Coronal Plane Alignment of Knee Joint (C.P.A.K.) Classification in Indian Population- Study of A New Classification System in Indian Knees
Background: Distribution of CPAK types in Indian knees will help surgeons better understand management of knee arthritis using concept of Kinematic alignment (K.A.). C.P.A.K. uses a matrix of 9 phenotypes of knees based on arithmetic hip knee ankle angle (aHKA) and Joint Line Obliquity (JLO). Methods: A radiological analysis of 200 healthy knees (HC) and 250 osteoarthritic knees (OC) was done and were classified based on C.P.A.K. classification. Primary outcomes include descriptive analysis of both groups, and comparison between frequencies of types within each group. Results: The commonest CPAK types in Healthy group were type 5, type 2, type 1. For arthritic group, common types in order were type 1, type 4 and type 2. Varus CPAK types (1,4,7) accounted for 34% of HC types while 59% of OC type, with odds of developing osteoarthritis in type 1 CPAK being 2.84 while that for type 4 were 2.02. Out of 450 knees studied 216 (48%) accounted for varus alignment. Conclusion: C.P.A.K. classification can be used to understand the targets for TKR in Indian population. Constitutional varus being commoner in Indian knees (48%) than their western counterparts implies that majority of Indian knees are in constitutional varus dynamics, hence K.A. caters to majority of the population. Arthritic Indian populations are predominantly of types C.P.A.K. 1(34%) and 4(22%). Further research is needed to understand which Indian knee types benefit the most from KA TKR.
Introduction
The goal of Mechanical alignment (MA) during Total knee arthroplasty (TKR) is to attain a ‘neutral limb alignment’ which is a usual dictum followed by knee surgeons. Yet as much as 20% dissatisfaction is reported in literature for postoperative TKR patients [1].
Previous studies have shown that a significant proportion of normal populace i.e., 32% in males and 17% in females are in a state of constitutional varus [2]. When considering Asian population, this proportion of constitutional varus is predicted to be even more [3].
With a dynamic shift in approach towards TKR, from being surgeon driven to being guided by patient profile, attention is now given to the concept of KINEMATIC alignment (KA) wherein constitutional alignment of patient’s original knee prior to onset of arthritic changes, is used as a template for restoration during TKR. KA approach being sounder physiologically for tibiofemoral kinematics, it is associated with superior pain relief, range of motion and richer subjective perception of a normal knee [4]. Optimal knee balance is reported with KA TKR’s owing to better intercompartmental pressure difference post-surgery and lesser soft tissue release or bone recuts needed to achieve the same [5]. Without knowing an individual’s constitutional alignment, replication of native anatomy with KA techniques is not easily achieved. This is complicated by the fact that the native alignment worsens or undergoes a varus shift as arthritis progresses and makes prediction of original native alignment difficult.
A recent CPAK classification holds promise in this regard where concept of Arithmetic Hip Knee Ankle angle (aHKA) and Joint line Obliquity (JLO) is used [6]. Macdessi, et al. [7] in his 2020 study, introduced concept of aHKA and concluded that it is a reliable marker of constitutional knee alignment irrespective of setting in of arthritic knee changes. Similarly, in 2021 JLO was introduced which used clearer terms i.e., apex proximal, apex distal and neutral for joint line orientation concluding the overlapping terminology between Limb Alignment and Joint line [6].
CPAK classification hence developed using JLO and aHKA to create a 3 x 3 matrix to classify knee morphology into 9 phenotypes (Figure 3) which can be used as a target for KA based TKR for that knee. In our study, knees from two separate groups (asymptomatic healthy group VS osteoarthritic group) were distributed into the 9 C.P.A.K. types. The primary aim of the study was to determine the frequency of different types of knee morphology based on CPAK classification in Indian population and to compare the distribution of 9 knee types among healthy and osteoarthritic groups. We also aim to find out the prevalence of constitutional varus in Indian population.
Data from this study can be a precursor for further research in CPAK classification, understanding knee dynamics in Osteoarthritis (OA) and determining which knee types will benefit most likely from KA approach for Indians.
Materials and Methodology
An Observational Cross section study of CPAK types in 450 knees divided in two groups i.e., Healthy knee group (200) and osteoarthritic knee group (250).
Patients (age > 40 years) presenting with complaints suggestive of OSTEOARTHRITIS (OA) knee and with radiographic evidence of Kellgren- Lawrence grade 3/grade 4 formed the Osteoarthritic Cohort (OC). Other healthy volunteers (age 25 to 50 years) presenting to OPD, without any complaint related to lower limb, or any lower limb deformity, LL trauma or any history of lower limb surgical intervention were used as the healthy cohort (HC).
Any patient with history of/known case/diagnosed subsequently of haemophilia/rheumatoid arthritis/ neuromuscular disease/spondyloarthropathy/ skeletal tuberculosis was excluded from study. Any history of surgical intervention involving lower limbs were also excluded. Suboptimal radiographs were also omitted. HC group, patients having asymptomatic knee osteoarthritic changes, or any other lower limb pathology as seen on radiographs were excluded. For OC group any previous history of any intra-articular pathology i.e. Chondromalacia or injury (ACL/ PCL/ Meniscus/Collateral) were all excluded.
Bilateral Lower Limb Standing Scanogram were done for every participant. Using the below mentioned parameters, markings were made on the printed film using marker and scale. Angles were measured using protractor. Scanograms for which films were not available were studied on a digital interface and angles were measured using digital protractor applications. The collected data and measurements were entered in a master chart. GraphPad was used for the analysis of data.
Radiographic parameters (Figure 1) 1. Center of Femoral head- printed template with concentric circles to be used. 2. Center of knee joint- intersection of the midline between the tibial spines and the midline between the femoral condyles and tip of the tibiae is used [6]. 3. Center of the ankle joint- mid-width of the talus to be used [6]. 4. Mechanical femoral axis - line from the center of the femoral head to the center of the knee[6] 5. Mechanical tibial axis - line from the center of the knee to the center of the ankle [6]. 6. lateral distal femoral angle (LDFA) lateral angle formed between the femoral mechanical axis and the joint line of the distal femur [6]. 7. medial proximal tibial angle (MPTA) medial angle formed between the tibial mechanical axis and the joint line of the proximal tibia [6].
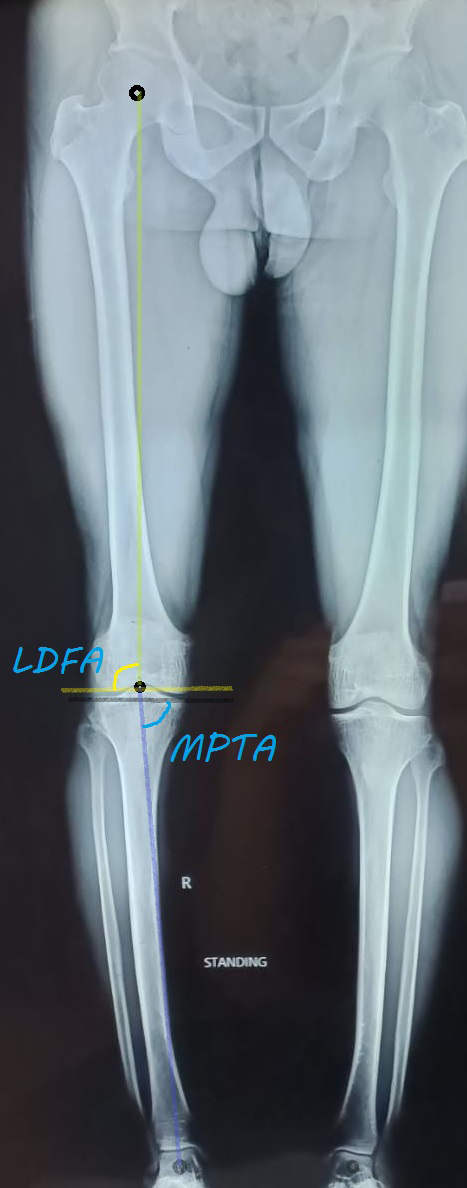
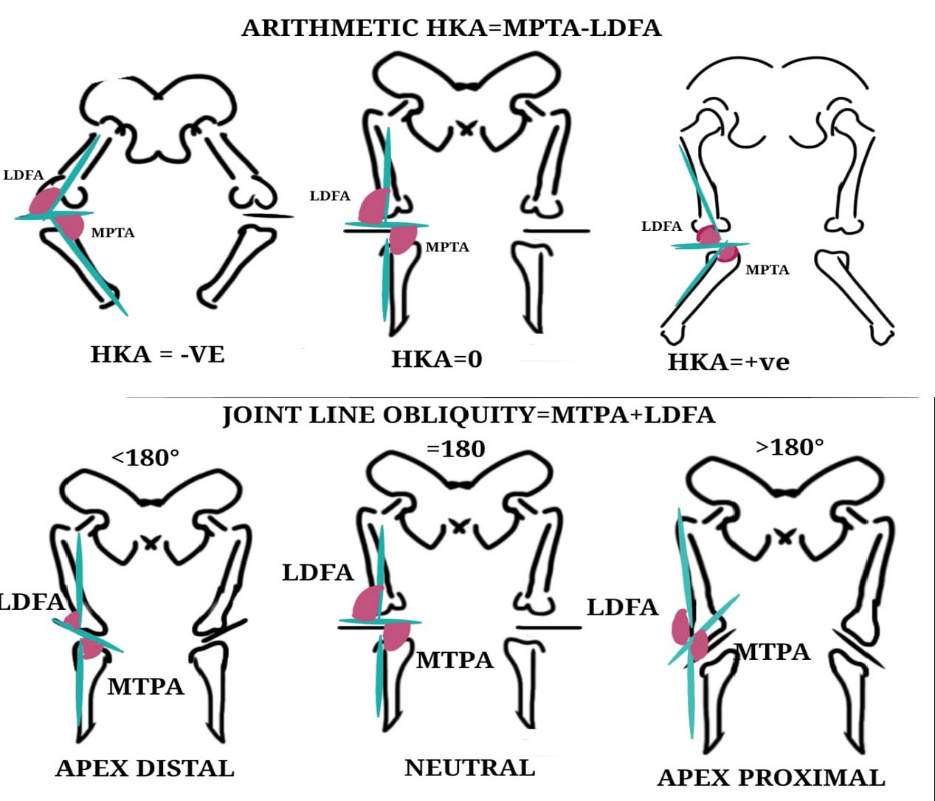
The arithmetic hip knee ankle angle (aHKA) aHKA = MPTA - LDFA. [6] A negative aHKA is considered VARUS type [6] A positive aHKA is considered VALGUS type [6]
The aHKA will be used to determine constitutional alignment [6] (Figure 2).
JLO (JOINT LINE OBLIQUITY) The JLO is independent of the axis of the knee joint.
JLO = MPTA + LDFA [6] joint lines of both knees when extended to the midline is either below, level with, or above the level of a horizontal joint line classifying the knees as ‘apex distal’, ‘neutral’, and ‘apex proximal’ (Figure 2).
The CPAK CLASSIFICATION MATRIX [6] (Figure 3).
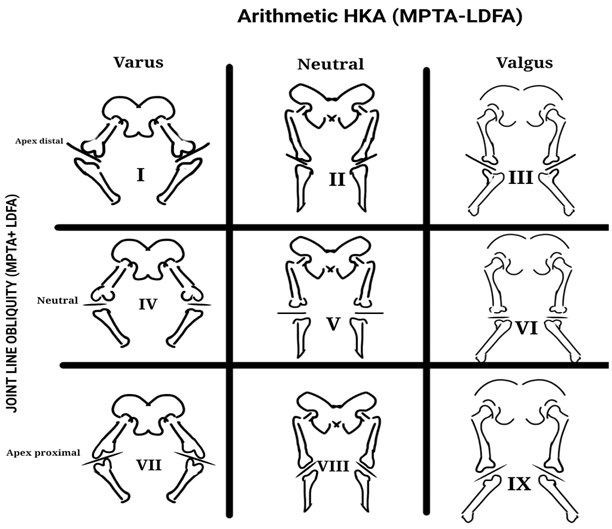
1) cpak boundaries for neutral ahka are 0° ± 2°, inclusive (sd 1.80°). a varus ahka is less than -2°, while a valgus ahka is greater than +2° [6]. 2) cpak boundaries for a neutral JLo are 180° ± 3°, inclusive (sd 2.90°). an apex distal JLo is less than 177°, while an apex proximal JLo is greater than 183° [6].
Results
Mean Age and Gender
A total of 450 knees were studied out of which the HC group consisted of 50% males and 50% females with an average age of 37 (S.D. 8) while the OC group consisted of 59% females and 41% males with mean age of 59 (S.D. 8).
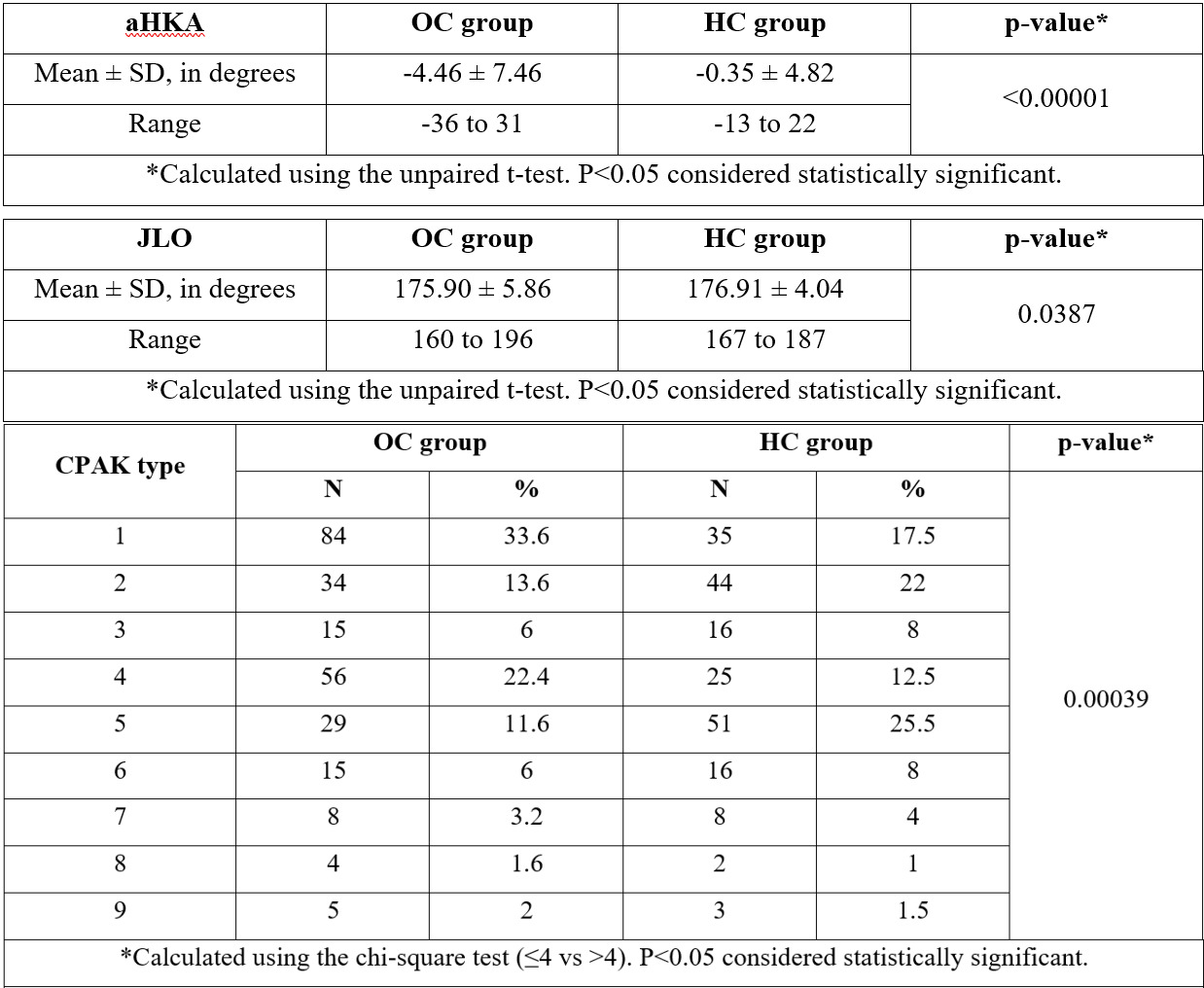
The mean MPTA value for HC group was 88.3 (± 3.07) and was 85.7 (± 4.98) for OC group. The mean LDFA value for HC group was 88.6 (± 3.22) and was 90.2 (± 4.49)for OC group. The Mean aHKA and JLO are briefly described in Figure 5.
Alignment Type
When comparing the alignment alone using aHKA, Varus malalignment accounted for 59% of the OC group as against 31.5% of HC group. Neutral alignment was the commoner alignment seen in healthy group accounting for 51% of HC group. Valgus alignment being least common in both study groups accounted for 13.2 % in OC group and 17.5 % in HC group (Figure 4).
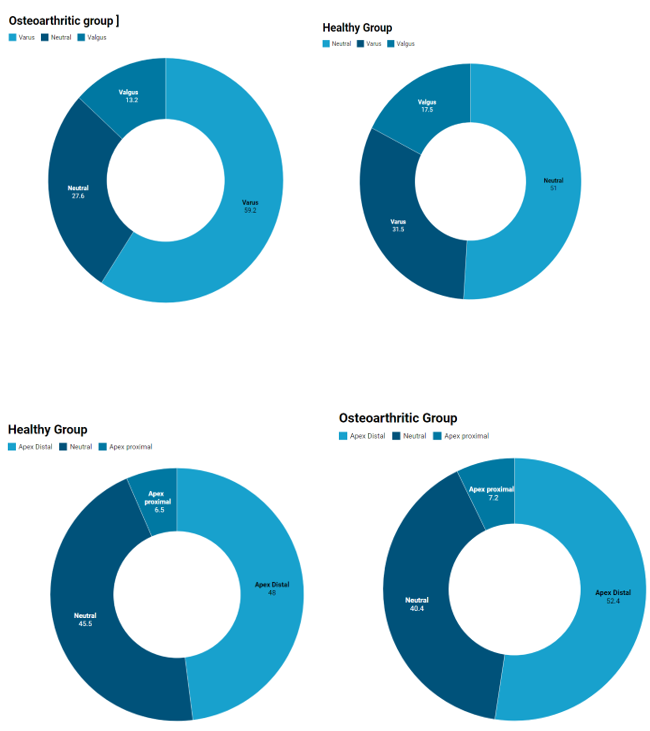
JLO Type
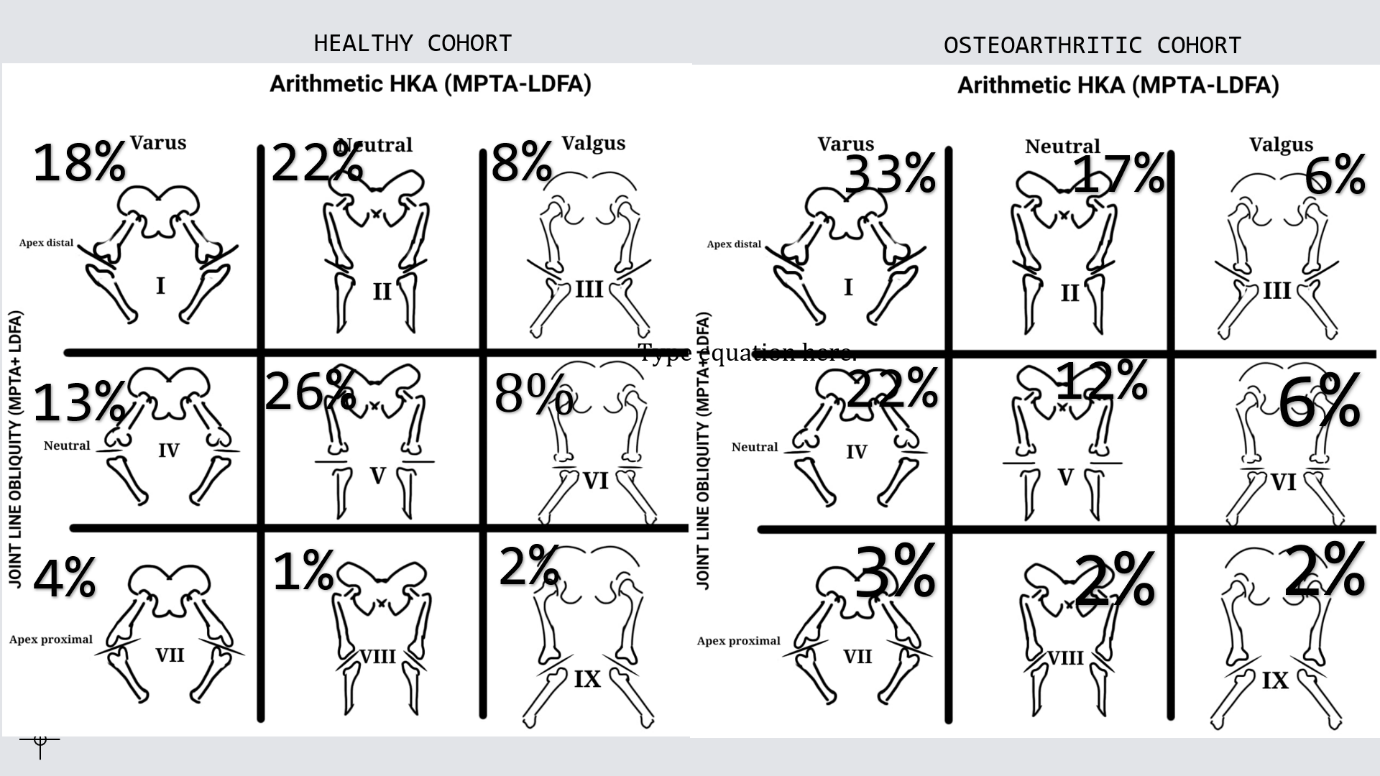
JLO types followed a similar trend in both the groups. Apex distal type accounted for commonest JLO in both the groups i.e., 52.4% in OC group and 48% in HC group. Neutral alignment formed 40% in OC knees and 45.5 % in HC. Apex proximal type remained least common type overall (Figure 4). CPAK Type Type 1 formed 33.6 %, being the most common CPAK type in osteoarthritic knees. The other common types were type 4 (22.4%) > type 2(13.6%) > type 5 (11.6%). For the healthy knee cohort, the commonest CPAK phenotype was type 5 (25.5%) > type 2 (22%) > type 1 (17.5%) > type 4 (12.5%). These 4 types i.e., types 1,5,4,2 accounted for maximum share of knees in both cohorts.
Type 9, type 8 and type 7 were the types least seen in Indian knees (Figure 5 & 6).
Discussion
In our study we found that the CPAK types 1,2,4,5 are top four commonest types in both the study groups alike, albeit with a different sequence of occurrence. Types 8,9,7 similarly were rare overall, and this rarity is reflected equally in both the groups as they have similar appearances in OC and HC. These findings are like that of Macdessi, et al. [6] who confirmed the applicability of CPAK classification to their population. Hence CPAK system can be used reliably to predict the native knee anatomy even in Indian arthritic knees owing to the concept of aHKA. This also supports the reliability of aHKA for Indian knees.
Among the top four, varus types (type1,4) were found to be more common in arthritic group (OC type1=34%, OC type 4=22%) while they ranked behind neutral types (type 2,5) in healthy group (HC type1= 18%, HC type 4=13%). Similarly, the neutral types (type 2,5) were comparatively less frequent in arthritic group as against their frequency in HC. Inferring from the data, whether CPAK type 1 and CPAK type 4 are more prone to developing Osteoarthritis of knee joint was examined. The odds of developing osteoarthritis in type 1 CPAK were 2.84 while that for type 4 were 2.02. Cerejo, et al. [8] also in his study mentioned the impact of varus alignment on osteoarthritis progression such that varus alignment at baseline increases the odds of 18-month progression in medial compartment arthritis by 4-fold. Whether having a native knee anatomy like that of CPAK types 1 and 4 predisposed to knee osteoarthritis needs to be further researched thoroughly. A deeper insight of knee dynamics in these high-risk knee groups can be used to improve KA techniques and in prevention strategies if possible. An important factor to consider with the above finding may be the older average age in arthritic study group (mean 59) as compared to healthy group age (mean 37) as OA and varus malalignment is more frequently seen with older population. However as inferred previously C.P.A.K. using aHKA predicts the native alignment of knee under study rather than the progressive change in alignment that is seen with arthritis.
Bellman et al in his study introduced the concept of constitutional varus wherein a considerate amount of populace has a state of natural varus alignment which exists at skeletal maturity [2]. Restoration to neutral alignment during knee replacement for these individuals as it disturbs their natural knee dynamics. Bellman et al calculated the proportion to be 32% in males and 17 % in females [2]. In our study based on Indian knees the CPAK types [1, 4, 7] that represent constitutional varus accounted for 59% of arthritic knees and 48% (216/450) of both our study groups combined (OC = 250, HC=200). A very high percentage of Indian knees are found to have constitutional varus when compared with Caucasian data that exists. Firstly, the high prevalence of constitutional varus in Indian knees may account for high prevalence of knee osteoarthritis and it being more common for Indians as compared to Caucasians who more commonly face osteoarthritis of hip. Secondly the aim for MA during total knee replacement (TKR) i.e., CPAK type 5 accounted for only 12 % of OC group and 18% of both groups combined. This points out the fact that restoration to a neutral alignment is not applicable to a major portion of population undergoing TKR and it does not represent the anatomy of most Indian knees. Fitting the desired result of neutral alignment to knees that are used to varus dynamics may be reason for increased implant wear and postoperative pain.
Macdessi, et al. [6] concluded that across all CPAK types, majority of KA treated knees achieved optimal balance compared to MA TKAs. This effect of KA TKAs was maximum for type 1> type 2 > type 4 meaning that these CPAK types benefit the most from KA approach. As these are also the most frequent Indian knee types, the choice of KA needs to be explored further as it caters to majority of Indian knees.
The aHKA being a marker of native knee alignment gives an insight into association of alignment and osteoarthritis. The RANGE for aHKA for OC was -36 to 32 (68) while that for HC knees was -13 to 22(35) meaning that the readings for osteoarthritic knees were more widely scattered than healthy knees around their respective averages. This also meant that the more severe the varus or valgus alignment of the knee, more likely for it would develop osteoarthritis.
The sample size of 200 healthy and 250 osteoarthritic knees in the Indian population is statistically adequate to assess the CPAK classification. The study used the system created by MacDessi, et al. [6] and tested its validity for the Indian population [6].
Our study has several limitations. Firstly, native knee anatomy with severely arthritic knees with altered bony landmarks cannot be assessed under CPAK system. CPAK deals only with the coronal alignment of knee joint whereas knee functions as a three-dimensional joint.
KA approach TKR and C.P.A.K. classification fails to address patellofemoral kinematics. Majority of KA TKR’s are done using implants that are designed for mechanical alignment thus not addressing the altered trochlear anatomy. Hence rates of patellofemoral complications remain similar in MA and KA TKR [9]. The age range of studied osteoarthritic group was comparatively older than that of healthy group. The study fails to demonstrate temporal relation between certain CPAK types and risk of OA.
Conclusion
C.P.A.K. classification can reliably be used for studying knee alignment in Indian population. Constitutional varus being commoner in Indian knees (48%) than their western counterparts implies that majority of Indian knees are in varus dynamics, hence a Kinematic approach caters to majority of the population.
The commonest C.P.A.K. knee types in Indians are TYPES 1, 2, 4 ,5 with varus types 1(34%) and 4(22%) being commonest in arthritic group and neutral types 1, 2 being commoner in non-arthritic knee group. Further research is needed to understand which Indian C.P.A.K. types benefit the most from KA TKR [10].
References
-
Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD (2010) Patient satisfaction after total knee arthroplasty: who is satisfied and who is not. Clin Orthop Relat Res 468(1): 57-63.
-
Bellemans J, Colyn W, Vandenneucker H, Victor J (2022) The Chitranjan Ranawat Award: Is Neutral Mechanical Alignment Normal for All Patients. The Concept of Constitutional Varus 470(1): 45-53.
-
Oussedik S, Abdel MP, Victor J, Pagnano MW, Haddad FS (2020) Alignment in total knee arthroplasty. Bone Joint J 102-B(3): 276-279.
-
Maderbacher G, Keshmiri A, Krieg B, Greimel F, Grifka J, et al. (2022) Kinematic component alignment in total knee arthroplasty leads to better restoration of natural tibiofemoral kinematics compared to mechanic alignment Knee Surg Sports Traumatol Arthrosc 27(5): 1427-1433.
-
MacDessi SJ, Griffiths-Jones W, Chen DB, Jones SG, Wood JA, et al. (2020) Restoring the constitutional alignment with a restrictive kinematic protocol improves quantitative soft-tissue balance in total knee arthroplasty: a randomized controlled trial. Bone Joint J 102-B(1): 117-124.
-
MacDessi S, Griffiths-Jones W, Harris I, Bellemans J, Chen D (2022) Coronal Plane Alignment of the Knee (CPAK) classification Bone Joint J 103-B(2): 329-337.
-
MacDessi SJ, Griffiths-Jones W, Harris IA, Bellemans J, Chen DB (2020) The arithmetic HKA (aHKA) predicts the constitutional alignment of the arthritic knee compared to the normal contralateral knee. Bone & Joint Open 1(7): 339-345.
-
Cerejo R, Dunlop DD, Cahue S, Channin D, Song J, Sharma L (2002) The influence of alignment on risk of knee osteoarthritis progression according to baseline stage of disease. Arthritis Rheum 46(10): 2632-2636.
-
Rivière C, Dhaif F, Shah H, Ali A, Auvinet E, Aframian A, et al. (2018) Kinematic alignment of current TKA implants does not restore the native trochlear anatomy. Orthopaedics & Traumatology: Surgery & Research 104(7): 983-995.
-
Paley D, Pfeil J (2022) Principles of deformity correction around the knee 29(1): 18-38.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results