Post-Traumatic Hip with Obturator Dislocation: Case Report and Review of the Literature
Introduction: Traumatic dislocation of the coxofemoral joint is defined as the permanent posterior or anterior displacement of the femoral head out of the acetabular cavity. It is generally the consequence of a violent trauma, most often an accident on the public road. our case it is a post-traumatic hip obturator dislocation, managed in our department. Clinical case and results: 16 years old patient, with no particular history, victim of a road accident, causing a closed trauma to his left hip, right ankle and left wrist. It presents with a vicious attitude: left lower limb in flexion, abduction, external rotation. An X-ray requested objective obturator dislocation with a small bone fragment of the head. A bone reconstruction CT was completed in favour of obturator dislocation with head fracture type 1 according to Pipkin's classification. Patient sent directly to the block, he benefits from a reduction under sedation according to Boehler's maneuver, control by scopy, then immoblisation by zimmer splint after testing the stability of dislocation. Patient is hospitalized in our ward for monitoring then follow-up in consultation. Results were satisfactory, removal of the zimmer splint at the 6th week. Total support was possible at week 12, with complete mobility, patient reviewed afterworld without clinico-radiological signs of aseptic necrosis of the femoral-head. Conclusion: The fracture-luxation of the femoral head is a serious lesion. It is necessary to think about it in front of each dislocation not to ignore the associated fracture which still darkens the prognosis.
Mahfoud M and Saleh Berrada M
Traumatology, Orthopedics surgery Department University Hospital Ibn Sina Rabat,
Morocco
Sina Rabat, Morocco, Tel: 0675668728; Email: krimechomar6@gmail.com without clinico-radiological signs of aseptic necrosis of the femoral-head.
dislocation not to ignore the associated fracture which still darkens the prognosis.
Keywords: Obturator Dislocation; Flexion; Radiography; Ankle; Hip
Introduction
Traumatic dislocation of the coxofemoral joint is defined as the permanent posterior or anterior displacement of the femoral head out of the acetabular cavity. It is generally the consequence of a violent trauma, most often an accident on the public road [1]. Among these anterior dislocations, Epstein and Wiss [2, 3]
distinguish type A, upper or pubic and type B, lower or obturator. De Lee, et al. [4] specified this classification with a type 1, upper with two varieties, one pubic and the other infraspinatus, and a type 2, lower also with two varieties, one obturator and the other perineal. In our case it is a post-traumatic hip obturator dislocation, managed in our department.
Case Report
Observation
This is a 16 years old patient, with no particular history, victim of a road accident, motorcyclist hit by a car, causing a closed trauma to his left hip, right ankle and left wrist. It's routed directly to the ER. An X-ray of the pelvis not done. Patient out with right ankle brace for ankle sprain. Patient still suffering from hip pain re-consults 3 days after the accident.
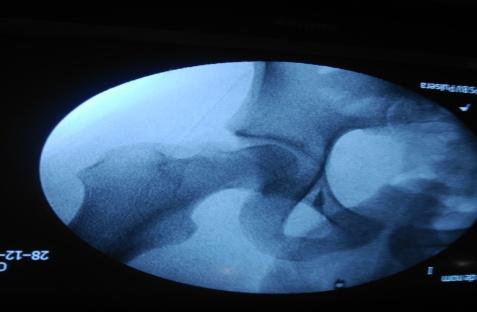
It presents with a vicious attitude: left lower limb in flexion, abduction, external rotation. An X-ray requested objective obturator dislocation with a small bone fragment of the head. A bone reconstruction CT was completed in favour of obturator dislocation with head fracture type 1 according to Pipkin's classification. Patient sent directly to the block, he benefits from a reduction under sedation according to Boehler's maneuver, control by scopy, then immoblisation by zimmer splint after testing the stability of dislocation. Patient is hospitalized in our ward for monitoring then follow-up in consultation.
Results were satisfactory, removal of the zimmer splint at the 6th week. Total support was possible at week 12, patient reviewed afterworld with complete mobility and without clinico-radiological signs of aseptic necrosis of the femoral-head.


Discussion
Very little work has been done on traumatic obturator dislocations (2). Percentage of obturator dislocations reported in traumatic dislocation series is between 6 % and 10 %.
It is common experience in hip replacement surgery that hip flexion and an external rotation and adduction force to the femur produces anterior hip dislocation after capsulotomy in patients who are anesthetized. Whether this is the mechanism during a road traffic accident is not known. The strong anterior capsule or Y shaped ligament of Bigelow is a strong disincentive to anterior dislocation, which may be part of the reason that this pattern of dislocation is less common. The anterior lip fracture may be produced as a result of the ligament or capsule failing to yield and causing an avulsion fracture. Inferior dislocation occurs when the hip is forced into abduction and external rotation [5, 6].
Anterior capsular lesions (tearing or disinsertion) are constant. Associated osteoarticular lesions are frequent, foremost among which are cephalic osteochondral fractures [5], attributed to an impact of the femoral head on the lower part of the anterior acetabular blade. Fracture of the anterior acetabular blade is also possible other lesions have been reported: fracture of the ilio and ischio-pubic branches, contralateral hip dislocation, femoral fractures, neck, shaft and major trochanter. Lesions of the femoral vessels and the femoral nerves or obturator must be sought systematically, even if they are rare. Initial management involves an attempt at orthopedic reduction under general anesthesia with complete muscle relaxation, with the particularity of: the difficulty of reduction and the risk of iatrogenic fracture [2].
Consequences after reduction orthopaedic or surgical procedures are not consensual. Currently there is no scientific argument to justify the interest of traction and unloading in the reduction of the risk of cephalic necrosis of the femoral head. Catonné et al recommend early support relieved and then total support at j15 with eviction of external rotation for 3 weeks as part of the previous dislocations [7]. The risk of necrosis occurring increases with reduction delay. This risk and the 30% in adults. Hoogard observed 47% necrosis when the reduction time exceeded 6 hours. But these figures are mostly lesions associated with fractures of the acetabulum or femoral head, this rate is certainly lower in isolated dislocations [8].
In 1957, Pipkin42 established a four-stage classification that often referred to. In 2001, Yoon57 described a classification that is simpler to understand based on the anatomical description of the lesions and which presents therapeutic implications that should impose it as a reference classification [1]. The publications dealing with femoral head fractures are rare and the series are short, it is difficult to identify a univocal therapeutic strategy.
Conclusion
The fracture-luxation of the femoral head is a serious lesion. It is necessary to think about it in front of each dislocation not to ignore the associated fracture which still darkens the prognosis.
References
-
Burdin G Traumatic hip dislocation: pure dislocation and femoral head fractures.
-
Boyer P, Bassaine M, Huten D (2004) Traumatic obturator foramen hip dislocation review: a case report and of the literature. Rev Chir Orthop Reparatrice Appar Mot 90(7): 673-677.
-
Epstein HC, Wiss DA (1985) Traumatic anterior dislocation of the hip. Orthopedics 8(1): 130-134.
-
Delee JC, Evans JA, Thomas J (1980) Anterior dislocation of the hip and associated femoral-head fractures. J Bone Joint Surg 62(6): 960-964.
-
Vielpeau C, Lanoe E, Delbarre JC, Hulet C (2000) Fractures dislocations of the femoral head. Ann Orthop West 32: 61-65.
-
Phillips AM, Konchwalla A (2000) The pathologic features and mechanism of traumatic dislocation of the hip. Clinical Orthopaedics and Related Research 377: 7-10.
-
Catonné Y, Meyer A, Sariali E, Biette G (2009) Pathologie du complexe pelvi-fémoral du sportif. Pathologie du complexe pelvi-fémoral du sportif 88: 99.
-
Elouakili, Issam, Younes Ouchrif, Redouane Ouakrim, Omar Lamrani, et al. (2015) Luxation obturatrice de la hanche: un traumatisme rare en pratique sportive. Pan African Medical Journal 21: 230.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results