Shifting Personal Protective Equipment Usage Found Amongst Nurses
Background: Personal protective equipment (PPE) has been around since the 14th century and the importance of it is unmeasurable. The COVID-19 pandemic left the world with a shortage of PPE mainly due to a resulting supply and demand problem. However, following peak COVID-19 pandemic PPE supplies began to normalize, yet hospital nurses’ focus on upholding proper PPE standards were markedly dwindling nationwide. Objective: The aim of this research study was to better understand the correlating factors playing a role in the noticeable change in hospital nurse attitudes regarding PPE usage. Methods: A mixed research design study was implemented over three weeks from January 2022 to February 2022 and included critical care registered nurses. A 27 open and closed-ended question survey was distributed via Survey Monkey to allow for qualitative and quantitative data collection. Data Analysis: A percent change was performed on quantitative data and a thematic analysis was conducted on qualitative data. Results: There was an 18.17% percent change increase in PPE supplies on the chosen critical care hospital units and consistent identifiable themes of fear, anxiety, and frustration in regards to PPE when working with COVID-19 patients. Conclusion: This survey did identify a reported shift in PPE usage amongst critical care nurses since peak COVID-19 pandemic. This shift could be due to many identifiable factors such as PPE accessibility, emotional resentments towards PPE supply, financial burden, PPE nursing education, and physical injuries from PPE wear.
Aims and Goals of Research Study
The aim of this research study is to better understand the correlating factors that are playing a role in the noticeable change in hospital nurse attitudes regarding PPE usage. The main goal for this study is to identify hospital nurse attitudes and behaviors towards PPE usage to ultimately evaluate underlying, correlating feelings, which would hopefully lead to an implementation intervention to help change this witnessed shift in mentality.
Research Question
Are there correlating factors in registered nurses working in a hospital setting to explain a shift in personal protective equipment (PPE) use seen before and during the COVID-19 pandemic?.
Problem Statement
The most immediate need of hospital nurses, during the initial phase of the COVID-19 pandemic, was a demand for personal protective equipment (PPE) due to an insufficient supply worldwide. The supply and demand for PPE led to an inconsistent distribution of PPE, which created contradictory PPE standards across hospitals nationally. In the months following the initial phase of the COVID-19 pandemic, the PPE supply greatly improved. However, nurses’ PPE usage has decreased creating a significant problem, which has also been identified in other countries, resulting in minimal protection from the virus [1]. Existing research in other countries has found potential factors to include COVID-19 vaccine distribution, the improved supply of PPE, burnout, employer frustration, and inconsistent PPE hospital guidelines [1]. The reality is all these factors could play a vital role in the attitude towards wearing less PPE. Therefore, this research study could help further existing research and act as a bridge in remaining knowledge gaps to elaborate on this phenomenon. A goal for the findings from this mixed research design study is to have them contribute to the field of research and be applicable to other areas of healthcare such as job satisfaction, burnout, retainability, and maintaining safe working environments. The purpose of this research study is to better understand what correlating factors are playing a role in this change in hospital nurse attitudes regarding PPE usage.
Theoretical Framework
Florence Nightingale is considered by many to be the founder of nursing and pioneer for numerous nursing practice guidelines. As a result, Florence Nightingale created nursing theories, which are still utilized to this day. One in particular is titled the Theory of Environment found in Florence Nightingale’s book written in 1860 titled, “Notes on Nursing: What it is, What it is Not” [2]. Florence Nightingale thought of this theory due to her experiences working as a nurse in the Crimean War where she noted how injured soldiers were dying quicker if being cared for in unsanitary environments [2]. Therefore, one of the key components to this theory is nurses assessing patient environments and changing what is needed to foster healing [2]. This central theory essentially laid the foundation for modern day infection control and protective personal equipment for both nurses and patients. During the COVID-19 pandemic, personal protective equipment (PPE) was in a worldwide shortage and nurses were left to figure out unconventional ways to protect themselves, their families, and their patients from a deadly virus. Post the peak of the COVID-19 pandemic, a shift in nursing mentality has been noted in decreased PPE usage meaning the environment for the nurse and patient is compromised and unhygienic. Nurses spend much of their day at the patients’ bedside and as a result they are important team members when it comes to enforcing proper hygienic methods to maintain infection control standards stemming from Florence Nightingale’s Theory of Environment.
Literature Review
A literature review was conducted to assess research pertaining to the history of personal protective equipment (PPE), mental health of nurses, physical PPE usage consequences, and importance of education in relation to PPE standards. The database CINAHL and Simmons University Library were used to foster the literature review search. The keywords “personal protective equipment”, “nurses”, “nurse”, and “nursing” were chosen for the literature review search. Articles were then narrowed down to include only academic journals from years 2017-2022. An initial number of articles obtained was 775. Further inclusion criteria for the articles were established and involved only full text, English language, and adult sample size. Articles with subject headings not pertaining to either: COVID-19; COVID-19 pandemic; personal protective equipment; occupational safety; nurses; nurses’ attitudes; occupational exposure; infection control; nursing practice; guideline adherence; and critical care nursing, were excluded from the literature review search. The final number of articles selected for the literature review was 45.
History of Protective Personal Equipment
In the 14th century, a horrible plaque brought havoc over Europe and scared the world of future outbreaks, which would later be known as the Black Death. Due to the uncertainty of how this plaque was being spread, people were desperate on finding ways to stop it and one way was to wear a mask with a long beak around those infected with the Black Death [3]. Here the first true form of personal protective equipment (PPE) was born. Since this development, research has progressed and discovered diseases can have various ways of transmission. This led to the evolvement of PPE to accommodate the vast differences in transmission since not every disease is spread via a respiratory pathway. Some diseases are spread through contact, airborne droplets, contamination, animals, or environmental factors. Florence Nightingale was a notable figure in the future of infection control due to the research she pioneered regarding the importance of hand hygiene and clean patient environments [2]. These concepts were developed in 1860 but are still famous today in the world of nursing and infection control, which arise from her book “Notes on Nursing: What it is, What it is Not” and built the foundation of her Theory of Environment. All these leading factors established the adoption of PPE guidelines stemming from infectious disease experts and worldwide organizations such as the CDC or WHO with a universal goal of standardizing PPE precautions. For example, standard PPE precautions encompass only gloves, contact PPE precautions entail the use of a gown and gloves; droplet PPE precautions pertain to gloves and a mask; and airborne PPE precautions utilize a N95 mask and gloves. COVID-19 perplexed many infectious disease experts on how it was spread resulting in continuous changes to PPE precautions when taking care of COVID-19 patients [3]. Regardless of the type of precaution, what remained the same standard for all, was each type of PPE was considered a one-time use, meaning once exited the patient’s room, the PPE was meant to be discarded. However, what happened next in the COVID-19 pandemic challenged these established PPE standards.
China was the epicenter of the pandemic and was also the main worldwide exporter of PPE. However, due to the pandemic originating in China, many countries were ceasing importation of PPE from China, which became the catalyst in the worldwide PPE shortage [4]. In the peak pandemic of COVID-19, all types of PPE were being utilized while the transmission of COVID-19 was being studied. Nurses were wearing N95 masks, face shield or goggles, gown, gloves, surgical caps, surgical shoe covers, and in some cases full body hazmat suits. As COVID-19 spread to other countries, they were finding themselves without adequate PPE due to the extreme demand for all types of PPE.
To further narrow this analysis to the United States, a study analyzed the main contributing players in the PPE shortage found within the United States [5]. These were found to be: an inappropriate hospital budgeting structure setup for PPE; worldwide supply and demand mismatch; and lack of government stepping in to incentivize United States factories to make PPE for local distribution. On top of this, the average cost to make PPE was increasing, which when coupled with an inappropriate PPE budget structure resulted in disaster. A study analyzed the average cost of PPE, specifically gowns, since during the peak COVID-19 pandemic the material to make gowns was becoming scarce to find [4]. Pre-pandemic gown cost was found to be an average of $1.10 US dollars/gown, which increased to an average of $9.63 US dollars/gown during the COVID-19 pandemic. All these factors combined created an imbalance of PPE in the United States, which led to many healthcare workers feeling unsupported and forgotten while they fended for themselves in the fight against COVID-19. However, in the months post peak COVID-19 pandemic, the PPE shortage was eventually resolved yet a phenomenon of nurses not adhering to COVID-19 PPE guidelines was beginning to be seen.
Physiological Consequences of Protective Personal Equipment Usage
Due to the previously mentioned factors playing a role with the worldwide and United States personal protective equipment (PPE) shortage, many healthcare members were left reusing their PPE, not taking off their PPE for their entire shift duration or were left to use inadequate forms of PPE. A study was conducted to gain a better understanding how much time nurses were wearing PPE while taking care of COVID-19 patients. From the study, it was discovered nurses were wearing PPE for an average of 6.38 hours/day [6]. Most nurses work twelves hour shifts meaning this data is suggesting over half of a nurse’s shift was spent while wearing PPE. Due to the uncertainty of how COVID-19 was transmitted, many nurses were wearing head to toe PPE with approximately 23-42 minutes spent putting on PPE and approximately 22-36 minutes spent taking off PPE. As a result of these findings, it was clear to researchers how long nurses were spending in PPE during their shifts. This led the researchers to further explore what physical consequences resulted from this prolonged time in PPE. The study findings, from a sample size of 165 nurses, exposed the following experiences found while wearing PPE: 81.88% reported poor vision; 79.38% reported nasal congestion; 74.38% reported decreased musculoskeletal mobility; 72.5% reported excessive sweating; 61.25% reported a level of skin damage; and 58.75% reported difficulty breathing. These findings were experienced while nurses were wearing PPE and show just how uncomfortable these PPE measures can be.
Coinciding with this study, another study analyzed the reported pressure injuries by nurses in relation to the immense amount of PPE worn during the peak COVID-19 pandemic [7]. This is an important factor to investigate given the previously mentioned average time nurses spent wearing PPE. This is because it is well-known that pressure injuries can result in as little as 2 hours, especially when pressure is placed on areas with little fat or bony prominences. A study encompassing a sample size of 266 nurses, found 77.1% conveyed they experienced a pressure injury from resulting PPE and 92.8% stated they experienced a level of pain from the PPE [7]. The most common sites of pressure injuries from PPE were located on the forehead, ears, and nose.
Another study, including a sample size of 297 nurses, analyzed an array of physical consequences from prolonged wear of PPE [8]. Researchers revealed 81.8% experienced pain located behind their ears in relation to prolonged mask wear [8]. This was the highest consequence reported from prolonged PPE wear. Other reports from prolonged PPE wear included the following: 78.5% experienced difficulty breathing; 60.3% reported excessive dry mouth; 59.1% stated they experienced a state of eczema; 58.9% described feelings of palpitations and dizziness; 57.8% reported excessive dry skin; 53.9% indicated a level of skin breakdown; and 42.1% experienced a sense of nausea [8]. What is key about this study compared to the others is these reports were noticed while nurses were wearing PPE and were still experienced even after the removal of the PPE [8]. Due to all these reported experiences from multiple studies, it is easy to infer a thought process to explain how and why a nurse may not want to wear an immense amount of PPE for prolonged periods of time. This inferable thought-process is a potential contributing factor justifying the phenomenon of nurses not adhering to COVID-19 PPE guidelines after resolution of the PPE shortage in the United States.
Methodology
Design
The research study design was a mixed methods integrating quantitative and qualitative data collection methods. Strengths of a qualitative research study are they provide cost efficient data collection; provide detailed information on a topic; and can lead to the generation of new theories [13]. Limitations of a qualitative research study are they are more difficult to analyze due to inability to fit perfectly into certain categories; data collections and statistical analysis can be time consuming; findings cannot be generalized to a certain population; and they cannot be used to determine cause and effect. Strengths of a quantitative research study are they are easily interpretable; data is thought to be more dependable; and research discoveries can be generalizable to other populations. Limitations of a quantitative research study are they are not vigorous enough or capable of describing complex phenomena. Therefore, the rationale for using a mixed methods technique was to produce generalizable robust data to explain the phenomenon behind the feelings and mentality of the research participants.
Institutional Review Board and Site Approval
The site of the research study was a hospital in Massachusetts. No Institutional Review Board (IRB) approval process was needed at the chosen hospital since no patients were involved in the study. Therefore, the site approval process did not warrant IRB verification. However, site approval was granted from the hospital’s Director of Nurses and Nurse Educator. Submission to the IRB at Simmons University was conducted via appropriate application forms and approved in December 2021.
Setting
Registered nurses who work in critical care units particularly: the intensive care unit (ICU), post anesthesia care unit (PACU), and emergency room (ER). The rationale for the inclusion of the specific hospital units was these critical care units were highly exposed to COVID-19 patients during the peak COVID-19 pandemic and were majorly affected by the PPE shortage compared to other hospital units.
Data Methods
The method of the research study was to gather quantitative and qualitative data via a distributed questionnaire form. Surveys and questionnaires do not have the same format for predicting validity and reliability since quantitative studies have more conclusive ways to ensure validity and reliability of a study compared to qualitative studies [13]. Therefore, combining methods of qualitative and quantitative provided the study with the best of both worlds in terms of validity and reliability. For this research study the questionnaire was distributed via the survey website Survey Monkey. This rationale is based off Survey Monkey being well-known as a highly credible website that helps researchers design questionnaires with methods that are tested and verified by a team of researchers ensuring the research study is yielding high quality results.
Data Collection
Cluster sampling was obtained to provide a sample size range of 10-40 participants. Research participants were recruited through a convenience sampling technique via email at their place of work. The 27 question survey was conducted over a timeframe of three weeks from January 2022 to February 2022 and contained a blend of close and open-ended questions to allow for both qualitative and quantitative data to be gathered (Appendix A). Independent variables to consider were the: critical care units; experience working with COVID-19 patients; level of education regarding proper PPE use; and national PPE crisis. The dependent measurable variables were the reported feeling/attitudes regarding use of PPE pre-and post-peak COVID-19 pandemic along with corresponding decisions regarding personal COVID-19 vaccine use.
Data Analysis
The survey had an 85% completion rate with an average time of 4 minutes 54 seconds where 20 people opened the survey and 17 completed it. The age range for the research participants was between 27 and 67 years old with a mean of 49.5. A majority of the research participants had 5 years or less of work experience as a registered nurse on their unit with a majority having prior work experience on medical/ surgical floors. Since only 17 participants completed the survey this meant there were not enough responses to conduct and display presence of statistical significance via an IBM SPSS software for the quantitative data [14]. However, a percent change was able to be performed for analyzing pre-and post-peak pandemic responses. While a thematic analysis was performed on the qualitative data to uncover the various themes that played a role in the participant’s experiences. One participant did not give consent for the study so their responses were filtered out from the survey in order to uphold the outlined ethical considerations.
Ethical Consideration
Data was collected anonymously with no collection of patient specific identifiers, therefore, no breach in confidentiality could be obtained and was conveyed to each research participant via a consent form. Consent to voluntarily partake in the research study was obtained before a research participant could begin the survey. Due to the anonymity of the survey, there were no potential risks to the research participant’s confidentiality or physical, psychological, legal, financial, or social wellbeing. The benefits to the research participants were the research study allowed the chance for them to share their experiences to be heard; allowed a sense of closure; and allowed the potential for an intervention to be developed which would help protect future nurses and patients.
Results
Out of the 27 questions, there were a few that analyzed potential factors pre and post peak COVID-19 pandemic to explain a shift in personal protective equipment (PPE) use. The potential factors were access/availability to PPE, additional PPE education, and associated emotions from the PPE supply. The results were broken down to categorize responses amongst the three critical care units: intensive care unit (ICU), emergency room (ER), and post anesthesia care unit (PACU).
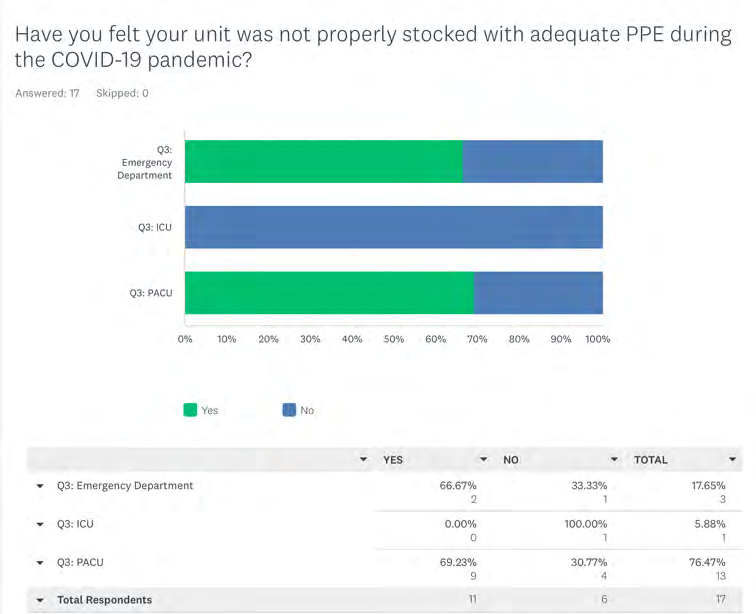
Analyzing accessibility/availability to PPE, a majority of research participants (64.71%) felt their unit was not properly stocked with PPE during the COVID-19 pandemic. Analyzing this further into separate departments showed 100% of participants in the ICU felt their unit was properly stocked with PPE. This is compared to the 33.33% (ER) and 30.77% (PACU) who reported adequate access to PPE, but 66.67% (ER) and 69.23% (PACU) reported inadequate access to PPE. When participants were asked if PPE supplies improved post peak COVID-19 pandemic a majority (76.47%) reported improvement. Amongst the different units, 66.67% (ER) and 84.62% (PACU) felt improvement in PPE supplies, but 33.33% (ER), 100% (ICU), and 15.38% (PACU) reported no change on their units. The overall results show there was a 18.17% percent change increase in PPE supplies on the chosen critical care hospital units (Figures 1 & 2).
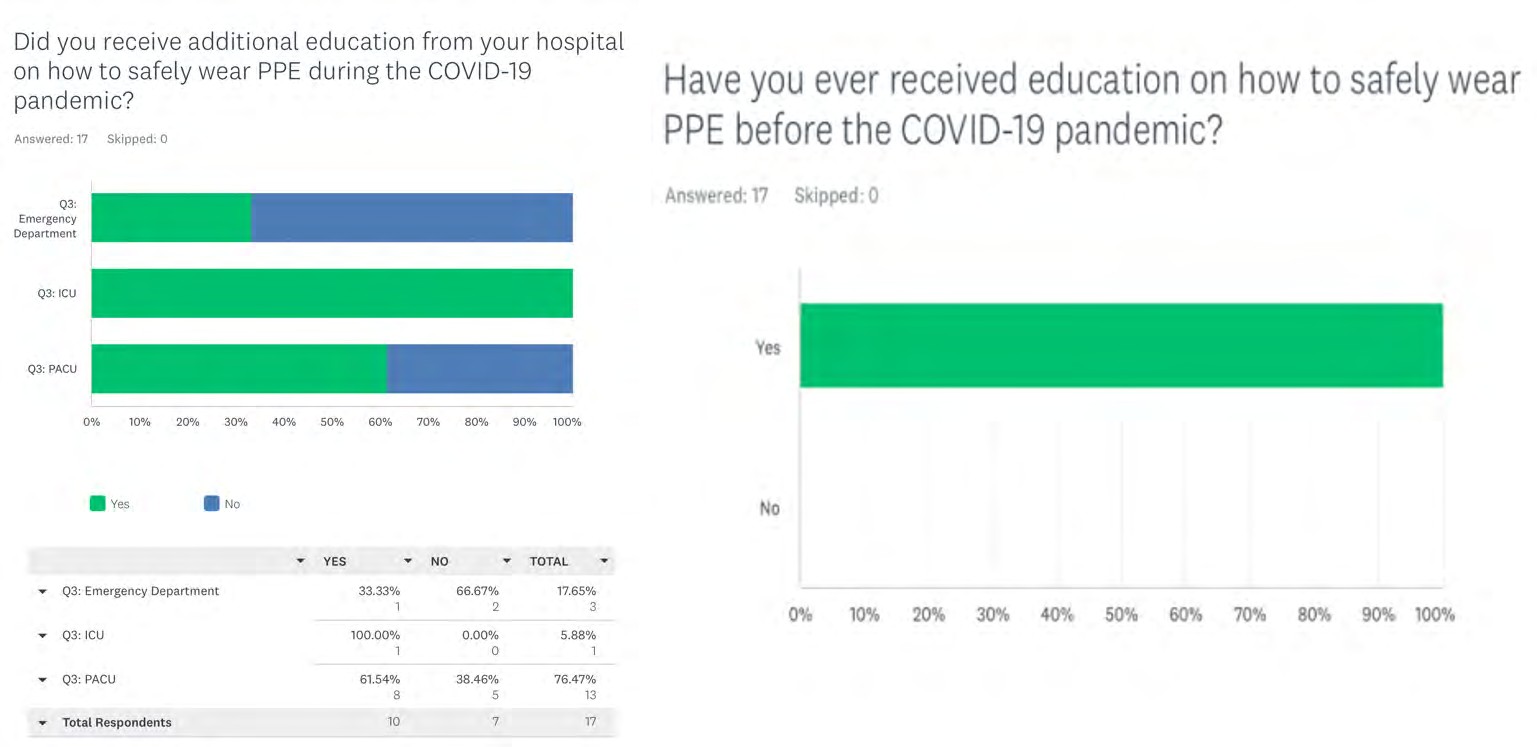
Evaluating PPE education showed 100% of research participants pertaining to all three critical care units received education regarding PPE before the COVID-19 pandemic. When asked if additional education was provided about PPE during the COVID-19 peak pandemic, only a slight majority (58.82%) reported there was while 41.88% reported there was no additional education provided. Breaking this down amongst the critical care units in question showed only 33.33% (ER), 61.54% (PACU), and 100% (ICU) had additional PPE education provided to them. This is compared to the 66.67% (ER) and 38.46% (PACU) who reported not receiving any additional PPE education. The overall results display a 41.18% decrease in receiving additional PPE education during the COVID-19 peak pandemic.
Emotional responses were collected to compare those felt at the beginning of the COVID-19 pandemic to those felt after the peak COVID-19 pandemic to analyze themes and changes. In the beginning of the COVID-19 pandemic, the most common themes experienced in each critical care unit was frustration and fear. A further breakdown analysis showed themes in the ER were frustration and satisfaction with supplies; themes in the ICU were fear; and themes in the PACU were anger, anxiety, frustration, disappointment, indifference, and neglect. Participants were asked if their emotions have changed since the beginning of the COVID-19 pandemic where a majority reported some change with the most responses occurred from the PACU with themes of improved frustration and decreased fear. The ICU had no reported change in emotions regarding the PPE supply and the ER had two responses with themes of increased frustration and disappointment. These overall results give rise to the question and support the notion of unit specific experiences.
Limitations
A major limitation of the study is time allocated to complete and submit this research project leading to inability to obtain an ideal amount of responses from participants. We allotted for a three week period to collect responses. Another limitation was the sample size was obtained from one particular hospital compared to multiple meaning results could be reflective of experiences pertaining to the individual hospital and may not be universally shared experiences. This can lead to results that may not be considered generalizable. Another limitation is the geographical location of the hospital used in the study since it may not reflect hospital worker experiences in areas with rural settings compared to a city. Upon result analysis, the number of responses obtained ranged from 15 to 17 depending on the question, which is a limitation due to the low response number coupled with inconsistent obtained responses. Another limitation is, the demographics revealed a majority of the questions were answered by registered nurses in the PACU, which could skew results due to the low variability of responses obtained from other critical care areas.
Discussion
Overall, this study demonstrated clear and consistent themes of fear, anxiety, and frustration throughout all three units in regards to the lack of personal protective equipment (PPE) while working with COVID-19 patients. Participants in the PACU and ICU reported some positive changes in their feelings due to seeing improvement in PPE supplies, however, ER nurses continued to report feelings of anger, anxiety, fear, and frustration towards the lack of PPE they received while at work despite the height of the pandemic slowing down. The theme of ER nurses continuing to have negative attitudes towards PPE has interesting, compelling correlations with level of education and PPE access. Upon analysis, ER nurses had the lowest reported rate of continuing education (33.33%) regarding how to properly utilize PPE compared to PACU (61.54%) and ICU nurses (100%). The difference in nursing education support across the three critical care units, specifically the ER, can be suggested to explain the reported negative emotional themes experienced by ER nurses. Along with this, nurses in the ER and PACU had the highest reports (over 66%) felt they had inadequate access to PPE in times of need, which again could explain the common emotional themes of fear, anxiety, and frustration.
Nurses from each critical care area were asked if they were instructed to re-use PPE in an effort to save on cost and supply of PPE. Over 66% of ER nurses and 100% of PACU and ICU nurses answered yes. This is a direct comparison to the nurses, over 66% of ER and over 69% of PACU, who stated they had to use their personal finances to provide themselves with adequate PPE at work. Critical care nurses were asked if their hospital unit followed CDC guidelines during the COVID-19 peak pandemic where 70.59% responded yes and 29.41% responded no. Following this question, nurses were asked to evaluate how safe they felt wearing their hospital- supplied PPE where 52.94% reported feeling safe opposed to
41.17% reported not feeling safe and 5.88% felt indifferent.
The comparison of the previously mentioned data points sparked an interest in future evaluation into how much personal financial resources nurses had to use to provide themselves with enough PPE to feel protected while working. The financial impact the COVID-19 pandemic had on healthcare workers who provided their own PPE has not been researched or reported on very thoroughly. However, our research strongly suggests there was a financial burden on the healthcare workers who provided direct patient care to COVID-19 patients. This is due to the previously mentioned responses of nurses who provided themselves with PPE in- order to help their hospital save on costs/supplies in addition to feeling their unit was not following CDC guidelines and those who reported not feeling safe while wearing the hospital-supplied PPE. Therefore, a general conclusion can be made regarding an experienced financial burden.
Upon further analysis of details regarding PPE usage, 35.29% of critical care nurses responded they suffered a physical injury from wearing PPE while taking care of COVID-19 patients. A breakdown of the reported physical injuries from PPE usage showed common complaints of: pressure ulcers on nose and ears, skin irritations, abrasions/ cuts, acne, and facial rashes. Nurses were then asked about the level of ease it was to work while wearing PPE where 41.18% felt it was somewhat easy, 23.53% felt it was either easy or difficult, 23.53% felt it was difficult, and 11.76% felt it was very easy. Following these questions, nurses were asked to evaluate their current PPE compliance when providing direct patient care to COVID-19 patients where it was reported: 69. 23% of PACU nurses used PPE 100% of the time; 30.77% of PACU nurses used PPE 75% of the time; 100% of ICU nurses used PPE 100% of the time; 33.33% of ER nurses used PPE 100% of the time; and 66.67% of ER nurses used PPE 75% of the time.
Again, the survey demonstrated another example of unit specific practices regarding PPE utilization. Further questions as to why 33.33% of ER nurses complied with utilizing PPE 100% of the time warrants further discussion and investigation. There could be multiple factors such as lack of supply, burnout, depression, and lack of readily available supply.
Overall, these results are a cause for concern due to the differences in PPE usage across the three critical care units. Based on the survey responses, addressing multiple areas revolving around PPE and the COVID-19 pandemic, there is enough evidence to support the notion of unit specific factors playing a role in PPE usage, supply, distribution and utilization.
Nurse Practice Implications
The results of this study demonstrated the emotional toll that having a lack of personal protective equipment (PPE) during the COVID-19 pandemic was universally felt throughout all critical care areas. The implications of consistently working under these conditions as a practicing nurse can lead to burnout, unemployment, anger, and resentment toward hospital administration and personal depression. The hospital leadership at the chosen hospital faced the same difficulties as many worldwide hospitals in regards to supply chain issues; however the impact of not having easily accessible PPE has had a clear, negative impact on all nurses throughout each critical care unit. This impact needs to be addressed in order for nurses to continue to provide quality care of patients in all healthcare settings. Supporting nurses directly impacts the quality of care patients will or will not receive in hospital settings.
Conclusion
The conclusion of this research study was set out to answer the question about identifying any correlating factors to explain a shift in personal protective equipment (PPE) use before and during the COVID-19 pandemic. This survey did identify a reported shift in PPE usage amongst critical care nurses since the start of the COVID-19 pandemic. This shift in PPE usage could be due to the many identifiable factors from the survey such as PPE accessibility, emotional resentments towards PPE supply, financial burden, PPE nursing education, and physical injuries from PPE wear. It is worth mentioning there was an overall 18.17% increase in PPE accessibility to critical care nurses since the beginning of the COVID-19 pandemic. However, despite this small increase in PPE accessibility, critical care nurses continued to require more accessibility along with more education regarding how to properly utilize PPE.
Overall, this study provided a closer understanding of the many struggles critical care nurses have continued to face during the pandemic as well as shed light on the notion of unit specific experiences driving current PPE usage trends. This is mainly based on the emotional themes, lack of education, and mixed feelings toward PPE supplies reported by ER nurses, which means this could prompt a general study isolated to ER healthcare workers about how to better support them while working with COVID-19 patients. However, a more specific study or quality improvement project revolving around the Emergency Department at this particular hospital is warranted to look into what can be done to correct their workplace environment due to the reports of feeling under supported, undersupplied, and undervalued by the ER nurses.
References
-
Hossain MA, Rashid MUB, Khan AS, Sayeed S, Kader A, et al. (2021) Healthcare worker’s knowledge, attitude and practice regarding personal protective equipment for prevention of covid-19. Journal of Multidisciplinary Healthcare 14: 229-238.
-
Petiprin A (2020) Nursing theory: Nightingale’s environment theory. Nursing theory.
-
Cherry DJ (2020) The role of face protection for respiratory viral infections: A historical perspective. Journal of the Pediatric Infectious Diseases Society 9(4): 411-412.
-
Harvey J (2020) Perspectives covid-19 and ppe in context: An interview with china. Journal of Public Health 42(3): 480-482.
-
Cohen J, Van Der Meulen Rodgers Y (2020) Contributing factors to personal protective equipment shortages during the covid-19 pandemic. Preventative Medicine 141: 1-7.
-
Wu M, Zhang L, Ning N, Liu L, Liu X (2021) Survey and enlightenment on the wearing of p r o t e c t i v e equipment of nurses working on the front line against COVID-19. Medicine 100(19): e25924.
-
Bambi S, Giusti DG, Galazzi A, Mattiussi E, Comisso I, et al. (2021) Pressure injuries due to personal protective equipment in Covid-19 critical care units. American Journal of Critical Care 30(4): 287-293.
-
Xia W, Fu L, Liao H, Yang C, Guo H, et al. (2020) The physical and psychological effects of personal protective equipment on health care workers in wuhan, china: A cross- sectional survey study. Journal of Emergency Nursing 46(6): 791-801.
-
Moradi Y, Baghaei R, Hosseingholipour K, Mollazadeh F (2021) Protective reactions of ICU nurses providing care for patients with COVID-19: A qualitative study. BMC Nursing 20(45): 2-6.
-
Ezzat A, Li Y, Holt J, Komorowski M (2021) The global mental health burden of COVID-19 on critical care staff. British Journal of Nursing 30(11): 634-642.
-
Shawahna R (2021) Knowledge, attitude, and use of protective measures against COVID-19 among nurses: a questionnaire-based multicenter cross-sectional study. BMC Nursing 20(163).
-
Chen F, Zang Y, Liu Y, Wang X, Lin X (2021) Dispatched nurses’ experience of wearing full gear personal protective equipment to care for Covid-19 patients in china-a descriptive qualitative study. Journal of Clinical Nursing 30(14): 2001-2014.
-
Polit DF, Beck CT (2017) Nursing research: Generating and assessing evidence for nursing practice. In: 10th (Edn.), Wolters Kluwer pp: 784.
-
IBM (2021) IBM SPSS statistics: Data sheet.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda