Anterior Maxillary Osteotomy Distraction Osteogenesis (Amodo) in the Treatment of Maxillary Hypoplasia in Unilateral Cleft Lip and Palate-A Case Report
Distraction osteogenesis defines a technique of bone generation by distraction of native bony segments. The technique offers a promising treatment alternative for patients with maxillary or midfacial hypolasia. In this case report, the various steps in the treatment of an 18 year old boy with premaxillary hypoplasia and anterior crossbite are described. Patient was treated with a distraction osteogenesis technique and premaxillary advancement was performed using individual tooth - borne distraction device. The surgical procedure involved an anterior segmental maxillary osteotomy respecting the palatal periosteum. Distractor was cemented in the mouth after the surgical procedures. The patient was observed during a seven day latency period after which the device was activated 0.4mm every 12 hours. The anterior crossbite was eliminated and the occlusal correction and settling was achieved with fixed orthodontic appliances.
Introduction
Maxillary hypoplasia is a common deformity secondary to cleft lip and palate. The correction of this deformity presents a great challenge to the oral and maxillofacial surgeons as well as the orthodontists. The advent of distraction osteogenesis has been a promising alternative for patients with maxillary or midfacial hypoplasia secondary to cleft lip and palate. Distraction osteogenesis (DO) was first described by Ilizorov in Russia in the 1950s and Cohen, et al. were the firsts to describe mid-facial distraction. Since then, there has been numerous reports of distraction osteogenesis at this level. There are different types of distractors based on their site and use like the maxillary or mandibular distractors or the internal and external distractors. The most popular among these is the Hygeinic rapid palatal distractor (HYRAX) [1]. The advantages of distraction osteogenesis over conventional osteotomies includes application at a younger age, lower risk of nerve damage, the displacement of the jaw or parts of the jaw over a greater distance, a better stability of the treatment result, possibility of avoiding bone grafts and availability of space in the arch especially in crowded cases [2]. Additionally, it establishes augmentation of soft tissue simultaneously with bone. Possible complications of the internal distractor includes faulty distraction vectors which could result in an open bite in maxillary anterior distraction and also cause inadequate distraction. However, distraction osteogenesis is being extensively used in cleft cases because of the difficulty in mobilising the maxilla in cleft cases due to the presence of scar tissue from the previous surgical procedures.
Case Report
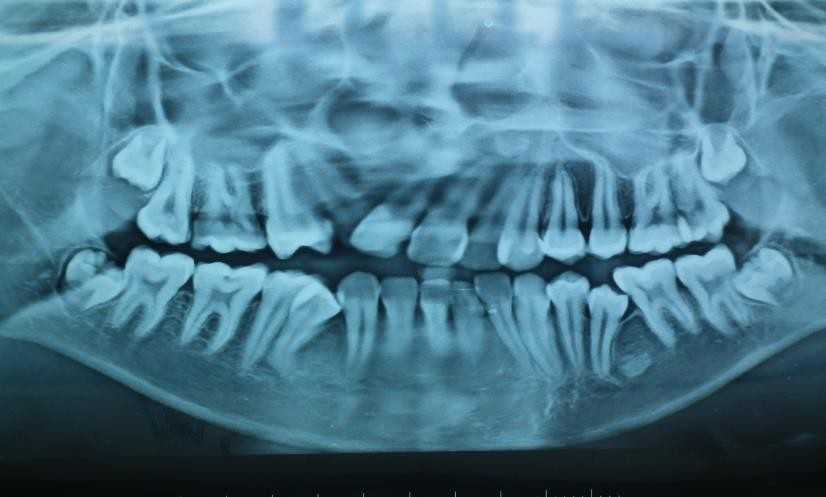
An 18 year old male patient exhibited a skeletal and dental class III malocclusion with maxillary hypoplasia secondary to cleft lip and palate with severe maxillary transverse constriction (Figure 1). Previously, he had undergone primary lip and palate closure surgeries at 9 months and 10 years of age respectively. Intra oral examination revealed an anterior and posterior crossbite, generalised crowding and impacted 35 and missing 12 (Figure 2). Pre treatment cephalometric findings includes a skeletal Class III due to a retrognathic maxilla and an orthognathic mandible with vertical growth pattern.


Treatment Progress
To correct the transverse discrepancy, the quad helix was the choice for expansion since the intention was slow expansion as it was feared that a rapid expansion could gape a fistula in the palate. After initial expansion, a preadjusted edgewise appliance was strapped up (Figure 4).

The upper second bicuspids were extracted to provide space for alignment. Once the arch was expanded and aligned, the distractor was fabricated. The distractor used was a HYRAX maxillary expansion device flipped sagittaly. The surgical procedure consisted of a standard anterior maxillary partial osteotomy and the distractor was cemented on the operating table. The distraction procedure was initiated 7 days after the surgery. The distractor was activated twice per day, half turn in the morning and evening respectively giving a total distraction of 0.8mm/day. The patient was recalled every 3 days and the distraction was continued until a positive overjet was achieved (Figure 5). Post distraction, the distractor was stabilised with acrylic, 8 weeks of consolidation period was maintained and the HYRAX appliance was removed only after callus formation was confirmed on the radiograph.

As the distraction progressed, an open bite developed due to the vector of force of the anterior segment being in the upward and anterior direction. Hence, two bilateral infra zygomatic mini plates were surgically placed to bring about upper posterior teeth intrusion thereby reducing the open bite (Figure 6). This also helped in maintaining the LAFH.

Sufficient space was created for the missing 12 and a riding pontic was placed. In the lower arch treatment progressed with extraction of second bicuspids followed by

arch alignment. Additionally, a vertical reduction genioplasty was also performed to camouflage the Class III tendency and maintain LAFH (Figure 7).
Results
With maxillary advancement, the facial profile improved and an acceptable interincisal relationship was also obtained (Figure 8). The SNA increased from 68.9° to 70.5° and the overjet increased from -2 to 3mm. The maxillary posteriors intruded by about 6mm and the LAFH decreased by 10.4mm with the help of intrusion of posteriors reinforced with infra zygomatic mini plates (Figure 9). The severe crowding, anterior and posterior crossbites and the open bite were corrected and a riding pontic was placed in relation to 12. There was no significant alteration in speech.


Discussion
Advancement of the anterior maxilla is often required for cleft patients to correct the skeletal deformity. But this maxillary anterior advancement by itself is limited because of the palatal and crestal soft tissue constraints. The use of DO has potentially solved this problem by slow bone lengthening along with soft tissue genesis. But the major disadvantage of distraction osteogenesis is the control of the force vectors which effects an upward and forward movement of the anterior segment resulting in an open bite.
This case report demonstrates an increase in the SNA angle with no adverse soft tissue reaction along with correction of a reverse overjet. When a distraction procedure is performed with the distractor placed parallel to the occlusal plane, the vector of forces passes below the centre of resistance of the maxilla which results in a counter clockwise rotation of the maxilla resulting in an anterior open bite. In this case, the open bite due to force vectors of the distraction has been successfully corrected using infra zygomatic mini plates which provided maxillary posterior teeth intrusion and subsequent reduction of the open bite. Similar results were obtained by Shetty et al using a modified Y distractor fabricated from a 15mm hyrax screw rotated 90º. The distractor was cemented into the patient’s mouth by adjusting it parallel to the occlusal plane in close approximation to palatal mucosa. Once the anterior maxilla was completely mobilised, a 16 mm bone screw was passed on each side through the loop-hole fabricated on the appliance. Activation was started three days postoperatively at a rate of 4 turns/day, to achieve a daily movement of about 0.8mm until an over-corrected positive interincisal relation was attained. To counteract the mild anterior open bite (if any) after distraction, anterior box elastics were used [3].
Grayson, et al. [4] advocates the use of intermaxillary elastics during the active distraction phase to modify the force vectors during distraction. Intermaxillary elastics may be worn in Class II, III, vertical or transverse (buccolingual) directions during the active phase of distraction. Anterior vertical intermaxillary elastics may be helpful in the reduction of an anterior open bite and may be used transversely to correct crossbite [4]. Certain authors have also described a skeletal change to intermaxillary elastics used during the active phase of distraction and considers it as the moulding response. This moulding to intermaxillary elastics occurs as the bones on either side of the new bone rotate around the distraction fixation pins. They also advocate the use of intermaxillary elastics during the period of consolidation for skeletal and dental retention in cases where the open bite has been closed [5].
Some authors also suggests the use of 3-D models to perform the model surgery where in the distractors are pre- bent, pre- shaped and activated to full movement so that the vector of distraction can be planned. Once the appliances are activated and perfect occlusion is obtained on the model, the actual surgery can be performed with proper vectors [6].
Conclusion
Distraction osteogenesis is an efficient treatment modality to treat severe midfacial hypoplasia especially those secondary to orofacial clefting and the presence of scaring. It allows gradual advancement of the maxilla along with lengthening of the soft tissue and offers lower relapse rates and serves as a better way to manage patients at a much lower risk and complications associated with orthognathic surgery.
References
-
Maheshwari S Verma SK, Tariq M, Prabhat KC, Kumar S (2011) Biomechanics and orthodontic treatment protocol in maxillofacial distraction osteogenesis. Natl J Maxillofac Surg 2(2): 120.
-
Rachmiel A, Aizenbud D, Eleftheriou S, Peled M, Laufer D (2000) Extraoral vs. intraoral distraction osteogenesis in the treatment of hemifacial microsomia. Ann Plast Surg 45(4): 386-394.
-
Shetty V, Khanum A, Yadav A, Sailer HF (2020) Minimally- invasive anterior maxillary distraction technique in patients with cleft lip and palate and maxillary deficiency: an evaluation of 106 patients. Br J Oral Maxillofac Surg 58(7): 777-783.
-
Grayson BH, Santiago PE (1999) Treatment planning and biomechanics of distraction osteogenesis from an orthodontic perspective. Semin Orthod 5(1): 9-24.
-
Peltomaki T, Grayson BH, Vendittelli BL, Katzen T, McCarthy JG (2002) Moulding of the generate to control open bite during mandibular distraction osteogenesis. Eur J Orthod 24(6): 639-645.
-
Guerrero CA (2016) Maxillary intraoral distraction osteogenesis. Orthognathic Surgery: Principles, Planning and Practice 16: 713-720.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results