds.), Churchill Livingstone, Spinal Control, pp: 187-193.
-
Brumagne S, Janssens L, Knapen S, Claeys K, Suuden- Johanson E (2008) Persons with recurrent low back pain exhibit a rigid postural control strategy. Eur Spine J 17(9): 1177-1184.
-
Hodges PW, Tucker K (2011) Moving differently in pain: a new theory to explain the adaptation to pain. Pain 152(3S): S90-S98.
-
Hildebrandt M, Fankhauser G, Meichtry A, Luomajoki H (2017) Correlation between lumbar dysfunction and fat infiltration in lumbar multifidus muscles in patients with low back pain. BMC Musculoskeletal Disorders 18: 12.
-
Hodges PW, James G, Blomster L, Hall L, Schmid AB, et al. (2014) Can proinflammatory cytokine gene expression explain multifidus muscle fiber changes after an intervertebral disc lesion? Spine (Phila Pa 1976) 39(13): 1010-1017.
-
Hodges PW, Richardson CA (1998) Delayed postural contraction of transversus abdominis in low back pain associated with movement of the lower limb. J Spinal Disord 11(1): 46-56.
-
Moseley GL, Hodges PW (2005) Are the changes in postural control associated with low back pain caused by pain interference? Clin J Pain 21: 323-329.
-
Leinonen V, Kankaanpaa M, Luukkonen M, Kansanen M, Hanninen O, et al. (2003) Lumbar paraspinal muscle function, perception of lumbar position, and postural control in disc herniation-related back pain. Spine (Phila Pa 1976) 28(8): 842-848.
-
Sipko T, Chantsoulis M, Kuczyński M (2010) Postural control in patients with lumbar disc herniation in the early postoperative period. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 19(3): 409-414.
-
Sawatzky B, Tredwell S, Sanderson D (1997) Postural control and trunk imbalance following Cotrel- Dubousset instrumentation for adolescent idiopathic scoliosis. Gait & Posture 5(2): 116-119.
-
Mazaheri M, Coenen P, Parnianpour M, Kiers H, van Dieen JH (2013) Low back pain and postural sway during quiet standing with and without sensory manipulation: a systematic review. Gait Posture 37(1): 12-22.
-
Ruhe A, Fejer R, Walker B (2011) Center of pressure excursion as a measure of balance performance in patients with non-specific low back pain compared to healthy controls: a systematic review of the literature. Eur Spine J 20(3): 358-368.
-
Yen TC, Toosizadeh N, Howe C, Dohm M, Mohler J, et al. (2016) Postural Balance Parameters as Objective Surgical Assessments in Low Back Disorders: A Systematic Review. J Appl Biomech 32(3): 316-323.
-
Latash ML, Scholz JP, Schoner G (2002) Motor control strategies revealed in the structure of motor variability. Exerc Sport Sci Rev 30(1): 26-31.
-
van Emmerik RE, van Wegen EE (2002) On the functional aspects of variability in postural control. Exerc Sport Sci Rev 30(4): 177-183.
-
Harbourne RT, Stergiou N (2009) Movement variability and the use of nonlinear tools: principles to guide physical therapist practice. Phys Ther 89(3): 267-282.
-
Stergiou N, Decker LM (2011) Human movement variability, nonlinear dynamics, and pathology: is there a connection? Hum Mov Sci 30(5): 869-888.
-
Holewijn RM, Kingma I, de Kleuver M, Schimmel JJP, Keijsers NLW (2017) Spinal fusion limits upper body range of motion during gait without inducing compensatory mechanisms in adolescent idiopathic scoliosis patients. Gait Posture 57: 1-6.
-
Toosizadeh N, Yen TC, Howe C, Dohm M, Mohler J, et al. (2015) Gait behaviors as an objective surgical outcome in low back disorders: A systematic review. Clin Biomech (Bristol, Avon) 30(6): 528-536.
-
Chockalingam N, Bandi S, Rahmatalla A, Dangerfield PH, Ahmed ELN (2008) Assessment of the centre of pressure pattern and moments about S2 in scoliotic subjects during normal walking. Scoliosis 3: 10.
-
Cattrysse E, Moens M, Schaillée E, D'Haens J, Van Roy P (2012) Changed cervical kinematics after fusion surgery. Eur Spine J 21(7):1353-1359.
-
Duc C, Salvia P, Lubansu A, Feipel V, Aminian K (2013) Objective evaluation of cervical spine mobility after surgery during free-living activity. Clinical Biomechanics 28: 364-369.
-
Hasegawa K, Okamoto M, Hatsushikano S, Shimoda H, Ono M, et al. (2017) Standing sagittal alignment of the whole axial skeleton with reference to the gravity line in humans. Journal of Anatomy 230(5): 619-630.
-
Ilharreborde B, Dubousset J, Le Huec JC (2014) Use of EOS imaging for the assessment of scoliosis deformities: application to postoperative 3D quantitative analysis of the trunk. Eur Spine J 23(S4): S397-S405.
-
Barrey C, Champain S, Campana S, Ramadan A, Perrin G, et al. (2012) Sagittal alignment and kinematics at instrumented and adjacent levels after total disc replacement in the cervical spine. Eur Spine J 21(8): 1648-1659.
-
Champain S, Mazel C, Mitulescu A, Skalli W (2007) Quantitative analysis in outcome assessment of instrumented lumbosacral arthrodesis. Eur Spine J 16(8): 1241-1249.
-
Machino M, Yukawa Y, Hida T, Ito K, Nakashima H, et al. (2012) Cervical alignment and range of motion after laminoplasty: radiographical data from more than 500 cases with cervical spondylotic myelopathy and a review of the literature. Spine (Phila Pa 1976) 37(20): E1243-E1250.
-
Downie WW, Leatham PA, Rhind VM, Wright V, Branco JA, et al. (1978) Studies with pain rating scales. Annals of the Rheumatic Diseases 37(4): 378- 381.
-
Nagamoto Y, Iwasaki M, Sugiura T, Fujimori T, Matsuo Y, et al. (2014) In vivo 3D kinematic changes in the cervical spine after laminoplasty for cervical spondylotic myelopathy. J Neurosurg Spine 21: 417- 424.
-
Petit Y, Aubin CÉ, Labelle H (2002) Three- dimensional imaging for the surgical treatment of idiopathic scoliosis in adolescents. Canadian Journal of Surgery 45(6): 453-458.
-
Roland M, Morris R (1983) A Study of the Natural History of Back Pain: Part I Development of a Reliable and Sensitive Measure of Disability in Low-Back Pain. Spine 8(2): 141-144.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results