Dramatic Clinical and Ultrasound Outcomes Post Platelet- Rich Plasma for Recalcitrant Chronic Mid-Portion Achilles Tendinopathy: Case Report
Chronic Achilles tendinosis with or without tendon tear is a common form of tendon degenerative pathology that is hard to treat with traditional approaches including oral anti-inflammatory medicine, physical therapy, and shock-wave treatment. corticosteroid injection could lead to tendon rupture, thus if conservative management fails then surgery is a last resort. This article presents a middle-female, who suffered Achilles tendinopathy symptoms for over 20 years, affecting her daily activity and sports life. She had tendon nodule clinically. Ultrasound scan (USS) showed diffuse thickening of the Achilles tendon at the mid-portion of the maximal sagittal diameter of 10 mm without a tendon tear. She failed conservative management, physiotherapy, and shock wave therapy. She elected for a single trial of investigational USS-guided platelet-rich plasma (PRP) therapy. She improved gradually by returning to completely normal daily activities and running/sprinting after one year of PRP therapy. Her tendon nodule resolved clinically, and a repeat USS showed reduced diffuse thickening of the Achilles tendon at the midportion of the maximal sagittal diameter down to 7mm suggestive of the healing process. Thanks to the regenerative restoration power of the growth factors and signalling proteins in platelets that stimulate the internal mesenchymal stem cells to promote the healing process. We recommend a comprehensive randomized control trial to approve those findings and standardization of the PRP technique, trusting regenerative medicine to develop as a mainstream therapy in several musculoskeletal pathologies, particularly in degenerative conditions and resistant injuries.
Introduction
The term tendinopathy in general could be either tendinitis or tendinosis. Tendinitis means tendon inflammation develops from micro-tears after sudden overloading force, though research frequently reported what is presumed to be tendinitis is commonly tendinosis [1, 2, 3].
Tendinosis is a degeneration of the collagen in response to recurring injuries and chronic overuse, this process arises because not enough rest for the tendon to heal. The wear and tear changes lead to an increase in the tendon bulk and loss of muscle strength, both contribute to the cycle of injury and can set the phase for secondary tendinitis and nerve impingement [4].
Current clinical tradition is the use of oral nonsteroidal anti-inflammatory drugs (NSAIDs) while this is helpful in tendinitis, it has been found not helpful for tendinosis as it hinders collagen repair [5]. The treatment of Achilles Tendinopathy (AT) is a substantial challenge for sports medicine physicians and orthopaedic surgeons making it not always possible to achieve a noble outcome. Conservative therapy with rehabilitation and shockwave therapy options are the standard practice [6, 7, 8]. Glucocorticoid injections are potentially harmful, and we should avoid them [9]. Open or arthroscopic surgical procedures for the treatment of AT involve incising the para-tendon and removing adhesions, followed by debridement of macroscopically degenerated tissue, to promote a repair response [10]. The local administration of growth factors, in particular, platelet- derived growth factors is an emerging treatment strategy which aims at providing a regenerative stimulus in a tissue to provide a local regenerative stimulus for tendon healing [11, 12, 13, 14, 15, 16, 17]. In this article, we have treated our patient with PRP for recalcitrant AT.
Case Report
Middle age lady presented with a 25-year history of right Achilles tendon (AT) pain with loss of ability to run or sprint, she started to develop more regular flare-ups in the last five years with ongoing pain with visual analogue score (VAS 0-10; 0=no pain and 10=worst pain) was 4/10 during rest and up to 8/10 during activities and flare-ups, limping, stiffness and swelling (nodule) at the mid-portion of the AT, the swelling increases when try to play touch rugby and running. She struggled to look after her dogs and lost her loved sports life.
She failed all kinds of conservative management including heal raise, rehabilitation using resistance and eccentric/concentric exercise. She also failed insoles, ankle support and shock wave therapy.
She searched for investigational therapy with platelet- rich plasma (PRP), after assessment in June 2022 she was referred for an ultrasound scan at the radiology department, which showed diffuse AT with thickening with the maximal sagittal diameter of 10 mm at the mid-portion but no tear or calcification. There is an echogenic appearance of the soleus muscle in keeping with some fatty atrophy.
At the end of June 2022, she underwent the PRP procedure in an office-based clinic after informed consent and using aseptic technique under local anaesthesia with Ropivacaine 0.2 % was injected under the skin and subcutaneous tissues in but not in the para-tendon or the tendon itself to avoid reduction of the PRP effectiveness, 30 ml of blood was withdrawn and placed in ACD-AC tubes in a centrifuge for 9 minutes, 7 ml of PRP was extracted. The procedure was performed under Sonosite ultrasound-guidance using a linear probe 10-5 MHz. Using lateral approach, we injected 2 mls in the paratenon area and 5 mls intra-tendinous. As in Figures 1a & 1b and Video 1 (https://medwinpublishers. com/articlevideos/jobdarticle.php).
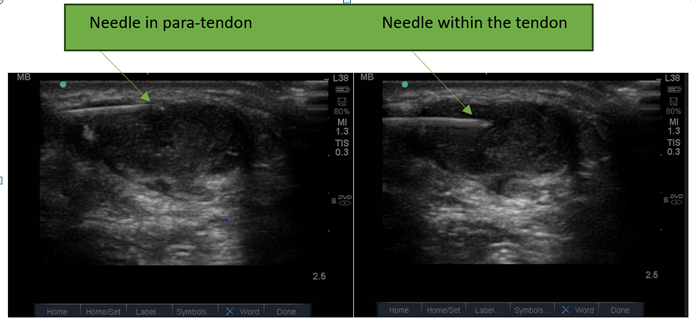
Figure 1a: Para-Tendon PRP Injection. Figure 1b: Intra-Tendinous PRP Injection.
Post-Procedure is as follows
- During first 3 months: Pain score was 7, swelling after initial treatment, stiffness and limping increased from original symptoms, not able to run at all. She couldn’t wear high heels.
- At 6 months her Pain score was 3, swelling greatly reduced, but still tender to touch, stiffness and limping decreased from original symptoms. Able to run, but not sprint and her ankle did not feel stable.
- After 12 months the VAS was zero for pain, no swelling (resolved nodule), stiffness or limping at all. Good stability, able to sprint, can run downstairs comfortably for the first time after 25 years of suffering.
After one year repeat ultrasound at the same radiology department revealed a significant reduction of the diffuse AT with thickening with a maximal sagittal diameter of 7 mm at the mid-portion with no tear, see Figure 2a (baseline USS) and Figure 2b (USS after the PRP therapy).
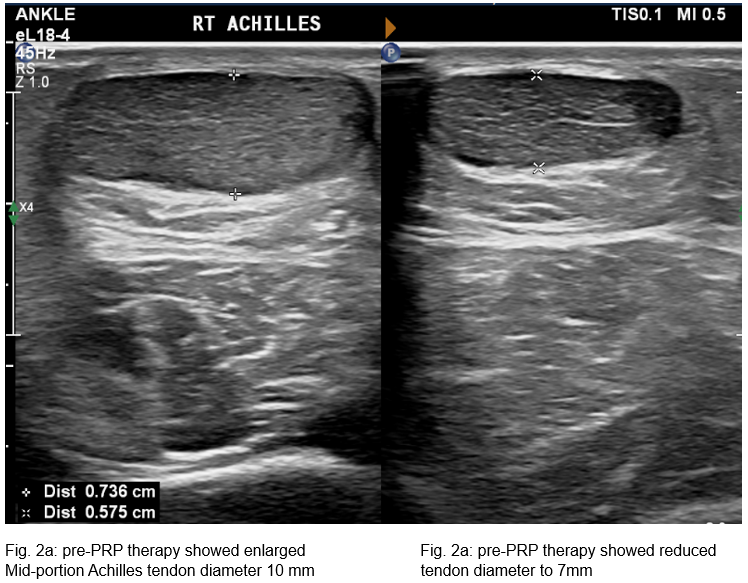
Figure 2a: Baseline USS. Figure 2b: USS after the PRP therapy.
Discussion
The common practice for managing Achilles tendinopathy (AT) is oral anti-inflammatory medicine, physiotherapy, proper insoles, and shockwave therapy. Repeatedly doctors are treating all cases as tendinitis and assuming the inflammatory process is the main issue thus NSAIDs are used.
Many injuries frequently assumed to be tendinitis are tendinosis. Chronic AT is typically described as mid-portion tendinopathy for more than 3 months. It is hard to treat as some degree of collagen degeneration with the wear and tear process [4].
Excessive and/or repetitive stretchable forces on the tendon are likely what triggers the degenerative process associated with tendinosis [18]. Debridement surgery can be used but it should be the last resort.
Our patient had a superior clinical response to a single PRP therapy for the AT although the response was slow, it has resolved her symptoms which have been bothering her for over 20 years affecting her daily activities and sports life. She regained her ability to sprint and run with clinical resolution of the tendon nodule and ultrasound evidence of a reduction in the mid-portion tendon swelling by 3 mm. She was thrilled with the outcome. This procedure can also be repeated safely if needing a booster dose.
Even though PRP is currently not funded by several insurance companies, but we intend and hope this will change soon given it is inexpensive, simple to do, safe with minimal adverse effects, and a far better option than invasive surgery.
Conclusion
We hypothesize the use of single platelet-rich plasma therapy has resulted in the resolution of debilitating symptoms of Achilles tendinopathy, improved quality of life, and evidence-based tendon healing and aborting most of the inflammation on ultrasound scan. This is a simple cost- effective approach worth trying, it could save people from prolonged rehabilitation programs and invasive surgery. However, we need to confirm those findings are consistent in wide randomized controlled trials.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images or videos. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing Interests
The authors declared no conflicts of interest.
Acknowledgments
I would like to acknowledge my wife Zahraa for encouraging me to perform investigational therapy and helping me with the paperwork.
References
-
Kraushaar B, Hirschl RP (1999) Current concepts review - tendinosis of the elbow (Tennis Elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J Bone & Joint Surg 81(2): 259-278.
-
Khan KM, Cook JL, Kannus P (2002) Time to abandon the “tendinitis” myth: Painful, overuse tendon conditions have a non-inflammatory pathology. BMJ 324(7338): 626-627.
-
Khan KM, Cook JL, Taunton JE, Bonar F (2000) Overuse tendinosis, not tendinitis—Part 1: A new paradigm for a difficult clinical problem. Physician Sportsmed 28(5): 38-48.
-
Bass E (2012) Tendinopathy: Why the Difference Between Tendinitis and Tendinosis Matters. Int J Ther Massage Bodywork 5(1): 14-17.
-
Tsai WC, Tang FT, Hsu CC (2004) Ibuprofen inhibition of tendon cell proliferation and upregulation of the cyclin kinase inhibitor p21CIP1. J Orthop Res 22(3): 586-591.
-
Malliaras P, Barton CJ, Reeves ND, Langberg H (2013) Achilles and patellar tendinopathy loading programmes: a systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Med 43(4): 267-286.
-
Sussmilch-Leitch SP, Collins NJ, Bialocerkowski AE (2012) Physical therapies for Achilles tendinopathy: systematic review and meta-analysis. J Foot Ankle Res 5: 15.
-
Al-Abbad H, Simon JV (2013) The effectiveness of extracorporeal shock wave therapy on chronic Achilles tendinopathy: a systematic review. Foot Ankle Int 34(1): 33-41.
-
Dean BJ, Lostis E, Oakley T, Rombach I, Morrey ME, Carr AJ (2014) The risks and benefits of glucocorticoid treatment for tendinopathy: a systematic review of the effects of local glucocorticoid on tendon. Semin Arthritis Rheum 43(4): 570.
-
Leadbetter WB, Mooar PA, Lane GJ, Lee SJ (1992) The surgical treatment of tendinitis. Clinical rationale and biologic basis. Clin Sports Med 11(4): 679.
-
Kaux JF, Crielaard JM (2013) Platelet-rich plasma application in the management of chronic tendinopathies. Acta Orthop Belg 79: 10-15.
-
Cole BJ, Seroyer ST, Filardo G (2010) Platelet-rich plasma: where are we now and where are we going?. Sports Health 2(3): 203-210.
-
Kajikawa Y, Morihara T, Sakamoto H (2008) Platelet-rich plasma enhances the initial mobilization of circulation- derived cells for tendon healing. J Cell Physiol 215: 837- 845.
-
Boswell SG, Cole BJ, Sundman EA (2012) Platelet-rich plasma: a milieu of bioactive factors. Arthroscopy 28(3): 429-439.
-
Aspenberg P, Virchenko O (2004) Platelet concentrate injection improves Achilles tendon repair in rats. Acta Orthop Scand 75: 93-99.
-
Virchenko O, Aspenberg P (2006) How can one platelet injection after tendon injury lead to a stronger tendon after 4 weeks? Interplay between early regeneration and mechanical stimulation. Acta Orthop 77(5): 806-812.
-
De Mos M, Van der Windt AE, Jahr H (2008) Can platelet- rich plasma enhance tendon repair? A cell culture study. Am J Sports Med 36(3): 1171-1178.
-
Murrell GA (2002) Understanding tendinopathies. Br J Sports Med 36(6): 392-393.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results