Effectiveness of Local Surgical Site Infiltration and Regional Nerve Blocks for Elective Foot Surgery Adnan a Faraj, Lesley Scanlone
Introduction: Peripheral nerve block for pain relief in elective foot surgery is recommended by the national institute for clinical excellence. The aim of the current study was to evaluate this. Material and Methods: In a retrospective study on the quality of pain relief in 100 patients undergoing elective foot and ankle surgery using, the degree of pain relief, and the duration of anaesthesia was analysed. Three methods of local infiltration was used, US guided, guided by anatomical landmark and local infiltration at site of surgery. The data was collected using a questionnaire, assessed and discussed with the anaesthetic and the orthopaedic team. The surgery was for elective foot conditions with the patient under general anaesthesia. Results: Local surgical site infiltration was used in in 40 cases, Ultrasound guided (USG) local anaesthetic injection was given for 30 of cases, and infiltration using anatomical land mark was given in for 30 cases. The duration of anaesthesia was longer when USG block was used after general anaesthesia. The degree of pain relief was similar between blocks and local surgical site infiltration. Conclusion: Local surgical site infiltration at the end of the operation is effective in pain relief following foot surgery and is less time and cost consuming.
Introduction
Regional nerve blocks can be offered routinely for people needing pain relief, during or after surgery, provided that doctors are sure that the patient understands what is involved and agrees to the treatment the procedure is carried out by experienced practitioner and the patient is involved in the decision and the procedure is monitored (NICE).
NICE looked at a total of 11 Comparative and non- comparative studies on the efficiency of nerve blocks blocks, has been confirming the value of their procedure for pain relief and in unfit patients as an alternative to general anaesthesia [1, 2, 3, 4, 5, 6]. Variable success rates and complications have been recorded (NICE) [7]. Local surgical site infiltration is well established in general and orthopaedic surgery, it also has been used in foot and ankle surgery. This has been an established technique [1].
The options mentioned in literature for pain relief used following foot and ankle surgery has been analgesia, local surgical site infiltration, and nerve blocks at the level of the ankle, popliteal, and the sciatic nerve or femoral nerve. Traditionally, local surgical site anaesthetic injection has been commonly used [1, 2, 3, 4, 5, 6].
- Evaluate the practice of local anaesthetic block in Bridlington hospital for patients undergoing elective foot and ankle surgery
- Compare efficacy and effectiveness of local anaesthetic surgical site injection with pre-operative foot and ankle block using ultrasound or landmark guidance.
- Use the information to guide future practice changes
Material and Methods
This retrospective study was conducted in the orthopaedic department, Bridlington Hospital- North Yorkshire between 2016-2017. All patients captured in the study, underwent elective forefoot surgery; hallux valgus correction (80%), forefoot fusion (15%) and replacement of the big toe metatarsophalangeal joint (5%). The research and development department registry this study as an audit.
Postoperative analgesia was composed of either of foot and ankle block using anatomical landmark or Ultrasound scan (US) guidance or local surgical local anaesthetic infiltration. The choice of the types of foot block or local surgical site infiltration was at the discretion of the surgeon and the anaesthetist in the lights of patient’s choice and informed consent. The three options were discussed with the patient on the day of surgery during surgical and aesthetic assessment and clerking. The anaesthetist and the surgeon further discussed this in the team brief prior to starting the operative list.
The following data was captured; the American scoring for anaesthesiologists (ASA) of the patients, the record of anaesthetics type, and duration the medications in the pre and postoperative period, the added time for the anaesthetic time when blocks or infiltrations were used, the amount of local anaesthetics given, the type, premedication, peri and postoperative analgesia given and the type. Patients are made comfortable in the recovery room prior to sending them back to the ward.
Exclusion criteria: Patients with peripheral neuropathy and Rheumatoid disease, patients who have had spinal anaesthetics were excluded from the study.
Postoperative pain score and documentation was carried out by the recovery nurse, the surgeon and the ward nurses. The pain relief was assessed using Visual pain analogue (0- 10), mild pain is (0-3), moderate is (4-6), severe is (7-10).
Medical, anaesthetic notes was obtained to review the nursing section of notes, the entry on the CPD (computerised patient documentation) were reviewed. In this series, induction analgesia of Fentanyl/ Fentanyl and intraoperative analgesia. Premedication analgesia was used before surgery.
Results
The current retrospective study on 1ii patients was conducted to compare the three techniques, Anatomical land mark (ALM) (30 patients), US guided blocks (30 patients) and local anaesthetic infiltration (40 patients) for pain relief used following elective surgery of the foot. The aim was to study the effectiveness of each technique and the duration each technique has taken to be administered. The surgery was conducted in Bridlington hospital were enrolled. The mean age was 49 (32-70) years, female to male gender ratio was 59/41. All these patients were operated upon under general anaesthetics. The ASA scores were II for 71 patients and I in 29 patients).
The results were analysed by the 2nd author (senior recovery nurse) following discharge of the patient from the hospital. The patients were day cases.
- The mean amount for local infiltration was 20 mls of 0.5% Chirocain. The amount used for USG was 18mls in 46.5% and 20mls in the remainder. When ALM was used, a mean 20 mls of local anaesthetics was used in 75%. On average the amount of local infiltration given post operatively as 20mls. 6% of the patients who have had USG needed less pain killers in the postoperative period compared to 40% needing less pain killer in the surgical site infiltration group.
- The larger amount of local surgical site local anaesthetic infiltration, the better the pain relief was (average 35mls of chirocain). Twelve patient with mild or no pain, did not receive any premedication, in the surgical site infiltration group.
- The anaesthetic time for anatomical land mark infiltration was administered significantly is a shorter period than the US guided infiltration (Figure 1).
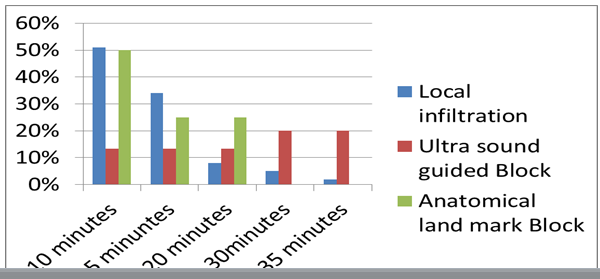
The Duration of Anaesthesia
The anaesthetic time was less than 15 minutes in 85% of surgical site infiltration and 35 minutes in 15%. The anaesthetic time and nerve block under USG was less than 15 minutes in only 26.6%, 16-35 minutes in 53.3% and in 19.9% it took between 16 and 45 minutes. The amount of long acting local anaesthetics injected varied depending on body weight and number of nerves blocked, the pain relief achieved was best with local infiltration and US guided injection, the anatomical land mark infiltration group has higher percentage of pain than the other two groups.
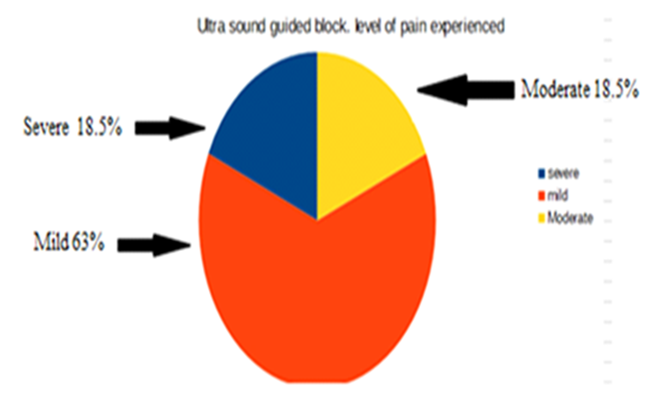
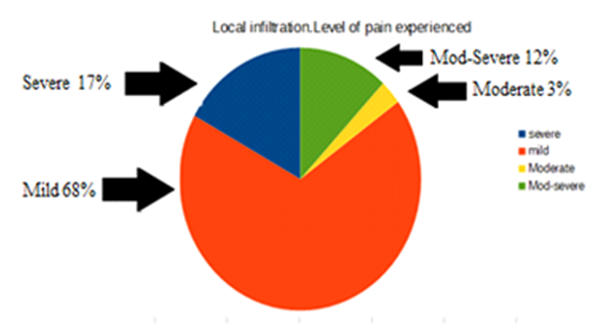
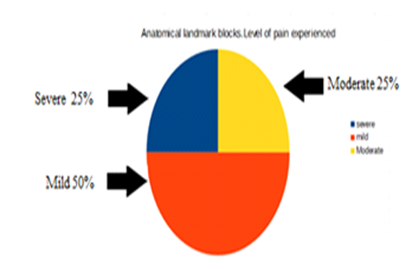
The pain visual analogue: 62.5% of the USG had 10/10 pain relief, while 68% of the local infiltration had similar amount of pain relief. The pain was severe in 18.7% (3/10) in USG group while 16% of the local infiltration group had severe pain. 50% of The ALM group had 10/10 pain relief. 66.6% of patients who had USG regional block with pre op analgesia reported severe pain post op, requiring opiate analgesia. This resulted in a longer recovery stay and 4 hours on the ward opposed to 2 hours for non-opiate treated pain relief. 33% reported mild pain (Figures 2-4).
Regardless of the type of local anesthetic injection; it was observed that when (Ibuprofen (400 mg) was added to (Paracetamol 1gm), the postoperative pain was better 80% of cases. The combination of Fentanyl (200mcg) with Paracoxib (40mg)/ morphine /Paracetamol in the perioperative period was superior to using Fentanyl alone in relieving. .the pain (90%)
Discussion
Reports of USG blocks claiming quicker techniques when ultrasound scan is used is scarce and success rate in some report is 50% (20/40 patients). The amount of local anaesthetics used however is less than when anatomical land mark is used for blocks without ultrasound guidance; the latter however have higher incidence of neurovascular injuries and is not recommended by NICE [8]. There was no neurovascular injury following nerve root block using any of the technique followed in this series. It is well established that nerve block using anatomical land mark without ultrasound guidance is associated with higher neurovascular injury. There are advocates that when nerve blocks are used, they should only be done under USG [2, 8].
The amount of anaesthetics used in our series was 2mls less when USG was used compared to local surgical site infiltration (LSSI). There was no complications recorded in relation to the volume of the local anaesthetic in both groups. Our results has shown that the anaesthetic time was significantly longer when USG blocks were used. In regards to the efficacy of pain relief; and in both parts of the study, patients in the local surgical site infiltration appeared to have less pain than USG and anatomical land mark injection blocks. In this series, the commonest method of local anaesthetic pain relief was infiltration of local anaesthesia.
The lack of consistency in producing pain relief in the USG blocks has been because of the failure of blocking all the sensory nerve supply of the skin. Often, the sural, saphenous, anterior tibial, posterior tibial nerves and branches have to be blocked. If any of these nerves is not blocked properly, the pain relief will not be complete. There is no consensus as to when and if alternative blocks can be used. In a comparative study, comparing foot and popliteal nerve block, both were found safe and effective; the popliteal block was less time consuming and analgesia more consistent [4].
In another prospective study comparing single nerve to double nerve block, it was suggested that double block (sciatic and femoral nerves) provides better surgical anaesthesia and good postoperative pain control for hindfoot and ankle surgery foot and ankle surgery than sciatic nerve alone [3].
The other factor which could undermine the outcome is the personnel giving the local blocks. There is no evidence that in the hands of the anaesthetists, the blockade is better than in the hands of the surgeons, in fact, the administration time of the nerve blocks is shorter in the hands of the anaesthetist (mean period of 6 minutes) [2]. Our results show significantly lower duration of the blockade when surgeons give local surgical site infiltration.
Despite reports of successful forefoot surgery under only ankle block and sedation without general anaesthesia [4, 5], only 2 of our patients had their surgery done without general anaesthesia in this series (2%). Forefoot surgery under ankle block alone may be safe and effective. Anaesthesia obtained permitted routine forefoot procedures and provided lasting post-operative analgesia. Combined with intra-operative sedation, the use of ankle tourniquet and same day discharge; has very high patient acceptance and satisfaction [5].
There are some unanswered questions for obtaining a good analgesia following foot and ankle surgery. The experience of the anaesthetists in administering USG blocks, and the number of cases to do to improve expertise and to avoid deskilling. It would be appropriate to standardise the practice and ratify the sub speciality colleague anaesthetists need to be involved in. Whilst the USG blocks for upper limb surgery is successful [7], the rate of this success is not evidenced in literature.
Local surgical site infiltration is effective, however compared too preoperative USG blocks, the intraoperative analgesia need was slightly higher when a successful USG block was administered. It is sensible to give the local surgical site infiltration prior to starting surgery.
The complications of nerve blocks is the masking of the potential compartment syndrome development following surgery remains a concern more so for fracture and dislocations of the foot, however it remain to be a concern. We have had no incidences of compartment syndrome.
Conclusion
Standardization of the practice of USG foot and ankle blocks and developing sub-speciality skill building is helpful prior to be able to perform surgery under only blocks. The pain relief has to be consistent. Local surgical site infiltration is effective is less time consuming and safe requiring no expenses or much training.
References
-
Herbst SA (2014) Local infiltration of liposome bupivacaine in foot and ankle surgery: case-based review’s. J Orthop (Belle Mead NJ) 43(S10): S13-S16.
-
Foote J, Freeman R, Morgan S, Jarvis A (2012) Surgeon administered regional blocks for day case forefoot surgery. Foot Ankle Surg 18(2): 141-143.
-
Lee KT, Park YU, Jegal H, Roh YT, Kim JS, et al. (2014) Femoral and sciatic nerve block for hindfoot and ankle surgery. J Orthop Sci 19(4): 546-551.
-
Migues A, Slullitel G, Vescovo A, Droblas F, Carrasco M, et al. (2005) Peripheral foot blockade versus popliteal fossa nerve block: a prospective randomized trial in 51 patients. J Foot Ankle Surg 44(5): 354-357.
-
Pilný J, Kubes J (2005) Forefoot surgery under regional anaesthesia. Acta Chir Orthop Traumatol Cech 72(2): 122-124.
-
Russell DF, Pillai A, Kumar CS (2014) Safety and efficacy of forefoot surgery under ankle block anaesthesia. Scott Med J 59(2): 103-107.
-
Ultrasound-guided regional nerve block (IPG285) (2009) Evidence-based recommendations on ultrasound- guided regional nerve block (placing a needle near a nerve to give pain relief/anaesthetic) Interventional procedures guidance Published.
-
Goebel S, Stehle J, Schwemmer U, Reppenhagen S, Rath B, et al. (2010) Interscalene brachial plexus block for open- shoulder surgery: a randomized, double-blind, placebo- controlled trial between single-shot anesthesia and patient-controlled catheter system. Arch Orthop Trauma Surg 130(4): 533-540.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results