A Meta-Analysis of Risk Factors for Stroke after Spinal Surgery
Background: Perioperative stroke is a rare but serious complication of spinal surgery. However, it has been reported that there are multiple risk factors that contribute to postoperative stroke, but still remains controversial. The aim of this study is to investigate the risk factors of stroke after spinal surgery. Methods: A systematic search of relevant articles is published in PubMed, Embase, Web of Science, Cochrane Library and Clinical Trials databases until August 2022. According to the inclusion and exclusion criteria, two reviewers independently performed literature screening, data extraction and quality assessment of the obtained literature. The Newcastle-Ottawa Scale (NOS) score was used for quality assessment, and STATA 16.0 software was used for meta-analysis. Results: A total of 1706 relevant articles were initially identified and 13 articles were finally included in this study for data extraction and meta-analysis. The meta-analysis showed that advanced age, hypertension and diabetes mellitus were the risk factors for stroke after spinal operation. The OR values (95%CI) of these three factors were 3.36 (1.81, 6.24), 1.61 (1.26, 2.06) and 2.07 (1.23, 3.49) respectively. Conclusions: Advanced age, hypertension and diabetes mellitus are the current risk factors for postoperative cerebrovascular accidents (CVA).
Introduction
With the aging process of people, the incidence rate of spinal degenerative diseases is gradually rising [1, 2]. Surgical management should be adopted for the treatment of spinal degenerative diseases when conservative treatment is Essay ineffective for 3 months [3, 4]. Spinal surgery can significantly improve patients’ neurological function and improve their quality of life, so that they can return to normal life as early as possible [5, 6]. However, previous literatures reported that there are many complications (infection, nerve edema, nerve injury, vascular injuries, dural tears, stroke, etc.) after spine surgery [3, 7, 8]. The stroke was one of the most serious postoperative complications, which could affect the surgical effects and even patient’s life. Some literatures have reported that age, hypertension, diabetes mellitus, hyperlipidemia, cerebrovascular disease, etc could affect the incidence of postoperative stroke [9, 10, 11, 12]. However, there still remains controversial [10]. Therefore, the aim of this study is to investigate the risk factors of stroke after spinal surgery.
Materials and Methods
Study selection and inclusion criteria
We conducted a systematic search of the scientific literature on perioperative stroke and performed a meta- analysis of the pooled data from the eligible studies. Case- control studies or cohort studies were searched from PUBMED, EMBASE, Web of Science, Cochrane Library and Clinical Trials independently by two authors. We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines. Taking PubMed as an example, the specific retrieval strategy is shown as follows: ((((((((((((((((((((((Risk Factors[Title/Abstract]) OR (Hazard[Title/Abstract])) OR (dangerous factors[Title/Abstract])) OR (Factor, Risk[Title/Abstract])) OR (Risk Factor[Title/Abstract])) OR (Social Risk Factors[Title/Abstract])) OR (Factor, Social Risk[Title/Abstract])) OR (Factors, Social Risk[Title/ Abstract])) OR (Risk Factor, Social[Title/Abstract])) OR (Risk Factors, Social[Title/Abstract])) OR (Social Risk Factor[Title/Abstract])) OR (Health Correlates[Title/ Abstract])) OR (Correlates, Health[Title/Abstract])) OR (Population at Risk[Title/Abstract])) OR (Populations at Risk[Title/Abstract])) OR (Risk Scores[Title/Abstract])) OR (Risk Score[Title/Abstract])) OR (Score, Risk[Title/ Abstract])) OR (Risk Factor Scores[Title/Abstract])) OR (Risk Factor Score[Title/Abstract])) OR (Score, Risk Factor[Title/Abstract])) AND ((((spin*[Title/Abstract]) OR (cervical[Title/Abstract])) OR (thoracic[Title/Abstract])) OR (lumbar[Title/Abstract]))) AND (((((((((((((((((((((Str okes[Title/Abstract]) OR (Cerebrovascular Accident[Title/ Abstract])) OR (Cerebrovascular Accidents[Title/ Abstract])) OR (CVA (Cerebrovascular Accident[Title/ Abstract]))) OR (CVAs (Cerebrovascular Accident[Title/ Abstract]))) OR (Cerebrovascular Apoplexy[Title/ Abstract])) OR (Apoplexy, Cerebrovascular[Title/Abstract])) OR (Vascular Accident, Brain[Title/Abstract])) OR (Brain Vascular Accident[Title/Abstract])) OR (Brain Vascular Accidents[Title/Abstract])) OR (Vascular Accidents, Brain[Title/Abstract])) OR (Cerebrovascular Stroke[Title/ Abstract])) OR (Cerebrovascular Strokes[Title/Abstract])) OR (Stroke, Cerebrovascular[Title/Abstract])) OR (Strokes, Cerebrovascular[Title/Abstract])) OR (Apoplexy[Title/ Abstract])) OR (Cerebral Stroke[Title/Abstract])) OR (Cerebral Strokes[Title/Abstract])) OR (Stroke, Cerebral[Title/Abstract])) OR (Strokes, Cerebral[Title/ Abstract])) OR (“Stroke”[Mesh])). Literatures were screened independently by two reviewers using uniform inclusion criteria. Any disagreements should be resolved through discussion or with the assistance of a third-party researcher.
The eligibility criteria were specified using the Population, Intervention, Criteria, Outcome and Study design (PICOS) framework. The selected literatures must meet the following conditions: 1) The definition of stroke is “rapidly developing clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent cause other than that of vascular origin.” [13, 14]; 2) The original data should provide OR value and 95% confidence interval (95%CI) or the OR value and 95%CI can be calculated from the data; 3) The summary results can be expressed by corresponding statistical indicators.
Exclusion Criteria
Excluded documents should meet one of the following criteria: (1) animal studies; (2) meta-analysis and reviews; (3) duplicate studies; (4) case reports; (5) articles without available data; (6) unrelated studies.
Methodological quality evaluation. The methodological quality of the included studies was assessed using the Newcastle-Ottawa Scale (NOS) scoring system. The principle of star-setting quantity was used, and the full score is 9 stars.
Statistical Analysis
Stata version 16.0 (Stata Corp LP, College Station, Texas) was used to synthesize, summarize, and evaluate the data. The collected data were tested for heterogeneity and the combined OR value and 95%CI were calculated. To determine heterogeneity across the studies, the I2 Higgins (0–100%) was adopted. The fixed-effect model was used for meta- analysis when the heterogeneity statistic I2 is less than 50%. In the meanwhile, the random-effect model was applied when the heterogeneity statistic I2 is greater than or equal to 50%. The Egger’s and Begg’s test was used to analyze potential publication bias when the number of articles included was more than 3. Sensitivity analysis was used to test the stability of meta-analysis results: (1) comparison of results between random effect model and fixed effect model; (2) When the number of included literatures is more than 3, the points with significant deviation from 95%CI in the funnel chart are excluded for meta-analysis, and the results are compared with those when all the literatures are included. The p value for statistical significance was set at <0.05.
Results
Study selection
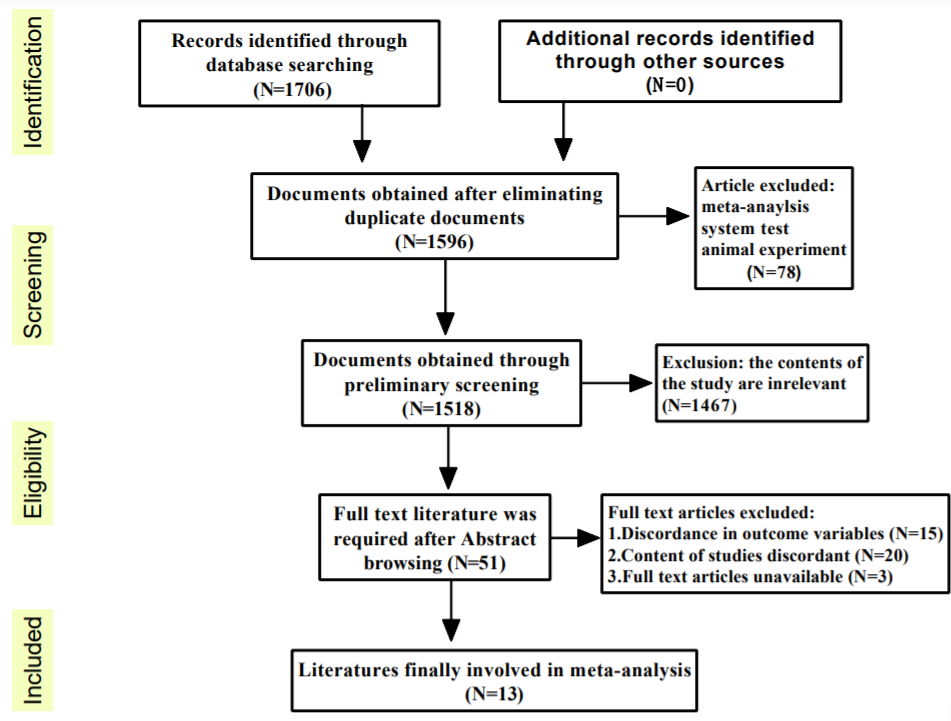
According to the search terms of the literature, a total of 1706 relevant articles were initially identified. Of those articles, 110 were duplicated in databases. After screening the remaining 1518 articles using titles and abstracts, most of the studies were excluded because they were not relevant to the objectives of this study (1467), meta-analysis and reviews (78). After reading the full text of the remaining 51 articles, a total of 38 were excluded due to the inability to obtain the full text (3), the outcome variables did not match (15), research content does not meet inclusion standards (20). Finally, 13 articles were included in this study for data extraction and meta-analysis (Figure 1).
Study characteristics
The eligible studies included 6 retrospective studies and 7 case-control study. The highest NOS score was 8 and the lowest was 5. A total of 415191 patients were included in the study. The basic characteristics and NOS scores of the included studies are shown in Table 1.
Meta‑analysis
According to the research contents of the included literature and the number of references for each factor, four risk factors including advanced age, hypertension, diabetes mellitus and cerebrovascular events were selected for meta- analysis.
Advanced age
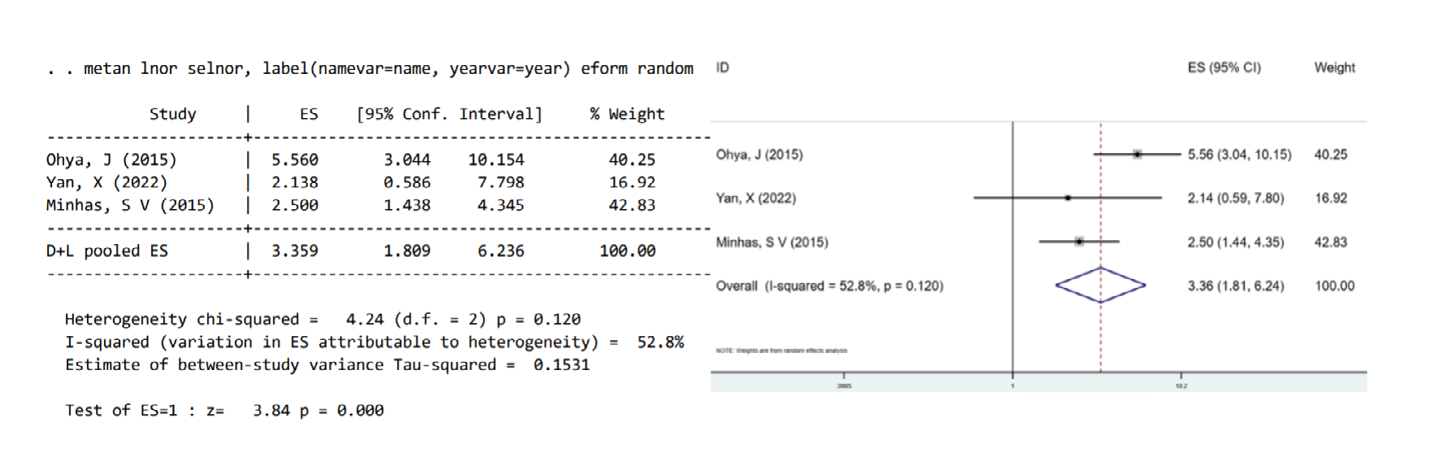
Assuming advanced age as an independent factor, the results of meta-analysis using a random effect model showed that advanced age had a strong correlation with the cerebrovascular accidents (CVA) postoperatively [combined OR values=3.36, 95%CI (1.81, 6.24), P<0.05, Figure 2]. Furthermore, mild heterogeneity was found among the studies (I2= 52.8%, P=0.12, Figure 2). After analyzing the original research, we guessed that the reasons for the mild heterogeneity might be as follows: 1. Different literatures have different definitions of advanced age (advanced age is defined as ≥65, 75 or 80, respectively); 2. The participants were ethnically diverse [9, 10, 12].
Hypertension
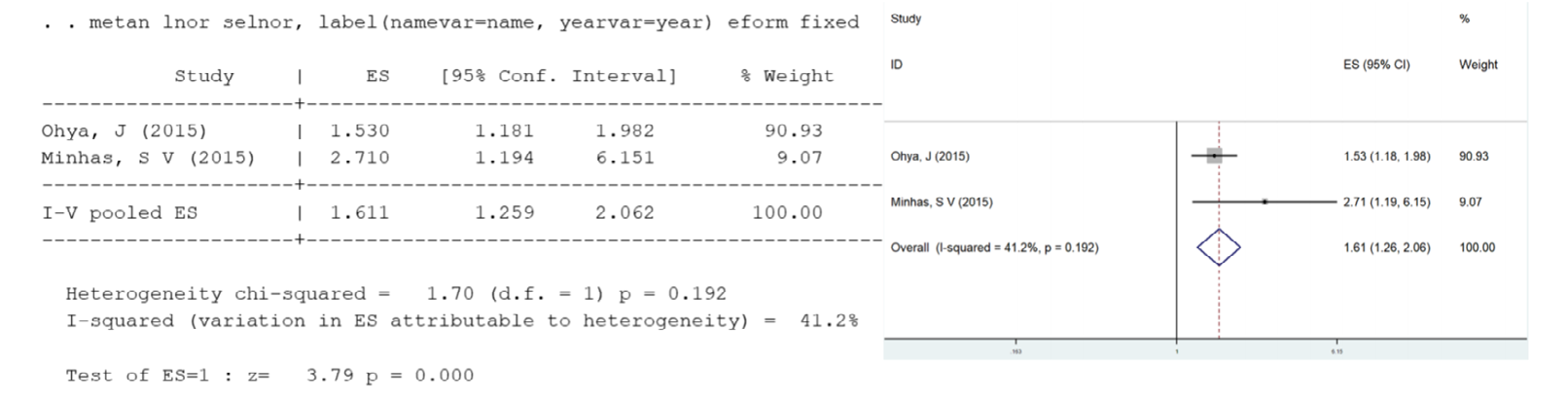
Two studies reported that the OR value between hypertension and perioperative stroke was 1.61[95%CI (1.26, 2.06)], and there was no heterogeneity between studies (I2=41.2%, P=0.192, Figure 3) [10, 12]. The forest plot between hypertension and perioperative stroke is also shown in Figure 3.
Diabetes mellitus
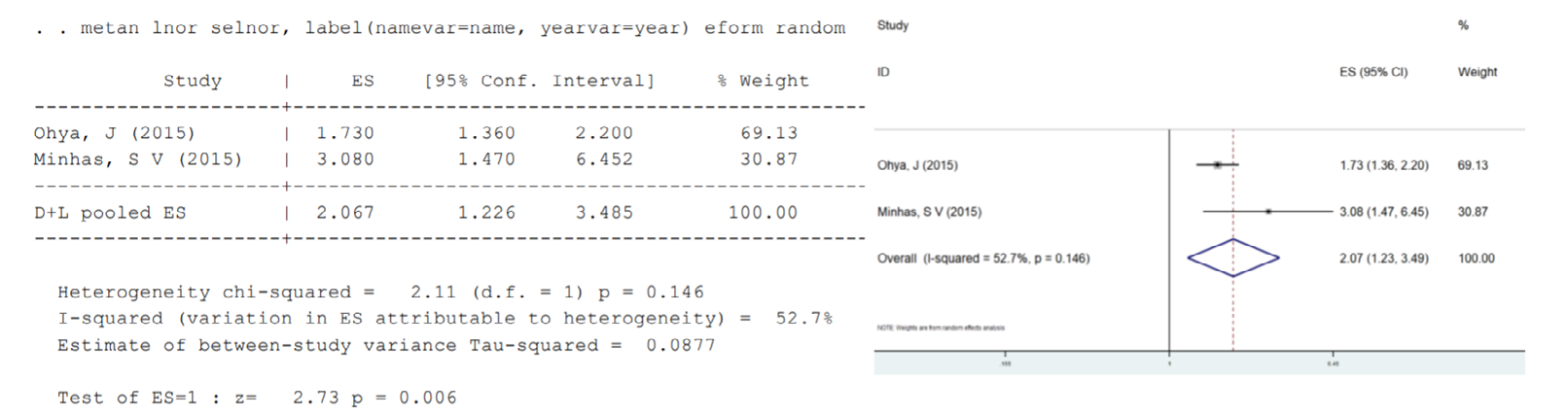
Meta-analysis of the two included studies using random effect model showed that diabetes mellitus had a significant effect on the perioperative stroke after spine operation [OR=2.07, 95%CI (1.23,3.49), P=0.006, Figure 4 and mild heterogeneity was observed between the two studies (I2=52.7%, P=0.146) [10, 12].
Cerebrovascular events
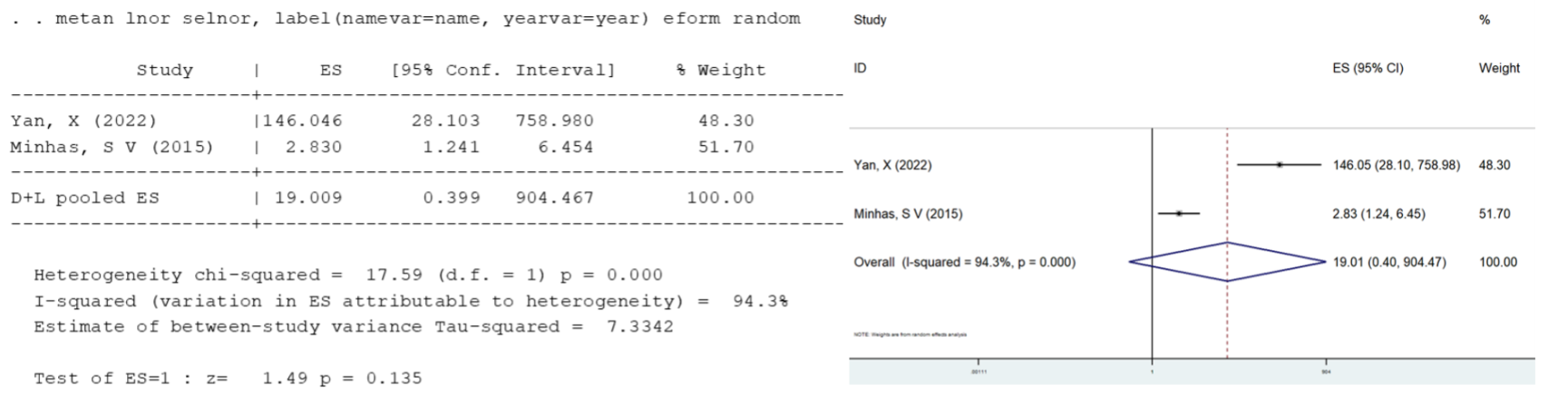
Two studies reported the relationship between cerebrovascular events and postoperative cerebrovascular accidents [9, 12]. There was great heterogeneity among these studies (I2=94.3%, P<0.01), therefore we abandoned the meta-analysis of cerebrovascular events as a risk factor for stroke after spinal surgery due to strong heterogeneity (Figure 5). We hypothesized that the strong heterogeneity may be due to the inclusion of both stroke history and transient ischemia (TIA) as cerebrovascular events.
Publication bias analysis
Using advanced age as indicators to detect publication bias, the Egger’s and Begg’s test results of advanced age were 0.834 and 1.000 respectively. The p value is greater than 0.05, indicating that there is little possibility of publication bias in this meta-analysis.
Discussion
This study systematically collected the studies on the risk factors of postoperative stroke after spine surgery. A total of 13 literatures were included, which clearly specified the inclusion and exclusion criteria. The statistical methods were correctly used, and the literatures quality was relatively high (all≥5 stars). Therefore, the meta-analysis results have high reliability, which showed that the advanced age, hypertension and diabetes mellitus were related to the perioperative stroke. However, cerebrovascular diseases are highly heterogeneous as risk factors for postoperative stroke. The strong heterogeneity might be due to the fact that both stroke history and transient ischemia (TIA) were included in cerebrovascular events.
Perioperative stroke is a relatively rare disease9, and there are not many literatures reported on it in clinical practice, even fewer literatures meeting our inclusion criteria. Older age, hypertension, and diabetes have been reported in two or more literatures as risk factors. However, coagulation abnormalities, history of heart disease, operation time, length of hospital stay, OPLL, COPD, and stroke history, etc cannot be included in the meta-analysis due to the lack of sufficient original studies [9, 10, 11, 12, 15, 16]. This meta-analysis showed that advanced age, hypertension and diabetes mellitus are risk factors for stroke after spinal operation.
As one of the risk factors, old age has been reported in three literatures, with OR values of 5.56, 2.138 and 2.5 respectively. The elderly, as a predisposed group for the disease, often present with other basic diseases and are at high risk of developing postoperative stroke [17, 18]. In addition, it has been reported that increasing age is associated with atherosclerosis. Old age was the most robust risk factor for subclinical atherosclerosis [19]. Patients with diabetes exhibit accelerated progression of carotid intima–media thickness and atherosclerotic plaque formation, and are prone to occlusive disease affecting small penetrating arteries in the brain [20]. Furthermore, diabetes increases cerebral edema, neovascularization, and protease expression that may damage endothelial integrity [21]. All these mechanisms may lead to the occurrence of stroke. In addition, Chronic hypertension may lead to stroke through injury of endothelial cells and thickening of smooth muscle cell [22]. These changes likely impair blood flow autoregulation and contribute to the increased infarct size after vessel occlusion [23].
For cerebrovascular events, this meta-analysis combined TIA with stroke as cerebrovascular events and found that there was extremely strong heterogeneity. We speculate that the possible reason is that TIA and stroke have different definitions. Transient ischemic attack, as a warning event for future stroke, is a less severe disease. However, according to previous literatures, both TIA and stroke can increase the incidence of postoperative stroke after the spinal operation (OR=2.83, 146.046 respectively) [10, 12]. Therefore, more original studies are required to further investigate the association between history of cerebrovascular disease and stroke after spinal surgery. To our knowledge, this is the first meta-analysis of risk factors for stroke after spinal surgery. Chronic diseases such as diabetes, hypertension, or advanced age may have increased vascular fragility, which in turn makes the probability of stroke increasing. However, more original studies were required to further investigate the association between the above risk factors and stroke after spinal surgery in the future.
Conclusions
Up to now, the risk factors for stroke after spinal surgery are still controversial. This meta-analysis is conducted to investigate risk factors for stroke after spinal operation. The results shows that advanced age, hypertension and diabetes mellitus are the current risk factors for postoperative cerebrovascular accidents. We believe that the results of this study can provide clinical reference for the risk factors of stroke after spinal surgery.
| Author, year | Study design | Date of data collection | Sample(N) | Mean age (years) | Male (N or %) | risk factors | Statistical method | NOS scores |
|---|---|---|---|---|---|---|---|---|
| Bronheim, R S 2018 | retrospective study | 2006-2013 | 9295 | 61.01 | 4146 | 1. coagulopathy | Logistic regression analysis | 5 |
| Arrighi- Allisan, A E 2020 | retrospective study | 2008-2016 | 3226 | 63.1 | 1534 | 1. diabetes mellitus (P=0.576) | Logistic regression analysis | 7 |
| Wu, J C 2012 | Prospective study | 2004-2007 | 30866 | 40.48±12.74 | 76.40% | 1. spinal cord injury | Logistic regression analysis | 6 |
| Huang, L C 2015 | Prospective study | 2000-2009 | 13503 | 67 | 5099 | 1. spinal surgery | Logistic regression analysis | 6 |
| Wu, J C 2012 | Prospective study | 2000-2005 | 18135 | 57.9 | 10576 | 1. spinal surgery | Logistic regression analysis | 7 |
| Labaran, L A 2019 | retrospective study | 2006-2013 | 30547 | unknown | 19020 | 1. polycythemia vera (P=0.580) | Logistic regression analysis | 5 |
Table 1: Characteristics and quality evaluation of the included studies. Legend: The basic characteristics and NOS scores of the
1. age (≥80)
2. heart disease
3. diabetes mellitus
- Ohya, J 2015 retrospective study
- 2007-2012
- 167106 unknown
- 98445
- Yan, X 2022 retrospective study
- 2015-2021
- 17408 unknown
- 8586
- Shin, J 2019 retrospective study
- 2002-2015
- 7450 unknown
- 3810
- 1. OPLL
- Logistic regression analysis
- 5
- Lin, S Y
- 2018
- Prospective study
- 2000-2010
- 27990
- 54.9±13.4
- 11423 1. cervical spondylosis
- Arena, P J
- 2020
- Prospective study
- 2007-2018
- 43063 unknown
- 20563 1. diabetes mellitus Logistic regression analysis
- 7
- 2. stroke history
- Wu, J C 2012 Prospective study
- 2000-2005
- 4452 unknown
- 1793
- 1. spinal surgery
- (P=0.522)
- Minhas, S V
- 2015 retrospective study
- 2006-2012
- 42150 unknown
- 16779
- 6. COPD
Table 2: Characteristics and quality evaluation of the included studies.
- Declarations Ethics approval and consent to participate: Not applicable Consent for publication: Not applicable Availability of data and materials: The datasets of the current study are available from the corresponding author upon reasonable request Competing interests: The authors declare that they have no competing interests
- Funding There is no source of funding for research and/or publication
- Authors’ contributions HY designed this study. LX analyzed the data and drafted the paper. ZT, SH revised the manuscript. SH provided critical comments on this draft. All authors read and approved the final manuscript.
- Acknowledgements Not applicable
References
-
Aizawa T, Kokubun S, Ozawa H (2016) Increasing Incidence of Degenerative Spinal Diseases in Japan during 25 Years: The Registration System of Spinal Surgery in Tohoku University Spine Society. ohoku J Exp Med 238(2): 153-163.
-
Wu PH, Kim HS, Jang IT (2020) Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. Int J Mol Sci 21(6): E2135.
-
Christensen FB, Bünger C (2004) Stabilisation surgery for chronic low back pain: indications, surgical procedures, and outcome. Scand J Rheumatol 33(4): 210-217.
-
van den Eerenbeemt KD, Ostelo RW, van Royen BJ, Peul WC, van Tulder MW (2010) Total disc replacement surgery for symptomatic degenerative lumbar disc disease: a systematic review of the literature. Eur Spine J 19(8): 1262-1280.
-
Yorimitsu E, Chiba K, Toyama Y, Hirabayashi K (2001) Long-term outcomes of standard discectomy for lumbar disc herniation: a follow-up study of more than 10 years. Spine (Phila Pa 1976) 26(6): 652-657.
-
Dewing CB, Provencher MT, Riffenburgh RH, Kerr S, Manos RE (2008) The outcomes of lumbar microdiscectomy in a young, active population: correlation by herniation type and level. Spine (Phila Pa 1976) 33(1): 33-38.
-
Rajaee SS, Kanim LEA, Bae HW (2014) National trends in revision spinal fusion in the USA: patient characteristics and complications. Bone Joint J 96-B(6): 807-816.
-
Coe JD, Smith JS, Berven S, Arlet V, Donaldsonet W, et al. (2010) Complications of spinal fusion for scheuermann kyphosis: a report of the scoliosis research society morbidity and mortality committee. Spine (Phila Pa 1976) 35(1): 99-103.
-
Yan X, Pang Y, Yan L, Ma Z, Jiang M, et al. (2022) Perioperative stroke in patients undergoing spinal surgery: a retrospective cohort study. BMC Musculoskelet Disord 23(1): 652.
-
Ohya J, Chikuda H, Oichi T, Horiguchi H, Takeshita K, et al. (2015) Perioperative stroke in patients undergoing elective spinal surgery: a retrospective analysis using the Japanese diagnosis procedure combination database. BMC Musculoskelet Disord 16: 276.
-
Arena PJ, Mo J, Sabharwal C, Begier E, Zhou X, et al. (2020) The incidence of stroke among selected patients undergoing elective posterior lumbar fusion: a retrospective cohort study. BMC Musculoskelet Disord 21(1): 612.
-
Minhas SV, Goyal P, Patel AA (2016) What are the Risk Factors for Cerebrovascular Accidents After Elective Orthopaedic Surgery. Clin Orthop Relat Res 474(3): 611- 618.
-
Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors JJB, et al. (2013) An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 44(7): 2064-2089.
-
Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, et al. (1980) Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ 58(1): 113-130.
-
Bronheim RS, Oermann EK, Cho SK, Caridi JM (2017) Coagulation Profile as a Risk Factor for 30-Day Morbidity and Mortality Following Posterior Lumbar Fusion. Spine (Phila Pa 1976) 42(12): 950-957.
-
Shin J, Choi JY, Kim YW, Chang JS, Yoon SY (2019) Quantification of Risk Factors for Cervical Ossification of the Posterior Longitudinal Ligament in Korean Populations: A Nationwide Population-based Case- control Study. Spine (Phila Pa 1976) 44(16): E957-E964.
-
Chivite D, Formiga F, Corbella X (2018) Basal functional status predicts one-year mortality after a heart failure hospitalization in elderly patients - The RICA prospective study. Int J Cardiol 254: 182-188.
-
Izawa S, Enoki H, Hirakawa Y, Iwata M, Hasegawa J, et al. (2010) The longitudinal change in anthropometric measurements and the association with physical function decline in Japanese community-dwelling frail elderly. Br J Nutr 103(2): 289-294.
-
Lim S, Choi HJ, Shin H, Khang AR, Kang SM, et al. (2012) Subclinical atherosclerosis in a community-based elderly cohort: the Korean Longitudinal Study on Health and Aging. Int J Cardiol 155(1): 126-133.
-
Haratz S, Tanne D (2011) Diabetes hyperglycemia and the management of cerebrovascular disease. Curr Opin Neurol 24(1): 81-88.
-
Phipps MS, Jastreboff AM, Furie K, Kernan WN (2012) The diagnosis and management of cerebrovascular disease in diabetes. Curr Diab Rep 12(3): 314-323.
-
Veglio F, Paglieri C, Rabbia F, Bisbocci D, Bergui M, et al. (2009) Hypertension and cerebrovascular damage. Atherosclerosis 205(2): 331-341.
-
Ergul A, Hafez S, Fouda A, Fagan SC (2016) Impact of Comorbidities on Acute Injury and Recovery in Preclinical Stroke Research: Focus on Hypertension and Diabetes. Transl Stroke Res 7(4): 248-260.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results