Recent Advances in Approved, Withdrawn, Experimental and Investigational Drugs in Clinical Trials for Alzheimer’s disease
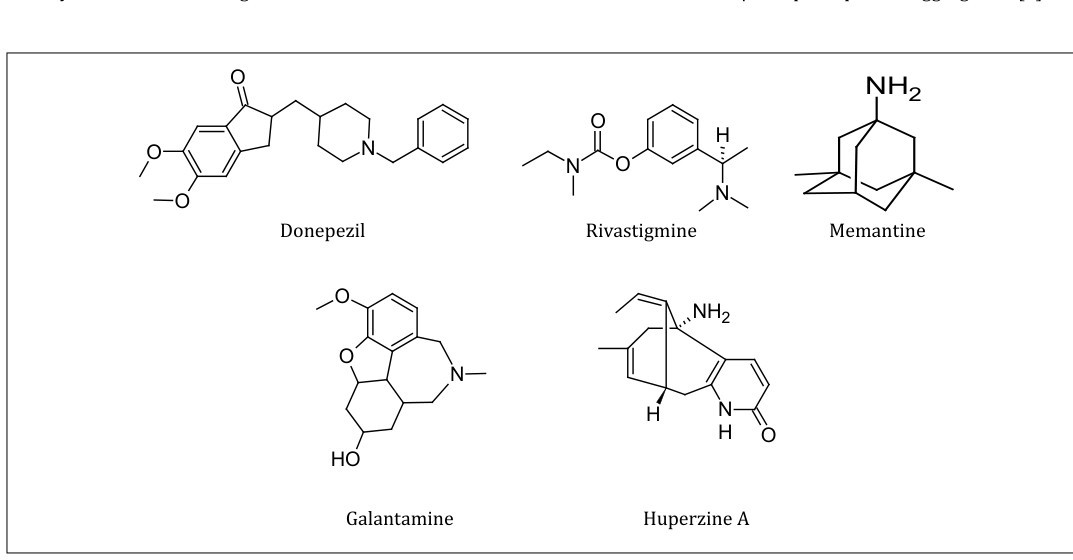
Alzheimer’s disease (AD) is an irreversible, chronic degenerative disease that slowly destroys memory and thinking skills, and eventually destroys the ability to carry out the simplest of day-to-day routine tasks. This disease is characterised by loss of neurons and synapses in the cerebral cortex and certain subcortical regions. Presence of beta-amyloid (Aβ) plaques and neurofibrillary tangles (NFTs) in brains of the affected patients are the distinguishable characteristics of this disease. Currently, no treatment is available to stop or reverse progression of AD, though it may temporarily improve symptoms. There are four USFDA approved drugs which are helpful for symptomatic treatment in AD namely Donepezil, Rivastigmine, Galantamine and Memantine. Memantine functions as an NMDA receptor antagonist, whereas the other three drugs act by inhibiting the acetylcholinesterase enzyme (AChE) resulting in an increase in the levels of acetylcholine (ACh) in the body. In the past decades, many advancements in the current drugs as well as the experimental drugs for AD have been made and these involve structural modifications and mechanistic improvements to increase the capacity of the molecules to cross the blood brain barrier (BBB). Synthesis of 2-acetylphenol-donepezil hybrids is an example of an approach which was adopted based on Multi- Target Directed Ligand (MTDL) strategy. Recently, synthesis of salicylanilide N-alkyl carbamates was carried out and these were observed to possess higher AChE inhibiting capacity than Rivastigmine. Memogain is an inactive prodrug of galantamine which has shown improved effectiveness, fewer side effects and due to its lipophilic nature is said to penetrate the BBB where it gets cleaved into active galantamine. Huperzine A is another highly selective AChE inhibitor and is approved for use only in China though not by USFDA. Tacrine and Huperazine A were combined together to form a hybrid molecule Huprine X, which is said to possess not only potency but also higher selectivity for AChE inhibition alongside anti-Aβ properties.
Introduction
Alzheimer’s disease (AD) is a chronic neurodegenerative disorder and is the most common cause of dementia. This disease generally starts at a slow rate but the symptoms worsen with the passage of time [1]. It is known to be affecting one - third of the world’s population aged more than 85 years [2]. Various hypothesis have been proposed to be causative of AD, primarily the deposition of intracellular neurofibrillary tangles (NFTs) and extracellular deposition of β-Amyloid (Aβ) plaques. This results in neurotoxicity and synaptic loss [3]. In the decade 2002-2012, 244 drugs were investigated for AD, of which only one drug Memantine was approved [4]. Presently there are only four USFDA approved drugs which are used for the treatment of AD namely Donepezil, Rivastigmine, Memantine, and Galantamine; alongside combinations of these drugs are also available. However, these drugs are single target acting drugs which improve the conditions of the patient by minimizing the symptomatic effects of the disease. Thus, currently there is no complete cure for AD. Tacrine was the first drug to be approved by the FDA for the treatment of AD in 1993 however was withdrawn in 2013 due to toxicity [5, 6]. Lately, it has been observed that increased exposure of anti-cholinergic agents is linked with a higher risk of dementia [4]. Current research is based on the Multi Target Drug Ligands (MTDLs) in the treatment of AD. They generally function by acting collectively on multiple mechanisms which are known to be the common causes of AD. Presently, there are nine major identified targets for the studies on application of MTDLs namely -Acetylcholinesterase (AChE), Beta-site amyloid precursor protein cleaving enzyme (BACE-I), Monoamine oxidases (MAOs), Metal ions in the brain, Glycogen synthase kinase - 3β (GSK-3β), N-methyl-D-Aspartate(NMDA), H3 Receptors, 5HT-receptors and Phosphodiesterases (PDEs) [6], in addition to targets like Aβ, Butyrylcholinesterase (BuChE) amongst others [6]. Currently, the MTDL strategy is being employed in development of novel medicines in treatment of AD. Hence, collective study on drugs and combinations of drugs is extremely important for the purpose of bringing out advancements in drug discovery and research in the treatment of AD.
In this work, we review the recent advances in drugs that are approved, withdrawn, or are experimental or investigational under clinical trials (CTs) for AD to provide insights into their structural features and chemistry and to provide an overview of the drug discovery scenario for therapeutics for AD. This might have relevance in accelerating drug discovery for AD therapeutics.
Approved Drugs
Donepezil, Galantamine and Rivastigmine are said to be competitive or reversible Acetylcholinesterase Inhibitors (AChEIs), whereas, Memantine is an irreversible NMDA receptor antagonist. (ID1) Donepezil a piperidine derivative (ID16) is currently the most extensively used drug for the treatment of AD. It was approved in 1997. It is a highly selective AChE inhibitor and has high potency [3]. Donepezil is well tolerated inspite of causing distinctive side effects like nausea, diarrhea, constipation and sleep disturbances [7]. SAR studies on Donepezil and derivatives have indicated that the carbonyl group on indanone ring is responsible for hydrogen bonding and increasing enzyme inhibition. Replacing it with a benzisoxazole ring was observed to improve the inhibitory activity [3]. The presence of electron withdrawing groups increases potency of the molecule. Also the presence of the basic nitrogen on the piperidine ring is important for increasing the activity and affinity of the molecule.
Advancements in Structure Activity Relationship Synthesis and investigation of 2-acetylphenol-donepezil hybrids (Table) is an approach adopted based on MTDL strategy for the improvement in efficiency of Donepezil. The biological responses of these molecules were analysed and evaluated for MAO and AChE inhibition [8]. Two molecules TM2 and TM14 were found to produce a significant increase in the capacity of the molecule to cross the blood brain barrier (BBB).
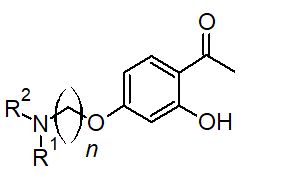
2-acetylphenol-donepezil hybrids
| Compound | n | NR R 1 2 |
|---|---|---|
| TM2 | 2 | N HN |
| TM14 | 2 | HN |
Advancements in Structure Activity Relationship Lately, a group of salicylanilide N-alkylcarbamates (Figure 2) were studied and it was observed that they showed more inhibitory effect on AChE than Rivastigmine. The affinity and activity of this molecule depended on the lipophilicity of the molecule which in turn was affected by the length of the alkyl carbon chain.3 Substitutions on the benzyl ring as well as on the nitrogen of the amide group was found to be necessary for the increase in AChE inhibiting activity.
Galantamine is an alkaloid isolated from the bulbs and flowers of Galanthus caucasicus. It is an AChE inhibitor and has also been studied for combination treatments with other drugs in the AD therapy [10]. Newer routes of administration for galantamine are being researched and studied apart from the usual oral route for better absorption and bioavailability. Two such examples are liposome embedded polymeric scaffolds for the extended delivery of galantamine [11]. And pressure sensitive adhesive patches for the transdermal delivery of Galantamine [12]. Gln-1062 (Memogain) (Figure 2) is an inactive prodrug of Galantamine which has shown better effectiveness and fewer side effects unlike the other cholinesterase inhibitors in the treatment of dementia. It has higher lipophilic nature due to which it is said to enter the brain where it is cleaved into active Galantamine.
Memantine is the only uncompetitive voltage dependent NMDA-Receptor Antagonist [13] till date proven to be useful in the treatment of AD. It is majorly used for the treatment of symptomatic effects in patients suffering from moderate to severe AD [14]. Memantine is known to decrease Aβ toxicity, decrease microglia associated inflammation, preventing hyperphosphorylation of tau, and increasing neurotrophic factors from astroglia [13]. Memantine targets glutametergic dysfunction and binds to the open state NMDA receptor channel [4]. Memoquin is a combination drug of polyamineamide caproctamine and muscarinic M2 receptor antagonist with synthetic derivative of coenzyme Q [3]. It acts as an ACE inhibitor and muscarinic M2 antagonist. It is known to decrease Aβ aggregation, β-secretase enzyme, tau-phosphorylation and free radical formation. This combination was known to show behavioural and cognition improvement in studies for the CTs for AD treatment. Currently this molecule is under study for its therapeutic properties and is considered to be an experimental drug [14]. Huperazine A is a highly selective AChE inhibitor [3]. It is a sesquiterpene alkaloid isolated from a clubmoss Huperzia serrata, approved for use only by China but not approved by USFDA on account of its toxicity [15, 16]. It is known to be useful for the treatment of fever, inflammation, blood related disorders and schizophrenia. Tacrine and Huperazine A were combined together to form a hybrid molecule referred to as Huprine X. These Huprine molecules were said to possess high potency and selectivity towards AChE for inhibitory action in ex vivo as well as in vivo studies. Huprine X possesses anti-amyloid properties and shows in vitro inhibition of Aβ and prion protein aggregation [3].
NH Cl
N
O
NH O
Cl NH2
R2
N
R1
O
O O H O
Huprine X Salicylanilide N-alkyl Carbamate derivatives Memogain
N NH O O
O
NH N
O
Memoquin Figure 2: Structural and mechanistic advancements in the approved drugs.
Withdrawn Drugs
In the past few decades, several molecules have been investigated for the treatment of AD and have undergone CTs. However almost all of these have been withdrawn, majorly due to lack of desired efficacy i.e not showing maximum therapeutic effects and/or showing severe adverse effects [14]. Henceforth we analyze the withdrawn drugs along with enlisting the potential causes of their withdrawal.
Drugs Withdrawn After Approval
Tacrine Tacrine was the first drug to be approved by the USFDA for the treatment of AD in 1993. It was a highly potent reversible AChEI and possessed anti-Aβ properties [3]. However, it was withdrawn from the market in 2013 since long term use of tacrine showed side effects including severe hepatotoxicity [17]. Since then, several analogues and combinations of tacrine were investigated for producing minimal side effects and maximal therapeutic activity. Tacrine based bi-functional inhibitors were first proven to be successful in 1996, wherein two tacrine molecules were connected via heptamethylene chain [18]. Combination of SAR of tacrine and dimerization strategy has led to production of highly selective and more potent tacrine homodimers [19].
NH2
N
Tacrine
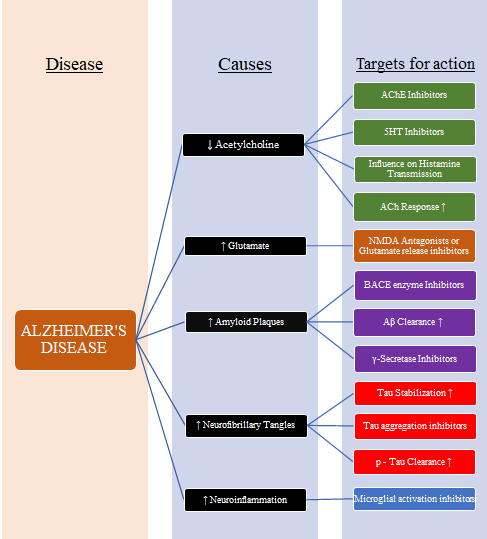
Classification of Treatment Strategies in Alzheimer’s disease with the Hallmarks and the Targets for Drug Action:
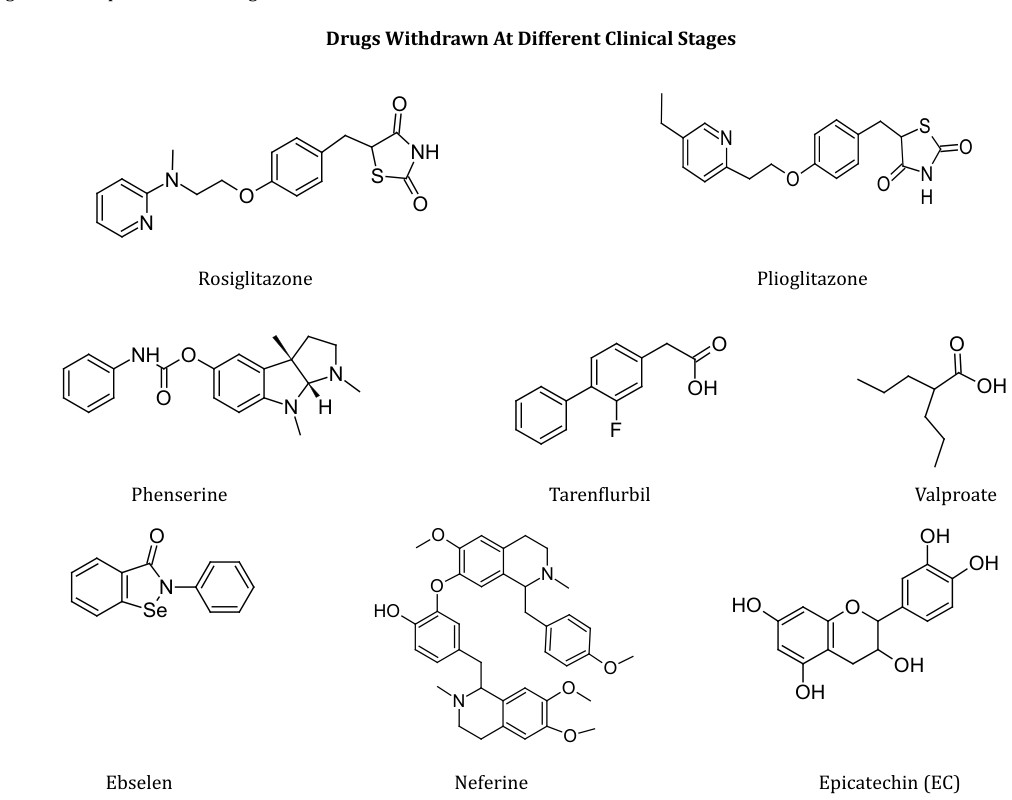
Drugs Withdrawn At Various Clinical Trial Stages
Rosiglitazone and Plioglitazone are thiazolidinediones and are known to be potent peroxisomal proliferator activated receptor gamma (PPAR-γ) agonists4 approved by USFDA
for the treatment of Type Diabetes Mellitus [20, 21]. They work by regulating glucose metabolism, lipid metabolism and suppressing inflammatory gene expression [22, 23]. Research has shown that the mechanism of progression of AD has been linked to both inflammation and decreased insulin sensitivity [24]. Both of these molecules were found to be inhibitors of BACE-I. Although Rosiglitazone was extensively studied for its activity in insulin pathway, the placebo trials which were conducted, failed to distinguish between Rosiglitazone and placebo when studied for primary endpoints. In CTs, Rosiglitazone showed no efficacy on cognition or global function. Plioglitazone was also studied but further trials were not conducted due to the conflicting results regarding its efficacy in AD treatment [24]. Both the drugs were withdrawn after phase 3 CTs [14].
Phenserine is a derivative of physostigmine and an AChE inhibitor [14]. It showed a moderate success in phase II CTs for the treatment of AD. Phenserine also reduced the concentrations of Aβ and Aβ Precursor Protein(APP) by reducing the translation of APP mRNA [25]. Although it showed a good tolerability and improvement in cognitive functioning during phase II CTs, it was withdrawn and further investigation regarding use in treatment of AD was stopped since the efficacy of the molecule was not seen [4].
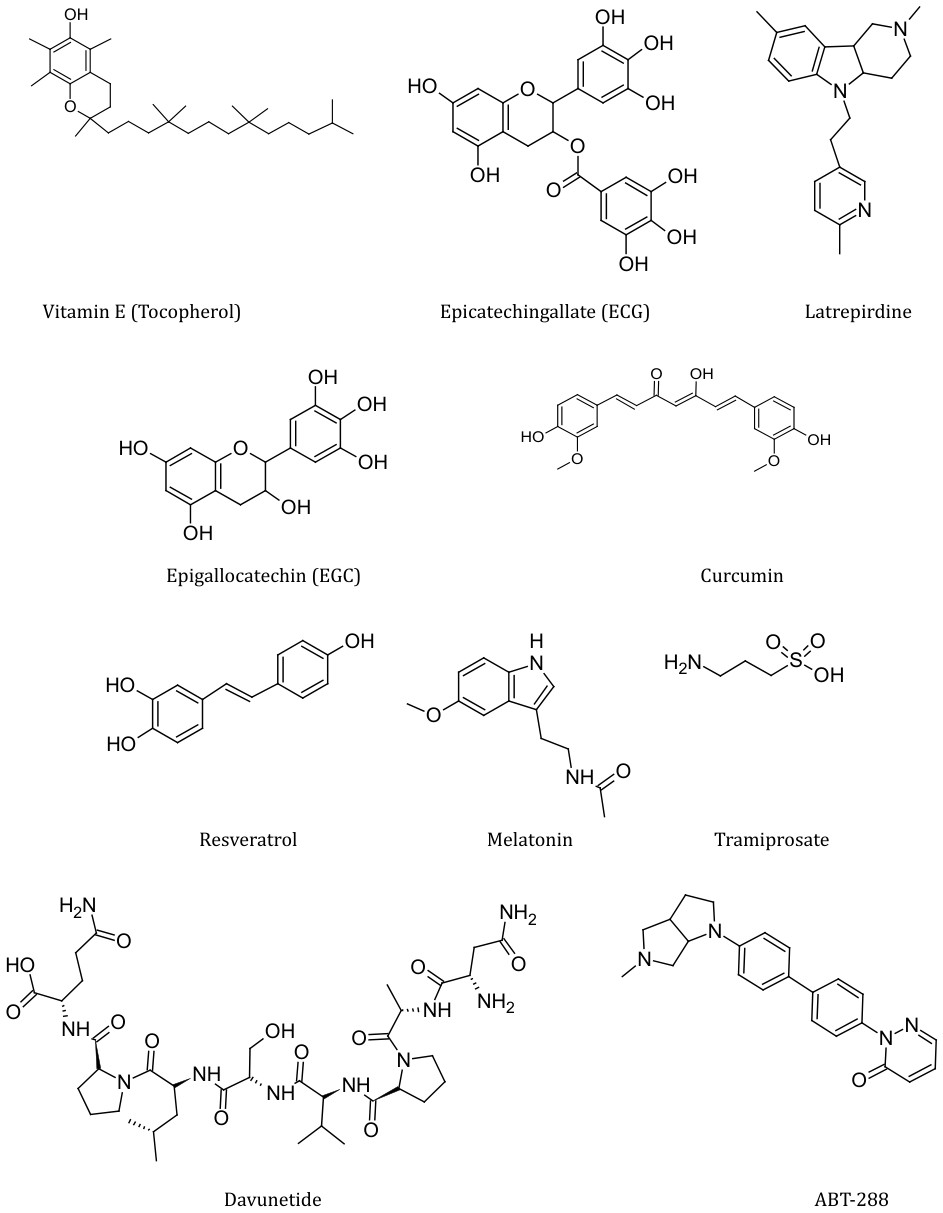
Latrepirdine, also known as Dimebon, and was first introduced in Russia and is a non-selective anti-histaminic drug. It has been studied under phase II CTs for its safety and tolerence levels. The results for these trials were positive and in favour of the drug usage. It weakly inhibits AChE and BuChE and is also known to inhibit the NMDA receptors with additional voltage-gated calcium channel blocking activity [26]. Latrepirdine also protected neuronal mitochondria from Aβ mediated toxicity [14].
Statins are a group of drugs known to be cholesterol biosynthesis inhibitors [27]. Cholesterol metabolism has been exclusively linked with AD pathogenesis. In recent trials, it was observed that statins can reduce phosphorylated Tau (pTau) in APP deficient neurons, which in turn suggests that its mechanism is independent of the APP gene. It was also studied that these cholesterol esters were not affecting major kinases such as GSK-3β which are responsible for tau phosphorylation. However further studies are required to understand the effect of modulation by CYP46A1 on other tissues and cells in the brain like oligodendrocytes, microglia and BBB [27].
Tarenflurbil is known to be a selective Aβ reducing agent that showed positive effect on cognition and functional results in mildly affected patients suffering from AD in the early stages of phase II CTs [28]. Further trials however showed that the drug molecule demonstrated no significant benefits on the primary outcomes for the treatment of AD in the intend-to-treat analytical study in phase II CTs [29]. Also no difference in secondary outcome measures was observed and it was withdrawn [28].
Valproic Acid (Valproate) is said to be a multitarget therapeutic agent which also works as a histone deacetylase blocker [30]. Several potential pathways of therapeutic action of valproate are being studied some of which are decrease in Aβ formation, inhibition of proinflammatory responses, enhancement of neurotrophic factors, etc. [30].
A trial conducted for Divalproex sodium (combination compound of valproic acid and sodium valproate) in nursing home residents with probable AD showed no benefit of the drug for the treatment of agitation related to dementia was seen [31]. Further trials for valproate were dicontinued after the phase III CTs [14]. Oxidative stress and free radical formation is one of the theories of aging which postulates that oxidative damage contributes a major part in neuronal degradation [32]. Oxidative stress is also an early condition seen occurring in AD [33, 34]. Increased oxidative stress results in an increase in Aβ aggregation and tau phosphorylation [35, 36]. Thus, antioxidants find substantial use for the symptomatic treatments of multifaceted diseases such as AD [37]. When amalgamated with with other therapeutics such as enzyme inhibitors, they exhibit enhanced therapeutic effects. These are known to be useful for AD, due to which an array of herbal medicines have been studied for their beneficial antioxidant and anti- inflammatory effects on AD [32, 37].
Flavonoids like Epicatechin(EC), Epigallocatechin(EGC), Epicatechingallate(ECG), etc have multifactorial antioxidant activities including scavenging effects on the superoxide anions and hydroxyl radicals. Considering several neuroprotective effects of red wine, it was suggested that several bioactive molecules like catechins, tannins, anthocyanidines, myricetin, etc. found in wine may have beneficial effects in AD [38].
Curcumin is a polyphenolic compound derived from Turmeric (Curcuma longa) and is known to be a herb native to the Indian subcontinent [39]. In Ayurveda, Curcumin has proven to be useful in the treatment of several disorders and conditions like liver disorders, respiratory problems, anorexia, etc [40]. The mechanism of action in treatment of AD involves targeting the two main markers involved in pathophysiology i.e Aβ and Tau proteins. It also shows activity by binding to copper, lowering the cholesterol levels, inhibition of AChE, enhancing insulin signalling pathway and behaving as an antioxidant [41]. Curcumin has the capacity to prevent the accumulation and formation of Aβ through the inhibition of GSK-3β dependent PS1 activation [42] as well as GSK-3β
inhibition. It inhibits hyperphosphorylation of tau through phosphatase and tensin homologue/protein kinase B/GSK- 3β pathway induced by Aβ [43]. Despite the considerable number of positive effects of curcumin which prove it to be a potential pathway in treatment of AD, it suffers from major disadvantage of low bioavailability due to which its ability to exert therapeutic effects is hindered [44]. Studies are currently focusing on optimizing the various ways through which the bioavailability of curcumin can be enhanced [41].
Resveratrol is a polyphenolic compound found in red wine, red grapes and other plant food items [45, 46] studies reveal that Resveratrol showed low bioavailability at therapeutic doses which was proven to be insufficient for treatment of AD [47]. Several molecules based in the stilbene scaffold present in Resveratrol have been synthesized and are being studied [48].
Vitamin E or α-tocopherol is a highly potent lipophilic antioxidant which has been studied for AD therapy [49, 50]. Owing to its highly lipophilic nature, Vitamin E is said to cross the BBB and at therapeutic doses, is able to lower the Aβ deposition and lipid peroxidation [51]. However, conflicting results were observed for dietary supplementation of vitamin E. No benefit or no considerable risk reduction was seen in AD therapy [52]. These disappointing conclusions have been postulated to be obtained due to the wrong dosage, timing or unbalanced monotherapy of vitamin E.
Melatonin plays an important role in regulating the circadian rhythm of the body, mitigates reactive oxygen species (ROS) and reactive nitrogen species (RNS) production [37] and is known to promote the antioxidant enzyme activity [53, 54]. Also it has been shown to decrease the Aβ levels and tau hyperphosphorylation [55]. All these advantages have leaded the researchers to study various compounds having multifarious effects of compounds like melatonin-donepezil hybrids [56].
Though all these antioxidants have been found to be biocompatible and well tolerated, yet they have shown low potential in the successful treatment of AD. Few of the many reasons are inadequate therapy intervals, doses, insufficiency to counter oxidative stress, etc [53, 57, 58, 59].
Selenium is an essential mineral having several physiological roles in growth and function of cells. It helps in resisting free radical initiated cell damage and thus was studied for its usefulness in AD [53, 60]. Selenoprotein (SELENOP) is a type of heparin-binding glycoprotein which is known to be a major transporter of Se in mammals [61]. It has the capacity of inducing antioxidant enzyme activity and possesses signalling fuctions via neuronal ApoER2. However, clinical studies have shown severe adverse reactions due to Se toxicity such as alopecia and dermatitis [62]. Various studies have suggested that, CTs if carried out in populations of appropriately low Se statues (majorly in European Populations), may lead to novel strategies in the treatment of AD [63].
Ebselen is another molecule which acts similarly as glutathione peroxidase and provides protection to the neuronal cells [53]. Additionally it also provides anti- inflammatory effect and reduces iron provoked tau phosphorylation for the purpose of treating AD [64]. Selenpezil (a combination of Ebselen and Donepezil) was studied and was found to exhibit no toxicity at higher doses unlike Ebselen [37].
Neferine is a bisbenzylisoquinoline natural alkaloid (ID7) extracted from lotus plant (Nelumbo nucifera) which offers a considerable amount of cytoprotective efficacy in the treatment of AD. Neferine showed significant BACE-I, AChE and BuChE inhibitory activity [65].
Tramiprosate (Homotaurine) is a natural amino acid present in seaweed. It is an aminosulphonate compound which is found in different varieties of marine red algae [66]. Tramiprosate acts by binding to the soluble Aβ, without binding to fibrillar Aβ as well as maintains Aβ in random α-helical conformation thus decreasing the Aβ burden in transgenic mice in the preclinical studies [67]. Additionally, Tramiprosate did not show mutagenic or clastogenic activities in non-clinical genotoxicity and safety pharmacology testing [68]. Tramiprosate was able to cross the BBB without accumulation in the brain. It reduced the amyloid burden by almost 29% [67]. Although Tramiprosate was well tolerated, safe to use and showed minimum toxicity and side effects, it was withdrawn in phase III CTs since it showed low potency, low CNS bioavailability [14] and was not found sufficiently efficacious to be used in AD treatment [14, 66].
Monoclonal Antibodies (mAbs) are the antibodies having monovalent affinity in which they bind to the same epitopes [69, 70]. Humanized mAbs are obtained from non-human species whose protein sequences have been structurally modified for the purpose of increasing their similarity with antibody variants which are produced naturally in humans [71]. Some of these humanized mAbs are discussed below for their potential therapeutic activity to provide symptomatic relief in AD.
Solanezumab is a mAb (wiki) which was being studied as a neuroprotective agent in the treatment of AD [14]. It acts by binding itself with Aβ peptides to reduce Aβ aggregation which is one of the major causes of formation of plaques in AD brain. Solanezumab was expected to show cognitive improvement in mild to moderate AD patients however, in phase III CT it failed to demonstrate improvement in the cognition and was withdrawn [4]. This molecule is now being studied for other diseases related to the amyloid aggregation such as Down’s syndrome.
Bapineuzumab is another humanized mAb [14] which showed positive results in phase II CT for treatment of mild to moderate AD [72]. It has been shown to lower the key biomarkers of AD like the Aβ brain plaques and hyperphosphorylated tau proteins. However, no significant efficacy was observed on cognition as well as the daily activities performed by the patients and hence was withdrawn in phase III CTs [14].
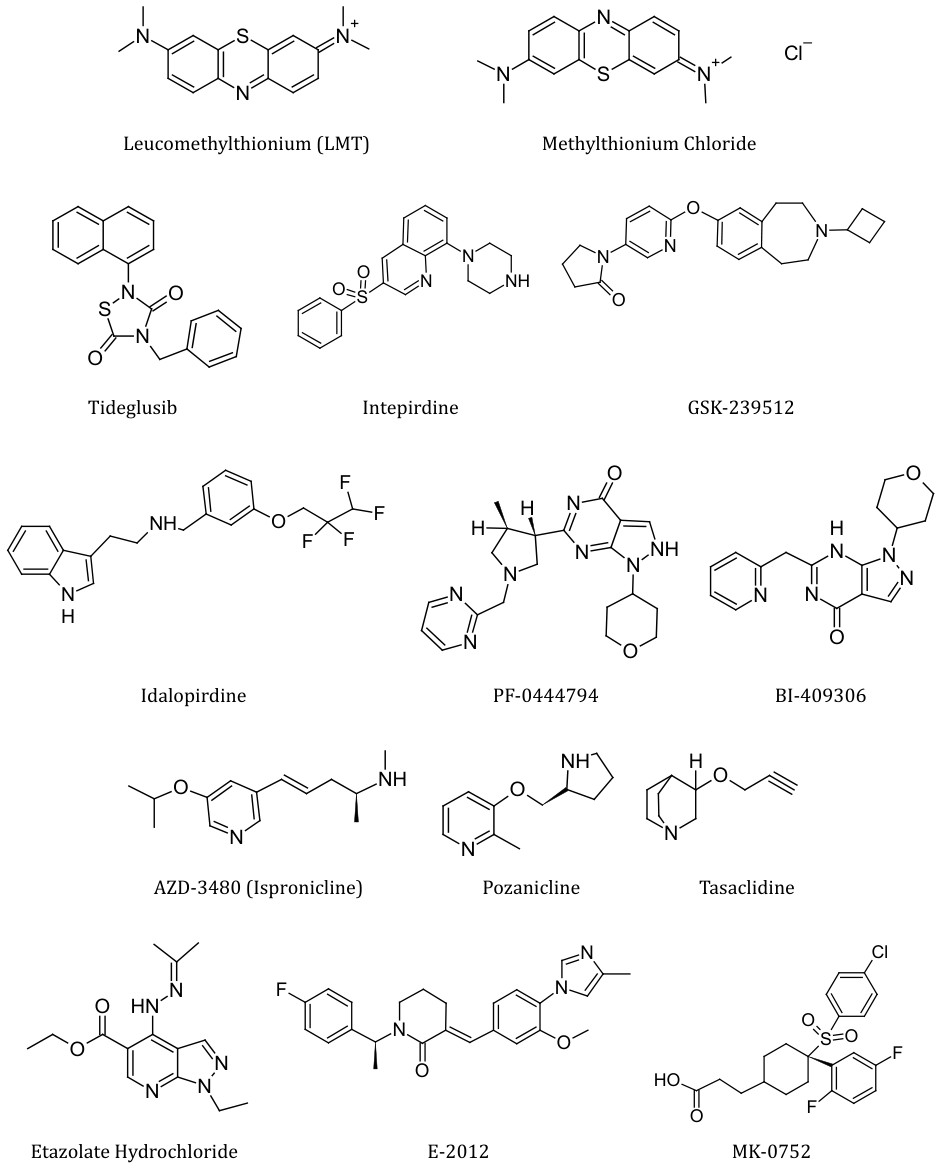
AN-1972 was used in passive immunotherapy as a potential agent helpful in lowering the Aβ levels in the brain. Passive immunotherapy targets lowering the risks involved in development of toxic side effects exerted by a particular drug molecule under CTs [73]. However, it was observed that almost 6% of the vaccinated subjects encountered meningoencephalitis during phase II CTs due to which the molecule was withdrawn from any further clinical assessment as it failed to meet the expectations of having a role in the treatment of AD [4, 14]. Affitope AD-01 and Affitope AD-02 were two molecules whose tolerability, safety and efficacy was checked via subcutaneous route in CTs done from 2007 to 2010. AD vaccines are known to use mimotopes or affitopes of the N-terminal end of Aβ as the antigenic component in the vaccine. The Affitope works by itself and behaves as an antigen to elicit response in the form of antibodies which then specifically target the original antigen present in the body. However only the phase I CT for this molecule was conducted and no results have yet been published officially. GSK-933776 is an anti-β amyloid monoclonal antibody which was directed against the amino terminus of Aβ.71 It has been tested under phase I CT, however, due to some unknown reasons, the studies were discontinued after this stage. Pre-clinically, the molecule showed excellent results in terms of tolerability. Davunetide (AL-108, NAP) was another potential drug for use in treatment of AD as well as cognitive impairment in schizophrenia and pathological neuropathies. It was being studied via different routes of administration like oral, subcutaneous route [74] intranasal [14] and intravenous injections [75]. Phase II studies of Davunetide showed positive cognitive effects and better tolerability, however, confirmation for safe usage of the drug was not obtained and hence it did not pass the phase II CT for the treatment of mild to moderate AD. Methylthionium (MT) acts as an inhibitor of tau aggregation [14]. It can exist either in the reduced form Leucomethylthionium (LMT) or the oxidized form wherein it gets converted to the chloride salt namely Methylthionium Chloride (MTC). MTC form is also called as ‘methylene blue [76]. MT is a redox molecule and at equilibrium exists in the oxidized or reduced forms based on the environmental conditions including factors like pH, reducing agents, oxygen, etc. The phase II studies were conducted which showed that In vivo brain levels for total MT in mouse were four times greater than for oral administration of reduced form than MT at low doses. Clinical efficacy of MTC was found to be hampered after 24 and 50 weeks and was said to be due to dissolution impairment and food effect. Dose absorption rate also was observed to be decreasing over a period of time [76]. On account of these results, the studies were discontinued after phase II due to lack of efficacy. GSK-3β Inhibitors GSK-3β (Glycogen Synthase Kinase 3) β is an enzyme with proven role and major importance in the pathology of AD.77 Tideglusib (NP-031112) was a thiadiazolidinone shown to inhibit GSK-3β enzyme non- competitively to reduce levels of phosphorylated tau in the brain. It was also found to prevent neuronal death and cognitive shortfall in animals. This drug was tested in phase II CTs and the results implied that it was insufficiently efficacious and could not be used for treating mild to moderate AD since it showed no cognitive improvements [77].
Two other marine natural compounds namely the alkaloid Manzamine, and the sesquiterpene palinurin have also failed as GSK3β inhibitors [78]. Many studies reported that low - dose Lithium may be considered as a potential treatment for agitation in AD [14]. Since there is no FDA approved treatment for agitation in AD [79] studies were conducted to design treatment strategies to nullify the agitation symptoms in AD patients.
However, few cases also reported that Lithium was found ineffective in the treatment of behavioural problems in dementia additionally producing extrapyramidal side effects [81]. It was also found that long term use of Lithium over decades lead to the deficiency of thyroid hormone [81]. Thus Lithium is not being used in treatment of AD [82].
5HT-6 Inhibitors are generally involved in disorders like anxiety, depression, epilepsy and obesity [78]. This receptor belongs to the family of G-protein coupled receptors and displays seven transmembrane domains [83]. Blockage of 5HT-6 receptors results in stimulation of ACh release. Therefore, inhibition of 5HT-6 receptors is a potential strategy in the treatment of AD [84] and many potential drugs inhibiting 5HT-6 have been studied as mentioned ahead.
Intepirdine (SB-742457) is a 5HT-6 blocker, completed phase I CTs with no demonstration of adverse effects [85].
Three studies were further performed in phase II CTs with some improvement in global function being observed but without improvement in cognitive function [86]. Intepirdine was also studied as an add on treatment with Donepezil and showed improvements for 48 weeks. However it was not able to meet the primary endpoint for Clinical Dementia Rating (CDR) scale and hence, further testing was not performed. It reached phase III CTs but was withdrawn due to lack of efficacy and activity [85].
Idalopirdine is another 5HT antagonist initially used in the treatment of schizophrenia [85]. It acts by blocking the 5HT receptors and increasing the overall acetylcholine concentrations in the body. Idalopirdine showed improvements in cognitive functioning when used as an adjunct with Donepezil and qualified for the phase II testing, however, the secondary endpoints were not met. Based on the results of phase II trials, phase III trials were conducted but the results showed no improvements in the cognitive functions. Hence further testing for idalopirdine was terminated.
PUFAs (polyunsaturated fatty acids) have anti- inflammatory activities and are being studied for their neuroprotective effects which can contribute towards amyloid clearance and may be useful in the treatment of dementia [87]. These include α-linolenic acid (ALA), eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) [88].
Serum ALA levels were found to be inversely associated with the risk of incapacitating dementia [89], however, the results were statistically insignificant. EPA and DHA were able to elevate membrane fluidity to produce a marked increase in the sAPPα levels, the enzyme reponsible for modulating α and β secretase enzyme [90], which ultimately results in an increase in Aβ clearance.
Transthyretin is also another molecule associated with this category which acts by binding to the free Aβ and reducing the overall levels of Aβ [87]. However, studies have shown that there was no significant improvement in the cognitive as well as normal functioning of the brain and hence, the idea of usage of these PUFAs in the treatment of AD was withdrawn [91].
PF-04447943 is a recently developed molecule, known to be a potent, selective, phosphodiesterase 9A (PDE9A) inhibitor [92]. It is known to elevate cyclic guanosine monophosphate (cGMP) in the brain and cerebrospinal fluid (CSF). The inhibition of PDE9A resulted in enhancement of synaptic plasticity, improvement and stability in pre-clinical cognition models and prevented the decrease in dendritic spine density in transgenic mice. The phase II CTs was conducted to analyse the efficacy, safety and the pharmacokinetics of the molecule in mild to moderate AD. However, the results showed that this molecule demonstrated severe gastrointestinal adverse effects including diarrhoea and nausea. Therefore, the study of this molecule was discontinued after the phase II of clinical assessment [14]. Ispronicline (AZD-3480) is a selective agonist of the central α4β2 and α2β2 neuronal nicotinic cholinergic receptors (NNCRs) [93]. It was suspected that the drug had the potential to bring improvements in cognitive functioning of the brain. However, the phase II CTs suggested that neither the combination of AZD3480 and donepezil nor AZD3480 alone showed any significant improvements in the cognitive functioning in mild to moderate AD. The phase II CTs concluded in 2014 and further assessment and analysis was discontinued for this molecule [93].
Pozanicline (ABT-089) is another nAChR agonist. This molecule also exhibits selectivity for the α4β2 NNCRs. Stimulation of these receptors results in elevation of ACh levels which in turn increase the Aβ clearance [93]. A phase II clinical study was performed to check the pharmacokinetics, safety and tolerance of the drug in mild to moderate AD. Even though the drug presented good tolerability and was safer for usage, it was not sufficiently efficacious [94].
Etazolate Hydrochloride (EHT-0202) is a novel entity found to increase α-secretase activity, PDE4 inhibitory activity, as well as GABA-A receptor modulating activity [95]. A phase-IIA CT was conducted for this molecule to evaluate safety and tolerance levels and was found to be safe and well tolerated. However, it lacked significant efficacy. Also a number of dose dependent adverse effects related to CNS were observed due to which the usage of EHT-0202 in the treatment of mild to moderate AD was discontinued. γ-secretase plays an important role in the final processing of APP for Aβ generation and the inhibitors of this enzyme block the effects of γ-secretase thereby inhibiting the Aβ production. However, almost all these γsecretase inhibitors showed hematological and gastrointestinal toxicity and were withdrawn.
E-2012 is a γ-secretase modulator which was studied for the ability to decrease Aβ. Pre-clinical studies showed occurrence of induced cataract in rats after repeated doses. It was disqualified in phase II CTs for the treatment of mild to moderate AD due to lack of efficacy [96]. MK-0752 is another γ-secretase inhibitor which reduces the production of Aβ. This molecule reached phase I CTs however, was withdrawn since it showed severe side effects of haematological and gastrointestinal toxicity [14]. This molecule was also involved in the notch signalling pathway and skin reactions and change in hair colour were some effects caused due to interference with the notch signalling pathway.
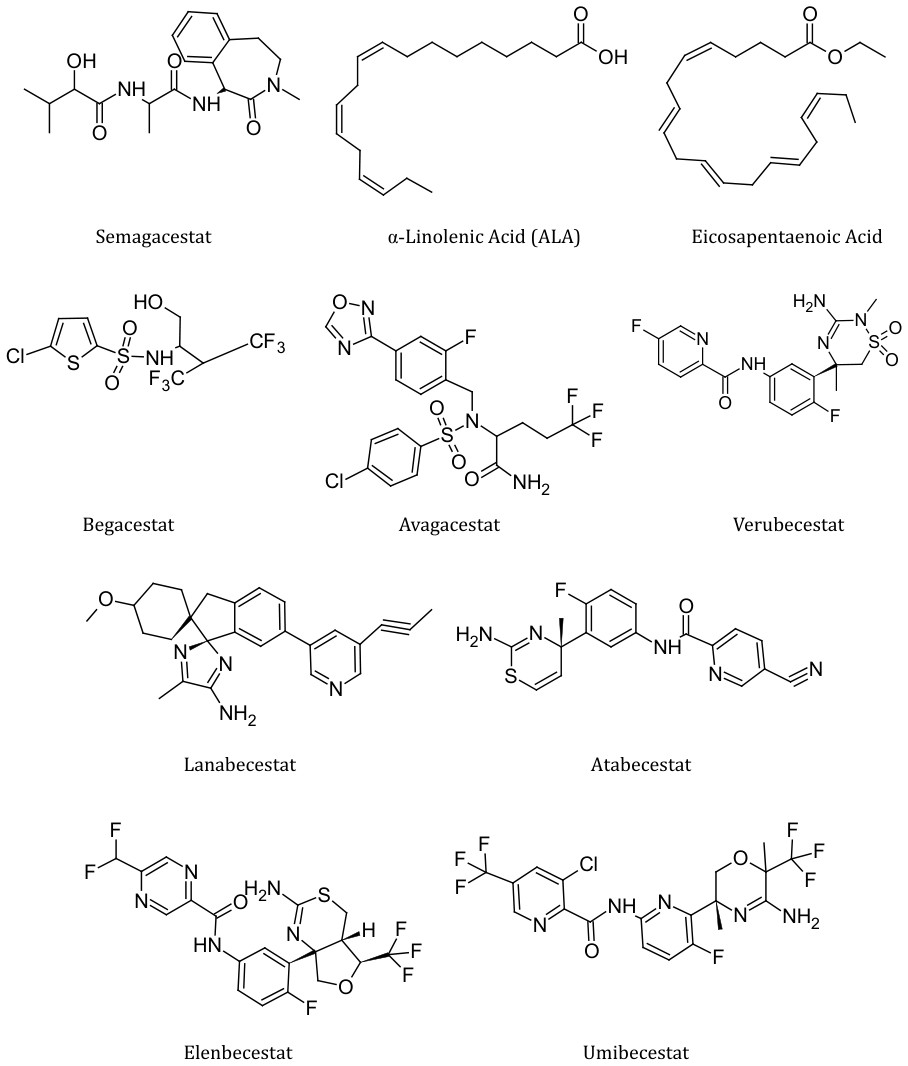
Semagacestat is a γ-secretase inhibitor [14]. Phase I and phase II CTs showed a decrease of plasma Aβ within 3 hours after administration, but an increase of 300% 15 hours post administration. No increases were seen in CSF and as a result phase III studies were continued using higher doses. The drug failed to succeed in the phase III of CTs because it not only failed to slow the disease progression but also worsened the clinical measures of cognition [4, 14]. Begacestat was studied in phase I CTs in patients with prodromal or mild to moderate AD [97]. It decreased the Aβ plasma concentrations substantially but did not change the CSF levels of Aβ. Begacestat failed to show any improvement in the cognitive functioning and was withdrawn at phase I CTs. The results have not yet been published officially. Avagacestat (BMS-708163) is a novel γ-secretase inhibitor. It was clinically tested in combination with the AChE inhibitors for higher therapeutic action and efficacy [4]. However, in phase II CTs, it failed to show significant effects in slowing the rate of progression of AD and did not met the requirements of decreasing the symptomatic effects of AD as well, hence the study was terminated after the phase II CTs [14, 98]. Verubecestat is a BACE-I inhibitor that has been studied for its ability to reduce Aβ [14]. It reduced Aβ and sAPP in the CSF of healthy adults who were administered with verubecestat for two weeks, as well as in patients suffering from mild to moderate AD within one week [99]. However, the trial which was conducted to test the efficacy of verubecestat showed a failure in the early 2017. A second trial was also conducted to test verubecestat in prodromal AD which also encountered failure due to lack of efficacy [4]. It was observed that there was no effect on slowing the disease progression; the clinical studies were halted in phase III CTs [100].
Lanabecestat was also studied and was under two CTs for early AD and mild to moderate AD respectively [4]. However, in mid-2018 it failed the interim futility analysis due to which both the CTs were halted and no further studies were done on this molecule. The official results are yet to be published [4]. A similar molecule Atabecestat was also developed and studied under phase II and phase III CTs. It produced the same effects as that of Verubecestat and lowered the Aβ concentrations by BACE-I inhibition. Both the phase II studies were conducted to study the safety profile of the drug and efficacy on long term usage and the early phase III trials to investigate the beneficial effects of atabecestat on the cognitive functioning [101], failed to show any positive results. In addition to this, hepatotoxicity was also seen as a severe side effect of this drug and therefore, further studies were terminated [4]. Elenbecestat was also another BACE-I inhibitor and also showed a marked decrease in Aβ levels in the initial stages. But, the common side effect of all the BACE-I inhibitors i.e hepatotoxicity was also seen in Elenbecestat.
Umibecestat (CNP-520) is another example of BACE-I inhibitor which has undergone phase II CTs but the trials were discontinued due to the worsening of cognitive functioning as well as various adverse events. Thus BACE-I inhibitors are not considered as a potential treatment in mild to moderate AD as well as for the prodromal AD due to a number of severe side effects demonstrated by them.
Nerve Growth Factors (NGFs) are responsible for the overall growth, development, maintenance and survival of the target neurons in mammalian brain. The basic structure is that of a glycoprotein consisting of three subunits – inactive (αNGF), biologically active (βNGF) and γNGF which is responsible for the conversion of the NGF precursor to the mature form. In AD patients, NGF levels are increased as observed in many clinical and preclinical studies. Pre-CTs showed an increase in cognitive functions when experimented on rats [102]. In humans, after 12 months of treatment with NGF, there was an improvement seen in the cognitive functioning and a marked decrease in Aβ.
However, the patients showed symptoms of brain atrophy which might be caused due to an increase in hyperphosphorylated tau. The side effects also included back pain [14]. Additionally it was also found that the treatment with Valproate showed a decrease in nuclear factor kappa. The final call on the usage of NGF as a potential treatment in mild to moderate AD is yet to be officially published.
Bryostatin-I is known to be a potent modulator of protein kinase C (PKC) by activation of α-secretase [14]. It showed therapeutic activity in preclinical studies on rats and hence was introduced into CTs. A double blind placebo controlled phase II CT was conducted for Bryostatin-I in the year 2015 and the study was completed in 2018. The subjects were administered with bryostatin-I through IV route. Due to adverse events, low tolerability and low efficacy, the study did not provide positive results on the usage of Bryostatin-I as a potential treatment in AD. Bryostatin was already investigated as an anti-cancer agent and was known to reduce Aβ levels and had shown memory improvement in rats and also had shown positive results in phase I CTs, however, phase II CTs did not show positive results in terms of safety and tolerability in the patients and were halted [103].
ABT-288 is a known selective H2 antagonist and was under experimentation for the treatment of mild to moderate AD. This molecule underwent phase II CTs which were designed to evaluate the safety and efficacy of the molecule at two doses [104]. However, the results on efficacy of the drug did not meet the futility criteria. Therefore further studies were discontinued for this molecule [14].
GSK-239512 is a H3 antagonist which has undergone phase II CTs. It is a novel entity and was designed for the treatment of cognitive dysfunctioning in patients suffering from mild to moderate AD. However, the studies were discontinued for this molecule due to failure in improvement of memory [105]. Talsaclidine is a selective muscarinic M1 receptor agonist. It was found to play an important role in lowering the levels of Aβ [40, 41, 42] by modulating the activity of proteases that cleave the APP [106]. This molecule was tested in phase I CTs and the study was further discontinued when the results showed undesirable cholinergic receptor mediated side effects [14].
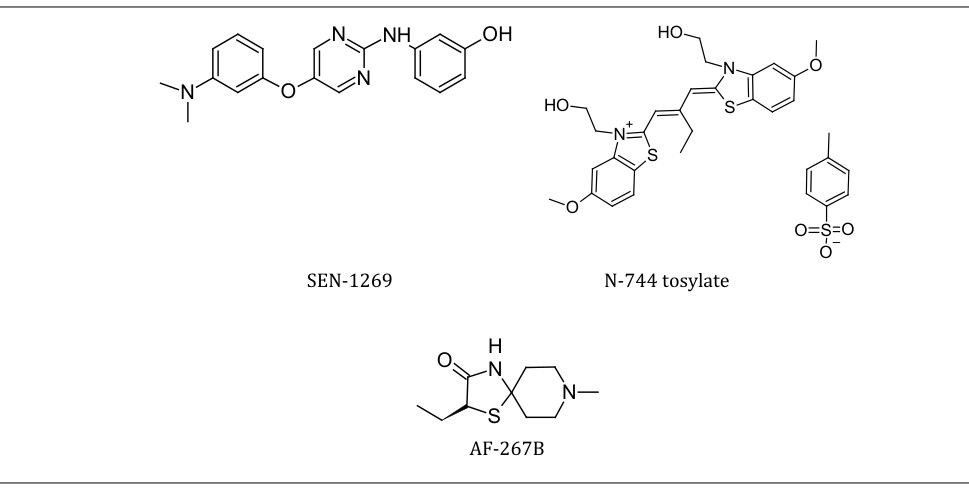
BI-409306 is a PDE4 inhibitor which was clinically tested for cognitive improvement in patients suffering from mild to moderate AD [107]. However, this molecule did not show significant improvement in cognitive behaviour and instead showed many adverse effects on the subjects. Hence, the clinical studies were halted for this molecule in phase II of the clinical assessment [105]. Drugs like RS-0406, SEN-1269, SP- 233, Exebryl-1, NGX, GSM-1, BBS-1 are some more examples of drugs which have failed in entering the early stages of the clinical trials [14].
PBT2 is yet another investigational drug candidate and is believed to be a successor to Clioquinol. PBT2 being a copper/zinc ionophore is known to rapidly restore cognition in the pre-clinical studies conducted on mice [108]. In phase II CTs it has shown to increase the Aβ clearance and produced a marked decrease in the Aβ concentrations in the subjects. In a recent small double blinded study, PBT2 failed to show efficacy and therefore it is currently not in CTs [109].
OH O
O
O
O
O
O O
O
OH H
O OH
O
O
OH O
O
O
O H
O O H
Bryostatin – I Palinurin
Docosahexaenoic Acid (DHA)
Drugs Withdrawn At Pre-Clinical Stage
The results of pre-clinical trials are always an indication of whether or not the drug is safe for usage in humans. However many drug molecules were withdrawn from the preclinical stage itself due to many reasons including severe toxicity, bioavailability issues, pharmacokinetics, adverse effects, etc.
Molecules like Phenylthiazolylhydrazides, Rhodanines, Minocycline, N-744 tosylate; Brain Derived Neurotrophic OH O H O OH OH OH N O S N H2 S O N H H N O OH Factor (BDNF), Ladostigil, AF-267B, M-30, etc are few molecules which were not successful in the preclinical studies for the treatment of mild to moderate AD. These molecules fall in the category of tau anti-aggregants, γ-secretase inhibitors, etc [4, 14, 105].
Peptidic antiaggregants are another class of molecules which are responsible for lowering the concentrations of the APP via several pathways, which also demonstrated various adverse and side effects in the pre-clinical stages.
NH O N
O
Rhodanine Minocycline Ladostigil
Investigational and Experimental Drugs currently in Clinical Trials
Homocysteine levels are elevated in patients suffering from AD. Therefore, hyperhomocysteinemia might contribute directly or indirectly in the pathology of AD by neurotoxic processes [32, 110].
AAB-003 is an Fc-engineered Bapineuzumab and its safety and tolerability is currently under investigation in phase I CTs [71].
Nicotinamide is the biologically active form of vitamin B3 (Niacin) [14]. It is known to decrease the phosphorylated tau levels in the patients suffering from mild to moderate AD via inhibition of microtubule polymerisation [111]. The phase II CT is still on going for the use of nicotinamide in AD therapy. The study is estimated to be completed in July 2020. Phase II/III CTs are being conducted on the use of combination of Donepezil with EGCG vs placebo to be used in treatment of this condition. Also, combination of Rivastigmine and MTC (Methylthionium Chloride) is being studied for obtaining better bioavailibility and improvement in the activity of the drug [14]. To combat the problems faced due to lithium in the treatment of agitation in AD, another strategy of combination of lithium with antipsychotics or antidepressants like Citalopram is being studied [82]. The success of the strategy is yet to be evaluated and is under investigation.
Azeliragon (TTP-448) is an inhibitor of Receptor for Enhanced Glycation Endproducts (RAGE) [4], which is a transmembrane receptor of the immunoglobin group widely exhibited by the endothelial cells and microglia that are upregulated in AD [112]. Aβ is a known ligand for RAGE which plays a role in the promotion of Aβ influx into the brain thereby disrupting the blood brain barrier integrity [14]. A phase II study of Azeliragon was conducted and it was observed that the cognitive functions were improved for 18 months in mild to moderate AD patients. Phase III trials are also being conducted but the results have not yet been published. The trials are projected to conclude in April, 2023.
Encenicline (EVP-6124) is a novel entity and a highly selective α7 nicotinic ACh receptor (nAChR) partial agonist. It is known that Nicotine shows improvement in attention, learning abilities and memory by interactions with nAChRs. These receptors are highly expressed in the hippocampal region of the brain which plays important role in the formation and storage of memory [113]. Agonists of these receptors have shown a significant increase in the learning and memory formation abilities of the patients. Recent clinical and preclinical studies have shown that it reversed a scopolamine induced deficit, to prevent natural forgetting. The molecule is said to be safe for usage in combination with Donepezil. The drug this undergone phase II CTs and the study was withdrawn before the participants were enrolled. No official records were published.
CTS-21166 is an orally administered compound belonging to the class of β-secretase inhibitors [14]. It is well tolerated in majority of the individuals and reduces plasma Aβ levels. However, the phase I CT results are not yet published officially and the molecule is currently under investigation [114].
PF-3084014 is another novel entity that acts as a γ-secretase inhibitor. It is known to reduce Aβ levels and improve cognition. It has undergone phase I CTs but the results are not yet posted officially. Reasons might be because of insufficient volunteers or safety issues with the drug [14].
SGS742 was a 3-aminopropyl-n-butyl phosphinic acid acting as a GABA(B) antagonist and was synthesized in large scale a IRIX Pharmaceuticals. Phase II CTs were conducted for this molecule to evaluate it’s enhancement in cognitive functioning in mild to moderate AD. The study revealed that this molecule can be considered as a candidate to prove useful in disorders related to cognitive functioning by performing additional clinical studies [115].
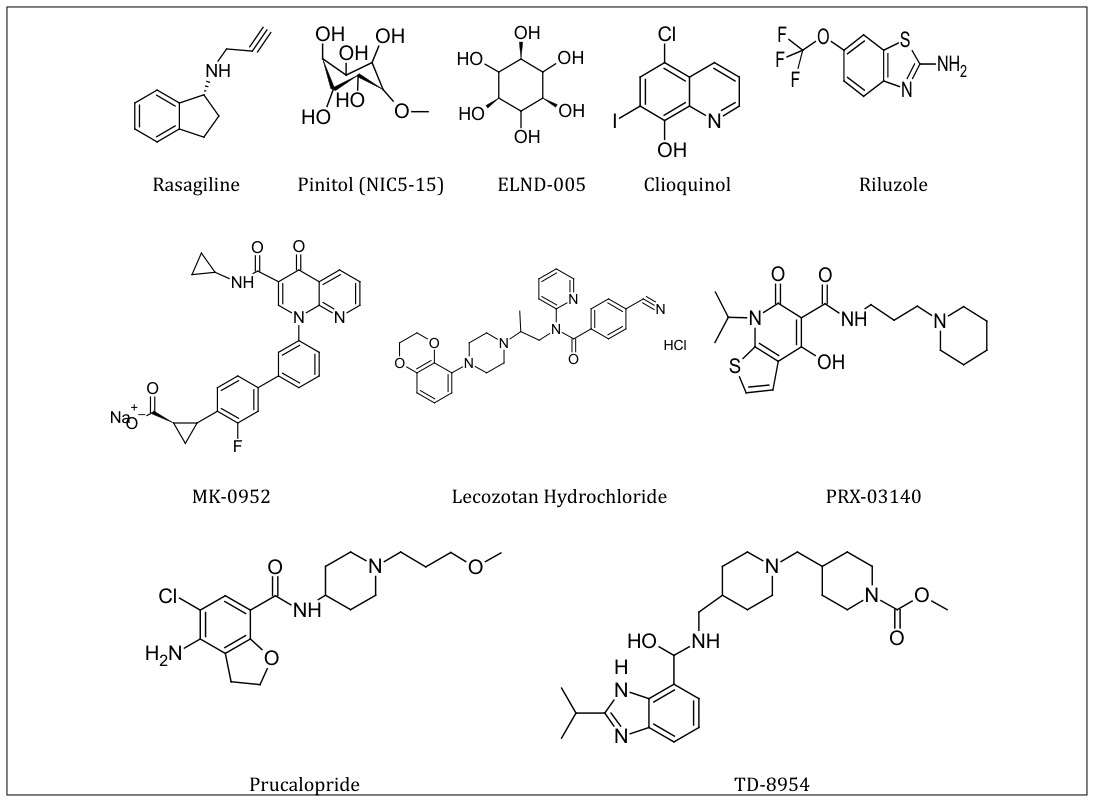
PRX-03140 and Prucalopride are two highly selective 5-HT4 agonists which demonstrated potent binding, brain penetrability and exhibited neuropharmacological properties wherein they increased Ach and histamine release in prefrontal cortex. Currently studied are being carried out to evaluate the extend of both these molecules to improve cognitive functioning in mild to moderate AD [116].
TD-8954 is yet another 5HT4 agonist which has shown better results in improving the cognitive functioning than that of PRX-03140. However, the CNS penetrability of all 5HT4 agonists is comparatively less than that of donepezil. Studies have shown that this drug behaved as a full agonist in the cAMP accumulation a sAPPα secretion assays but exhibited a lower intrinsic activity. The clinical studies for this molecule are yet to be completed [117].
Rasagiline is a selective MAO inhibitor and is under investigation for combination therapy with Rivastigmine to show better tolerance and bioavailability in the treatment of AD [118].
Pinitol (NIC5-15) is a naturally occurring cyclic sugar molecule and has mild insulin sensitizing effects. This molecule is being investigated under the category of chiro- inositols and insulin sensitizing compounds which are already proven to be safe for human use. It also exhibits γ-secretase inhibiting activity.(ID4) It is currently being tested under phase II trials and the results are yet to be published [119].
ELND005, formerly known as AZD-103 is a scyllo-inositol molecule. This molecule is said to have the ability to bind to Aβ and cause misfiling which results in the inhibition of aggregation as well as stimulation of dissociation of the Aβ aggregates [14]. In the pre-clinical studies on animals, it reduced the levels of soluble and insoluble Aβ, reduced plaque burden and glial inflammatory response. Currently it is being studied as an orally administered drug under phase II CTs [14].
CAD-106 is a vaccine under development for potential treatment of AD. It is being investigated as a subcutaneous injection and contains Aβ1-6 peptide bound to a Qβ virus- like particle [14]. This vaccine is being designed such that it can induce Aβ specific antibodies so as to reduce the accumulation of Aβ. Confirmatory CTs are still ongoing and the results are yet to be published.
ACC-001 is another vaccine under investigation and is said to be conjugated to mutated diphtheria toxin protein CRM19 [120]. Currently phase II CTs are going on for studying the long term effects, safety and tolerability of the molecule.
V-950 is also a vaccine being tested as an aluminium containing adjuvant with or without Iscomatrix which is a biological adjuvant of saponin, cholesterol and phospholipids [14]. Currently many mAbs are being tested for passive or active immunization against Aβ.
Ponezumab (PF-04360365) falls under the category of passive immunotherapy and is said to be a humanised, modified IgG2 antibody [14]. This molecule has successfully undergone phase I CTs with minimum signs of adverse events. It has shown good tolerability and is safe to use. Currently it is being investigated for efficacy under phase II CTs.
Crenezumab is another humanised mAb and is said to target monomeric and conformational epitopes. The phase I CTs were conducted with the purpose of analysing the safety, efficacy and tolerability of the drug which was administered intravenously to patients suffering from mild to moderate AD [121, 122, 123]. No adverse effects of the drug were observed in the CTs. This molecule is currently undergoing phase II CTs. The results have not yet been officially published.
Gantenerumab is another humanised mAb and is known to target Aβ [40, 41, 42]. This molecule has reached phase III CTs which are currently ongoing and are expected to be completed in 2022 or 2023.71 like the other mAb molecules; Gantenerumab also aims at lowering the Aβ levels. In the small phase IIa clinical studies, it was given as an intravenous infusion. Two subjects from the 200mg group showed inflammation at focal areas with the highest levels of Aβ reduction. Results showed that this molecule was well tolerated and safe at multiple doses for maximum 12 months [123, 124].
Aducanumab is a human mAb developed by Biogen Inc. which acts by selectively binding to the Aβ fibrils and soluble oligomers [109]. First double- blinded, placebo controlled, single – dose escalation study was conducted on aducanumab in 2011 [125]. This study was conducted for the purpose of testing the safety and tolerability of the molecule in patients suffering from mild-to-moderate AD and the results stated that aducanumab demonstrated an acceptable safety, tolerability and pharmacokinetics at maximum single dose of 30mg/kg (maximum tolerated dose) [126]. However, the most commonly observed side effects were the amyloid related imaging abnormalities [127]. In 2015, Biogen released two identical 18-month phase III studies in order to evaluate the efficacy of the molecule in slowing the cognitive and functional impairment. Overall, the results of this study have supported the idea of continuing the research on studying the potential of aducanumab in the treatment of AD [128].
BAN-2401 is a humanised IgG1 (Immunoglobulin G1) mAb. It was first tested and evaluated in patients for mild to moderate AD. The safety profile of the drug suggests that BAN2401 is well tolerated at single doses upto 15mg/kg and intravenous multiple doses upto 10mg/kg. Currently this molecule is under phase II CTs and the results are yet to be published officially. ACI-24 is again a humanized mAb currently being tested under phase II CTs [14].
UB-311 is a novel Aβ vaccine comprising of two Aβ1-14 targeting peptides which are linked to different helper T-cell peptide epitopes in the form of chimeric peptide to maximise immunogenicity [106]. It is currently being investigated under phase I CTs [14].
R-1450 is another mAb molecule which has been tested under phase I CTs and is said to target the Aβ levels and increase the clearance of Aβ [129, 130].
Metal Chelators with BBB permeability could potentially help reduce the imbalance of metals associated with the brains of AD inflicted populations.
Clioquinol (PBT1) is a metal chelator with the ability to cross the BBB. It has affinity for zinc and copper ions [131, 132]. This molecule was tested for the purpose of expecting an improvement in the cognitive functions in CTs. However, the results of the same are currently limited as the drug is under study [131].
Riluzole is a drug approved for the treatment of amyotrophic lateral sclerosis (ALS). This molecule also acts as an NMDA receptor antagonist due to which it has been under investigation for the treatment of mild to moderate AD. It is an orally administered drug and is currently being evaluated for cognitive functional changes and specific imaging biomarkers. Phase II CTs are being performed under placebo control. The results of the trials are yet to be officially published.
MK-0952 is a phosphodiesterase 4 (PDE4) inhibitor and has been found to be orally bioavailable in the preclinical studies [133]. Its ability to improve cognition has also been tested and compared with other similar molecules like MK-0359 and MK-0873. In a water maze test which was conducted for the above molecules, MK-0952 was observed to improve the performance results.
Lecozotan is a selective 5HT1a receptor antagonist and has completed the phase III CTs in June, 2008. It enhances the potassium stimulated release of ACh and Glutamate.105 It was suggested from the results of the CTs that lecozotan is involved in the cognitive processing since it demonstrated improvement in the cognition of the patients suffering from mild to moderate AD [134].
MABT-5102A was tested for effect on brain Aβ load under phase II CTs. However, official results are yet to be published. It is known to be falling under the category of passive immunization therapy [14].
The chemical features of these drugs included in this review, when taken into account in the initial stages of drug discovery may have implications in accelerating drug discovery for AD therapeutics. There have been so many failures associated with the CTs of many drugs for therapy of AD. However there is a big pipeline of drugs still awaiting their CT results which offers a ray of hope that atleast some of these drugs might someday be introduced as drugs for therapy of AD.
This review takes into account the drugs that have been tested till date or are currently under CTs for therapy of AD.
References
-
Dementia (2021) World Health Organization.
-
Masters CL, Bateman R, Blennow K, Rowe CC, Sperling RA, et al. (2015) Alzheimer’s disease. Nat Rev Dis Primers 1: 15056-15058.
-
Agatonovic-Kustrin S, Kettle C, Morton DW (2018) A Molecular Approach in Drug Development for Alzheimer’s Disease. Biomed Pharmacother 106: 553- 565.
-
Fish PV, Steadman D, Bayle ED, Whiting P (2019) New Approaches for the Treatment of Alzheimer’s Disease. Bioorganic Med Chem Lett 29(2): 125-133.
-
Lou YH, Wang JS, Dong G, Guo PP, Wei DD, et al. (2015) The acute hepatotoxicity of tacrine explained by 1H NMR based metabolomic profiling. Toxicol Res 4(6): 1465- 1478.
-
Watkins PB, Zimmerman HJ, Knapp MJ, Gracon SI, Lewis KW (1994) Hepatotoxic effects of tacrine administration in patients with Alzheimer’s disease. JAMA 271(13): 992-998.
-
Zhang P, Xu S, Zhu Z, Xu J (2019) Multi-Target Design Strategies for the Improved Treatment of Alzheimer’s Disease. Eur J Med Chem 176: 228-247.
-
Zambrano P, Suwalsky M, Rzeminska MJ, Strzalka K, Sepúlveda B, et al. (2019) The Acetylcholinesterase (AChE) Inhibitor and Anti-Alzheimer Drug Donepezil Interacts with Human Erythrocytes. Biochimica et Biophysica Acta (BBA)-Biomembranes 1861(6): 1078- 1085.
-
Zhu G, Wang K, Shi J, Zhang P, Yang D, et al. (2019) The Development of 2-Acetylphenol-Donepezil Hybrids as Multifunctional Agents for the Treatment of Alzheimer’s Disease. Bioorganic Med Chem Lett 29(19): 126625.
-
Chauhan MK, Sharma PK (2019) Optimization and Characterization of Rivastigmine Nanolipid Carrier Loaded Transdermal Patches for the Treatment of Dementia. Chem Phys Lipids 224: 104794.
-
De Vito EE, Carroll KM, Babuscio T, Charla Nich, Sofuoglu M (2019) Randomized placebo-controlled trial of galantamine in individuals with cocaine use disorder. Journal of Substance Abuse Treatment 107: 29-37.
-
Mufamadi MS, Kumar P, du Toit LC, Choonara YE, Obulapuram PK, et al. (2019) Liposome-Embedded, Polymeric Scaffold for Extended Delivery of Galantamine. Journal of Drug Delivery Science and Technology 50: 255-265.
-
Ameen D, Michniak-Kohn B (2019) Development and in Vitro Evaluation of Pressure Sensitive Adhesive Patch for the Transdermal Delivery of Galantamine: Effect of Penetration Enhancers and Crystallization Inhibition. Eur J Pharm Biopharm 139: 262-271.
-
Rafii MS, Aisen PS (2019) Alzheimer’s Disease Clinical Trials: Moving Toward Successful Prevention. CNS Drugs 33(2): 99-106.
-
Mangialasche F, Solomon A, Winblad B, Mecocci P, Kivipelto M (2010) Alzheimer’s Disease: Clinical Trials and Drug Development. Lancet Neurol 9(7): 702-716.
-
Wang R, Yan H, Tang XC (2006) Progress in Studies of Huperzine A, a Natural Cholinesterase Inhibitor from Chinese Herbal Medicine. Acta Pharmacol. Sin 27(1): 1-26.
-
Zhao Q, Tang XC (2002) Effects of Huperzine A on Acetylcholinesterase Isoforms in Vitro: Comparison with Tacrine, Donepezil, Rivastigmine and Physostigmine. Eur J Pharmacol 455 (2-3): 101-107.
-
Shutske GM, Pierrat FA, Cornfeldt ML, Szewczak MR, Huger FP, et al. (1998) (±)-9-Amino-1,2,3,4- Tetrahydroacridin-1-Ol. A Potential Alzheimer’s Disease Therapeutic of Low Toxicity. J Med Chem 31 (7): 1278- 1279.
-
Pang YP, Quiram P, Jelacic T, Hong F, Brimijoin S (1996) Highly potent, selective and low cost bis- tetrahydroaminacrine inhibitors of acetylcholinesterase. Steps toward novel drugs for treating Alzheimer’s disease. J Biol Chem 271(39): 23646-23649.
-
Hu MK, Wu LJ, Hsiao G, Yen MH (2002) Homodimeric tacrine congeners as acetylcholinesterase inhibitors. J Med Chem 45(11): 2277-2282
-
Product information. Avandia (rosiglitazone). Research Triangle Park, NC: GlaxoSmithKline, 2011.
-
Product information. Actos (pioglitazone). Deerfield, IL: Takeda Pharmaceuticals America Inc., January 2011.
-
Yki-Jarvinen H (2004) Thiazolidinediones. N Engl J Med 351(11): 1106-1118.
-
Landreth G (2006) PPARgamma agonists as new therapeutic agents for the treatment of Alzheimer’s disease. Exp Neurol 199(2): 245-248.
-
Miller BW, Willett KC, Desilets AR, (2011) Rosiglitazona y Pioglitazona Para El Tratamiento de La Enfermedad de Alzheimer. Ann Pharmacother 45(11): 1416-1424
-
Klein J (2007) Phenserine. Expert Opin Investig Drugs 16(7): 1087-1097.
-
Wu J, Qin Li, Bezprozvanny I (2008) Evaluation of dimebon in cellular model of Huntington’s disease. Mol Neurodegener 3: 15.
-
Blanchard JW, Tsai LH (2019) Unraveling the Paradox of Statins with Human Neurons: New Leads in Alzheimer’s Disease. Cell Stem Cell 24 (3): 347-349.
-
Hull MA (2014) Alzheimer’s Disease Mortality and Patient Retention in Clinical Trials: The Impact of Alzheimer’s Disease on Mortality. Global Clinical Trials for Alzheimer’s Disease pp: 179-195
-
Sano M (2010) Tarenflurbil: Mechanisms and Myths. Arch Neurol 67(6): 750-752.
-
Eid A, Richardson JR (2019) Pharmacoepigenetics and Pharmacoepigenomics of Valproate in Neurodegenerative Disease. Pharmacoepigenetics 10: 801-816.
-
Tariot PN, Raman R, Jakimovich L, Schneider L, Porsteinsson A, et al. (2005) Divalproex Sodium in Nursing Home Residents with Possible or Probable Alzheimer Disease Complicated by Agitation: A Randomized, Controlled Trial. Am J Geriatr Psychiatry 13(11): 942-949.
-
Mecocci P, Polidori MC (2012) Antioxidant Clinical Trials in Mild Cognitive Impairment and Alzheimer’s Disease. Biochim Biophys Acta 1822(5): 631-638.
-
Mariani E, Polidori MC, Cherubini A, Mecocci P (2005) Oxidative stress in brain aging, neurodegenerative and vascular diseases: an overview. J Chromatogr B Analyt Technol Biomed Life Sci 827(1): 65-75.
-
Mangialasche F, Polidori MC, Monastero R, Ercolani S, Camarda C, et al. (2009) Biomarkers of oxidative and nitrosative damage in Alzheimer’s disease and mild cognitive impairment. Ageing Res Rev 8(4): 285-305.
-
Penumala M, Zinka RB, Shaik JB, Mallepalli SKR, Vadde R, et al. (2018) Phytochemical profiling and in vitro screen¬ing for anticholinesterase, antioxidant, antiglucosidase and neuroprotective effect of three traditional medicinal plants for Alzheimer’s Disease and Diabetes Mellitus dual therapy. BMC Complement Altern Med 18(1): 77.
-
Budni J, Santos TB, Mina F, Garcez ML, Zugno AI (2015) The Involvement of BDNF, NGF and GDNF in Aging and Alzheimer’s Disease. Aging Dis 6(5): 331-341.
-
Obulesu M (2019) Antioxidants in Alzheimer’s Therapy. Alzheimer’s Dis. Theranostics: 13-18.
-
Caruana M, Cauchi R, Vassallo N (2016) Putative role of red wine polyphenols against brain pathology in Alzheimer’s and Parkinson’s disease. Front Nutr 3: 31.
-
Prasad S, Aggarwal BB, Benzie IFF, Galor SW (2011) Turmeric, the golden spice: From traditional medicine to modern medicine. In Herbal Medicine: Biomolecular and Clinical Aspects. 2nd (Edn.), Chapter 13. CRC Press/ Taylor & Francis.
-
Araujo CC, Leon LL (2001) Biological activities of Cur874 cuma longa L. Mem Inst Oswaldo Cruz 96(5): 723-728.
-
Tang M, Taghibiglou C, Liu J (2017) The Mechanisms of Action of Curcumin in Alzheimer’s Disease. J Alzheimers Dis 58(4): 1003-1016.
-
Xiong Z, Hongmei Z, Lu S, Yu L (2011) Curcumin medi906 ates presenilin-1 activity to reduce _-amyloid production 907 in a model of Alzheimer’s Disease. Pharmacol Rep 63(908): 1101-1108.
-
Huang HC, Tang D, Xu K, Jiang ZF (2014) Curcumin attenuates amyloid-_-induced tau hyperphosphorylation in human neuroblastoma SH-SY5Y cells involving PTEN/ Akt/GSK-3β signaling pathway. J Recept Signal Transduct Res 34(1): 26-37.
-
Ullah F, Liang A, Rangel A, Gyengesi E, Niedermayer G et al. (2017) High bioavailability curcumin: An anti- inflammatory and neurosupportive bioactive nutrient for neurodegenerative diseases characterized by chronic neuroinflammation. Arch Toxicol 91(4): 1623-1634.
-
Reijerkerk A, Gijs Kooij, Susanne vander MAP, Khazen S, Dijkstra CD, et al. (2006) Diapedesis of monocytes is associated with MMP-mediated occludin disappearance in brain endothelial cells. FASEB J 20(14): 2550-2552.
-
Verslegers M, Lemmens K, Hove IV, Moons L (2013) Matrix metalloproteinase-2 and -9 as promising benefactors in development, plasticity and repair of the nervous system. Prog Neurobiol 105: 60-78.
-
Loy CT, Schofield PR, Turner AM, Kwok JBJ (2014) Genetics of dementia. Lancet 383(9919): 828-840.
-
Sawda C, Moussa C, Turner RS (2017) Resveratrol for Alzheimer’s Disease. Ann N Y Acad Sci 1403(1): 142-149.
-
Polidori MC, Stahl W, Sies H, Flohe RB (2007) Vitamin E, metabolism and biological activity of metabolic products, In: Preedy V, Watson R (Eds.), The Encyclopedia of Vitamin E, New York, CAB International 11-20.
-
Iuliano L, Monticolo R, Straface G, Spoletini I, Gianni W, et al. (2010) Vitamin E and enzymatic/oxidative stress- driven oxysterols in amnestic mild cognitive impairment subtypes and Alzheimer’s disease. J. Alzheimers Dis 21(14): 383-1392
-
Sung S, Yao Y, Uryu K, Yang H, Lee VM, et al. (2004) Early vitamin E supplementation in young but not aged mice reduces Abeta levels and amyloid deposition in a transgenic model of Alzheimer’s disease. FASEB J 18(2): 323-325.
-
Zandi PP, Anthony JC, Khachaturian AS, Stone SV, Gustafson D, et al. (2004) Reduced risk of Alzheimer disease in users of antioxidant vitamin supplements: the Cache County Study. Arch Neurol 61(1): 82-88.
-
Mezeiova E, Spilovska K, Nepovimova E, Gorecki L, Soukup O, et al. (2018) Profiling donepezil template into multipotent hybrids with antioxidant properties. J Enzyme Inhib Med Chem 33(1): 583-606.
-
Miller E, Morel A, Saso L, Saluk J (2015) Melatonin redox activity. Its potential clinical applications in neurodegenerative disorders. Curr Top Med Chem 15(2): 163-169.
-
Lahiri DK (1999) Melatonin affects the metabolism of the beta amyloid precursor protein in different cell types. J Pineal Res 26(3): 137-146.
-
Ramos E, Egea J, de Los, Rios C, Contelles JM, et al. (2017) Melatonin as a versatile molecule to design novel multitarget hybrids against neurodegeneration. Future Med Chem 9(8): 765-780.
-
Bournival J, Quessy P, Martinoli MG (2009) Protective effects of resveratrol and quercetin against MPPþ- induced oxidative stress act by modulating markers of apoptotic death in dopaminergic neurons. Cell Mol Neurobiol 29(8): 1169-1180.
-
Pratico D (2008) Oxidative stress hypothesis in Alzheimer’s disease: a reappraisal. Trends Pharmacol Sci 29(12): 609-615.
-
Murphy MP (2014) Antioxidants as therapies: can we improve on nature?. Free Radic Biol Med 66: 20-23.
-
Allmang C, Wurth L, Krol A (2009) The selenium to selenopro¬tein pathway in eukaryotes: more molecular partners than anticipated. Biochim Biophys Acta 1790(11): 1415-1423.
-
Lobanov AV, Hatfield DL, Gladyshev VN (2009) Eukaryotic selenoproteins and selenoproteomes. BBA-Gen Subjects 1790(11): 1424-1428.
-
Lippman SM, Klein EA, Goodman PJ, Lucia MS, Thompson IM, et al. (2009) Effect of Selenium and Vitamin E on Risk of Prostate Cancer and Other Cancers The Selenium and Vitamin E Cancer Prevention Trial ( SELECT). JAMA 301(1): 39-51.
-
Solovyev N, Drobyshev E, Bjørklund G, Dubrovskii Y, Lysiuk R, et al. (2018) Selenium, selenoprotein P, and Alzheimer’s Disease: Is There a Link?. Free Radic Biol Med 127: 124-133.
-
Xie L, Zheng W, Xin N, Xie JW, Wang T, et al. (2012) Ebselen inhibits iron-induced tau phosphorylation by attenuating DMT1 up-regulation and cellular iron uptake. Neurochem Int 61(3): 334-340.
-
Asokan SM, Mariappan R, Muthusamy S, Velmurugan BK (2018) Pharmacological benefits of neferine - a comprehensive review. Life Sci 199: 60-70.
-
Aisen PS, Gauthier S, Ferris SH, Saumier D, Haine D, et al. (2011) Tramiprosate in Mild-to-Moderate Alzheimer’s Disease - A Randomized, Double-Blind, Placebo- Controlled, Multi-Centre Study (the Alphase Study). Arch Med Sci 7(1): 102-111.
-
Gervais F, Paquette J, Morissette C, Krzywkowski P, Yu M, et al. (2007) Targeting Soluble Aβ Peptide with Tramiprosate for the Treatment of Brain Amyloidosis. Neurobiol. Aging 28(4): 537-547.
-
Janus C, Pearson J, McLaurin J, Mathews PM, Jiang Y, et al. (2000) A beta peptide immunization reduces behavioural impairment and plaques in a model of Alzheimer’s disease. Nature 408(6815): 979-982.
-
Morgan D (2011) Immunotherapy for Alzheimer’s disease. J Intern Med 269(1): 54-63.
-
Reichert JM (2013) Which are the antibodies to watch in 2013?. MAbs 5(1): 1-4.
-
Prins ND, Scheltens P (2013) Treating Alzheimer’s Disease with Monoclonal Antibodies: Current Status and Outlook for the Future. Alzheimer’s Res Ther 5(6): 56.
-
Salloway S, Sperling R, Gilman S, Fox NC, Blennow K, et al. (2009) A phase 2 multiple ascending dose trial of bapineuzumab in mild to moderate Alzheimer disease. Neurology 73(24): 2061-2070.
-
Yi K (2014) Passive immunotherapy - a viable treatment for Alzheimer’s disease. Psychiatr Danub 26(S1): 256- 265.
-
Pachima YI, Nof MM, Gozes I (2019) NAP (Davunetide) Preferential Interaction with Dynamic 3-Repeat Tau Selected Tauopathies. Explains Differential Protection in PLoS One 14(3): e0213666.
-
Shiryaev N, Jouroukhin Y, Giladi E, Polyzoidou E, Grigoriadis NC, et al. (2009) NAP protects memory, increases soluble tau and reduces tau hyperphosphorylation in a tauopathy model. Neurobiol Dis 34(2): 381-388.
-
Baddeley TC, McCaffrey J, Storey JMD, Cheung JKS, Melis V, et al. (2015) Complex Disposition of Methylthioninium Redox Forms Determines Efficacy in Tau Aggregation Inhibitor Therapy for Alzheimer’s Disease. J Pharmacol Exp Ther 352(1): 110-118.
-
Lovestone S, Boada M, Dubois B, Hüll M, Rinne JO, et al. (2015) A Phase II Trial of Tideglusib in Alzheimer’s Disease. J Alzheimers Dis 45(1): 75-88.
-
Martinez A, Gil C, Perez DI (2011) Glycogen Synthase Kinase 3 Inhibitors in the next Horizon for Alzheimer’s Disease Treatment. Int J Alzheimers Dis 2011: 280502.
-
Devanand DP, Strickler JG, Huey ED, Crocco E, Forester BP, et al. (2018) Lithium Treatment for Agitation in Alzheimer’s Disease (Lit-AD): Clinical Rationale and Study Design. Contemp Clin Trials 71: 33-39.
-
Randels PM, Marco LA, Hanspal NS, Robinson (1984) Possible lithium-induced extrapyramidal effects in Alzheimer’s disease. Hillside J Clin Psychiatry 6(1): 117- 121
-
Devanand DP, Mintzer J, Schultz SK, Andrews HF, Sultzer DL, et al. (2012) Relapse risk after discontinuation of risperidone in Alzheimer’s disease. N Engl J Med 367(16): 1497-1507.
-
Porsteinsson AP, Drye LT, Pollock BG, Devanand DP, Frangakis C, et al. (2014) Effect of citalopram on agitation in Alzheimer disease: the CitAD randomized clinical trial. JAMA 311(7): 682-691.
-
Armstrong RA (2009) The molecular biology of senile plaques and neurofibrillary tangles in Alzheimer’s disease. Folia Neuropathologica 47(4): 289-299.
-
Hers I, Tavare JM, Denton RM (1999) The protein kinase C inhibitors bisindolylmaleimide I (GF 109203x) and IX (Ro31-8220) are potent inhibitors of glycogen synthase kinase-3 activity. FEBS Letters 460(3): 433-436.
-
Andrews M, Tousi B, Sabbagh MN (2018) 5HT6 Antagonists in the Treatment of Alzheimer’s Dementia: Current Progress. Neurol Ther 7(1): 51-58.
-
Edwards MM, Hind AJZ, Hunter M, Gold G, Hopton G,et al. (2010) Double-blind, controlled phase II study of a 5-HT6 receptor antagonist, SB-742457, in Alzheimers disease. Curr Alzheimer Res 7(5): 374-385.
-
Dong W, Li XJ, Chen PZ, Meng XJ (1996) Effects of N-3 Polyunsaturated Fatty Acids on Traumatic Infection. Chinese Pharmacol Bull 12(5): 461-464.
-
Lopez LB, Silverstein DK, Connor EB, et al. (2011) High dietary and plasma levels of the omega-3 fatty acid docosahexaenoic acid are associated with decreased dementia risk: the Rancho Bernardo study. J Nutr Health Aging 15(1): 25-31.
-
Yamagishi K, Ikeda A, Chei CL, Noda H, Umesawa M, Cui R, et al. (2017) Serum α-Linolenic and Other ω-3 Fatty Acids, and Risk of Disabling Dementia: Community- Based Nested Case–Control Study. Clin Nutr 36(3): 793- 797.
-
Yang X, Sheng W, Sun GY, Lee JC (2011) Effects of fatty acid unsaturation numbers on membrane fluidity and alphasecretase- dependent amyloid precursor protein processing. Neurochem Int 58(3): 321-329.
-
Hjorth E, Zhu M, Toro VC, Vedin I, Palmblad J, et al. (2013) Omega-3 fatty acids enhance phagocytosis of Alzheimer’s disease-related amyloidbeta42 by human microglia and decrease inflammatory markers. J Alzheimers Dis 35(4): 697-713.
-
Schwam EM, Nicholas T, Chew R, Billing CB, Davidson W, et al. (2014) A multicenter, double-blind, placebo- controlled trial of the PDE9A inhibitor, PF-04447943, in Alzheimer’s disease. Curr Alzheimer Res 11(5): 413-421.
-
Wilens TE, Verlinden MH, Adler LA, Wozniak PJ, West SA (2006) ABT-089 A Neuronal Nicotinic Receptor Partial Agonist, for the Treatment of Attention-Deficit/ Hyperactivity Disorder in Adults: Results of a Pilot Study. Biol Psychiatry 59(11): 1065-1070.
-
Haig GM, Pritchett Y, Meier A, Othman AA, Hall C, et al. (2014) A Randomized Study of H3 Antagonist ABT-288 in Mild-to-Moderate Alzheimer’s Dementia. J Alzheimers Dis 42(3): 959-971.
-
Vellas B, Sol O, Snyder PJ, Ousset P, Haddad, et al. (2011) EHT0202 in Alzheimer ’ s Disease : A 3-Month , Randomized , Placebo- Controlled , Double-Blind Study. Curr Alzheimer Res 8(2): 203-212.
-
Ito KN, Fujikawa Y, Hihara T, Shinjo H, Kotani S, et al. (2014) E2012-Induced Cataract and Its Predictive Biomarkers. Toxicol Sci 137(1): 249-258.
-
Henley DB, May PC, Dean RA, Siemers ER (2009) Development of semagacestat (LY450139), a functional gamma-secretase inhibitor, for the treatment of Alzheimer’s disease. Expert Opin Pharmacother 10(10): 1657-1664
-
Nishioka H, Tooi N, Isobe T, Nakatsuji N, Aiba K (2016) BMS-708163 and Nilotinib Restore Synaptic Dysfunction in Human Embryonic Stem Cell-Derived Alzheimer’s Disease Models. Sci Rep 6: 33427.
-
New Alzheimer’s Drug Clears Milestone inHuman Clinical Trial.
-
Egan MF, Kost J, Tariot PN, Aisen PS, Cummings JL, et al. (2018) Randomized trial of verubecestat for mild- to-moderate Alzheimer’s disease. N Engl J Med 378(18): 1691-1703.
-
Timmers M, Streffer JR, Russu A, Tominaga Y, Shimizu H, et al. (2018) Pharmacodynamics of Atabecestat (JNJ- 54861911), an Oral BACE1 Inhibitor in Patients with Early Alzheimer’s Disease: Randomized, Double-Blind, Placebo-Controlled Study. Alzheimer’s Res Ther 10(1):
-
Etcheberrigaray R, Tan M, Dewachter I, Kuipéri C, Wera S, et al. (2004) Therapeutic eff ects of PKC activators in Alzheimer’s disease transgenic mice. Proc Natl Acad Sci USA 101(30): 11141-11146.
-
Haig GM, Pritchett Y, Meier A, Othman AA, Hall C, et al. (2014) A Randomized Study of H3 Antagonist ABT-288 in Mild-to-Moderate Alzheimer’s Dementia. J Alzheimer’s Dis 42(3): 959-971.
-
Wang CY, Wang PN, Chiu MJ, Finstad CL, Lin F, et al. (2017) UB-311, a Novel UBITh® Amyloid β Peptide Vaccine for Mild Alzheimer’s Disease. Alzheimer’s Dement (NY) 3(2): 262-272.
-
Moschetti V, Kim M, Sand M, Wunderlich G, Andersen G, et al. (2018) The Safety, Tolerability and Pharmacokinetics of BI 409306, a Novel and Potent PDE9 Inhibitor: Overview of Three Phase I Randomised Trials in Healthy Volunteers. Eur Neuropsychopharmacol 28(5): 643-655.
-
Faux NG, Ritchie CW, Gunn A, Rembach A, Tsatsanis A, et al. (2010) PBT2 Rapidly Improves Cognition in Alzheimer’s Disease: Additional Phase II Analyses. J Alzheimer’s Dis 20(2): 509-516.
-
Pitt J, Thorner M, Brautigan D, Larner J, Klein WL (2013) Protection against the Synaptic Targeting and Toxicity of Alzheimer’s-Associated Aβ Oligomers by Insulin Mimetic Chiro-Inositols. FASEB J 27(1): 199-207.
-
Ho RC, Cheung MW, Fu E, Win HH, Zaw MH, et al. (2011) Is high homocysteine level a risk factor for cognitive decline in elderly? A systematic review, metaanalysis, and meta-regression. Am J Geriatr Psychiatry 19(7): 607-617.
-
Green KN, Steffan JS, Coria HM, Sun X, Schreiber SS, et al. (2008) Nicotinamide restores cognition in Alzheimer’s disease transgenic mice via a mechanism involving sirtuin inhibition and selective reduction of Thr231-phosphotau. J Neurosci 28(45): 11500-11510.
-
Kook SY, Hong HS, Moon M, Ha CM, Chang S, et al. (2012) Aβ 1-42-Rage Interaction Disrupts Tight Junctions of the Blood-Brain Barrier via Ca 2+-Calcineurin Signaling. J Neurosci 32(26): 8845-8854.
-
Prickaerts J, Goethem NPV, Chesworth R, Shapiro G, Boess FG, et al. (2012) EVP-6124, a Novel and Selective Α7 Nicotinic Acetylcholine Receptor Partial Agonist, Improves Memory Performance by Potentiating the Acetylcholine Response of Α7 Nicotinic Acetylcholine Receptors. Neuropharmacology 62(2): 1099-1110.
-
Tang JJN (2009) Beta-secretase as target for amyloid- reduction therapy. Alzheimers Dement 5(4): 74.
-
Froestl W, Gallagher M, Jenkins H, Madrid A, Melcher T, et al. (2004) SGS742: The First GABAB Receptor Antagonist in Clinical Trials. Biochem Pharmacol 68(8): 1479-1487.
-
Johnson DE, Drummond E, Grimwood S, Basak AS, Miller E, et al. (2012) The 5-Hydroxytryptamine 4 Receptor Agonists Prucalopride and PRX-03140 Increase Acetylcholine and Histamine Levels in the Rat Prefrontal Cortex and the Power of Stimulated Hippocampal θ Oscillations. J Pharmacol Exp Ther 341(3): 681-691.
-
Shen F, Smith JAM, Chang R, Bourdet DL, Tsuruda PR, et al. (2011) Neuropharmacology 5-HT 4 Receptor Agonist Mediated Enhancement of Cognitive Function in Vivo and Amyloid Precursor Protein Processing in Vitro : A Pharmacodynamic and Pharmacokinetic Assessment. Neuropharmacology 61(1-2): 69-79.
-
Cummings JL, Tong G, Ballard C (2019) Treatment Combinations for Alzheimer’s Disease: Current and Future Pharmacotherapy Options. J Alzheimer’s Dis 67(3): 779-794.
-
Pitt J, Thorner M, Brautigan D, Larner J, Klein WL (2013) Protection against the Synaptic Targeting and Toxicity of Alzheimer’s-Associated Aβ Oligomers by Insulin Mimetic Chiro-Inositols. FASEB J 27(1): 199-207.
-
Muhs A, Hickman DT, Pihlgren M, Chuard N, Giriens V, et al. (2007) Liposomal vaccines with conformation- specifi c amyloid peptide antigens defi ne immune response and efficacy in APP transgenic mice. Proc Natl Acad Sci USA 104(23): 9810-9815.
-
Adolfsson O, Pihlgren M, Toni N, Varisco Y, Buccarello AL, et al. (2012) An effector-reduced anti-β-amyloid (Aβ) antibody with unique aβ binding properties promotes neuroprotection and glial engulfment of Aβ. J Neurosci 32(28): 9677-9689.
-
Garber K (2012) Genentech’s Alzheimer’s antibody trial to study disease prevention. Nat Biotechnol 30(8): 731-732.
-
Callaway E (2012) Alzheimer’s drugs take a new tack. Nature 489(7414): 13-14.
-
Moreth J, Mavoungou C, Schindowski K (2013) Passive anti-amyloid immunotherapy in Alzheimer’s disease: what are the most promising targets?. Immun Ageing 10(1): 18
-
A Clinical Study to Assess Single and Repeat Doses of a New Medication (GSK933776) in Patients With Alzheimer’s Disease.
-
Ferrero J, Williams L, Stella H, Leitermann K, Mikulskis A, et al. (2016) First-in-Human, Double-Blind, Placebo-Controlled, Single-Dose Escalation Study of Aducanumab (BIIB037) in Mild-to-Moderate Alzheimer’s Disease. Alzheimer’s Dement (NY) 2(3): 169-176.
-
Sevigny J, Chiao P, Williams L, Chen T, Ling Y, et al. (2015) Aducanumab (BIIB037), an anti-amyloid beta monoclonal antibody, in patients with prodromal or mild Alzheimer’s disease: Interim results of a randomized, double-blind, placebo-controlled, Phase 1b study. Alzheimers Dement 11(7): 277.
-
van Dyck CH (2018) Anti-Amyloid-β Monoclonal Antibodies for Alzheimer’s Disease: Pitfalls and Promise. Biol Psychiatry 83(4): 311-319.
-
Sevigny J, Chiao P, Bussiere T, Weinreb PH, Williams L, et al. (2016) The antibody aducanumab reduces Abeta plaques in Alzheimer’s disease. Nature 537(7618): 50- 56.
-
Dodel RC, Du Y, Depboylu C, Hampel H, Frölich L, et al. (2004) Intravenous immunoglobulins containing antibodies against beta-amyloid for the treatment of Alzheimer’s disease. J Neurol Neurosurg Psychiatry 75(10): 1472-1474
-
Relkin NR, Szabo P, Adamiak B, Monthe C, Lent RW, et al. (2009) 18-Month study of intravenous immunoglobulin for treatment of mild Alzheimer’s disease. Neurobiol Aging 30(11): 1728-1736.
-
Gottfries MXC, Regland B, Lehmann W, Abedini I, Jonsson M, et al. (2001) Treatment of Alzheimer ’s Disease with Clioquinol. Dement Geriatr Cogn Disord 12(6): 408-414.
-
Jenagaratnam L, McShane R (2006) Clioquinol for the treatment of Alzheimer’s Disease. Cochrane database of systematic reviews (1): CD005380.
-
Gallant M, Aspiotis R, Day S, Dias R, Dubé D, et al. (2010) Discovery of MK-0952, a Selective PDE4 Inhibitor for the Treatment of Long-Term Memory Loss and Mild Cognitive Impairment. Bioorganic Med Chem Lett 20(22): 6387-6393.
-
Schechter L E, Smith DL, Lipson SR, Sukoff SJ, Dawson LA, et al. (2005) Lecozotan (SRA-333): A Selective Serotonin 1A Receptor Antagonist That Enhances the Stimulated Release of Glutamate and Acetylcholine in the Hippocampus and Possesses Cognitive-Enhancing Properties. J Pharmacol Exp Ther 314(3): 1274-1289.
- Spectrophotometric Determination of Lanthanum (III) and Some Rare Earths with Xylenol Orange
- Introduction and Sources of Molluscicides
- Trimetazidine: An Antianginal Drug and Not Only!
- Nature Inspired Discovery and Development of Antibacterials: An Update
- Fungal Biodegradation of Polycyclic Aromatic Hydrocarbons (PAHs)
- Recent Approaches of Impurity Profiling in Pharmaceutical Analysis: A Concise Review