The Role of the Cell Saber in the Intraoperative Period in Response to Bleeding During the Postoperative Period
<p style="text-align: justify;">Purpose: The risk of bleeding in Cardiac surgery is high, thus, it is necessary to transfuse blood products in the majority of cases. The Cell Saver (CS), when used during the intraoperative is an alternative helping reduce the need for homologous transfusion of blood products in cardiac surgery under extracorporeal circulation (EC). Our objective is to investigate whether the use of the CS in the intraoperative period, increases or decreases the rate of hemorrhages during the postoperative period.</p> <p style="text-align: justify;">Methods: We studied 162 patients who underwent cardiac surgery with EC and CS at the University Hospital. Analyzing variables of the CS in the intraoperative period, and postoperative bleeding are also reviewed.</p> <p style="text-align: justify;">Results: 71.6 % of the patients had no episodes of bleeding, while 28.4% had. Profile of the patients: 59.3 % males and 40.7 % women, with a mean age of 61.99 years. Surgical procedures: replacement / repair of the aortic valve (37.7 %), mitral valve (15.4 %, tricuspid valve 2.5 and more than two surgical procedures in the same patient (27.1 %). The CS, average volume of autologous blood recovered and processed was 1800 ml. being 580 ml. of red blood cells, the average volume obtained and reinfused again in the patient.</p> <p style="text-align: justify;">Conclusion: More than half of the patients who underwent cardiac surgery with EC, and the use of CS had no episodes of bleeding in the immediate postoperative period. The profile of patients treated were mainly overweight men of advanced ages undergoing surgery for aortic valve surgery.</p>
Introduction
Cardiac surgery is a complex surgical intervention that consumes a large number of blood products. Also, according to the American College of Cardiology and American Heart Association (ACC/AHA) these surgeries have a high percentage of complications or adverse reactions in the postoperative period, primarily hemorrhage [1]. Defining hemorrhage is difficult, especially when it comes to assessing criteria for blood transfusions [2].
Nursing & Healthcare International Journal
Hemorrhagic shock due to bleeding is considered as the loss of 20% or more of the circulating blood volume [3], although the study by Advance Trauma Life Support (ATLS®) considered it as the acute loss of circulating blood volume with clinical symptoms [4]. But regardless of the definition used, clinical trials it won’t be necessary the Higher Yield of the New Strategy of Enoxaparin, Revascularization and Glycoprotein IIb/IIIa inhibitors (SYNERGY), determined the risk of hemorrhage is present in patients undergoing cardiac surgery [5]. Piednoir points to two causes: unsatisfactory surgical technique or secondary to hemostasis alterations [6]. During EC, hemostatic alterations occur, requiring a normovolemic hemodilution, which triggers a decrease in hemoglobin and hematocrit of the patient. On the other hand, the administration of high doses of heparin sodium to prevent blood clotting on the surface of the extracorporeal circuit. Furthermore, sodium heparin used in high doses to prevent blood clotting in the extracorporeal circuit surface can aggravate the homeostatic alterations and cause haemorrhage [7, 8] moreover, the protamine, can produce blood clotting disorders. Other elements that also influence the risk of bleeding and need to be taken into account are: advanced age, anemia, coagulation disorders, thrombocytopenia or antiplatelet therapies. In the case of hemorrhage of patients undergoing cardiac surgery with EC, the transfusion is a total or partial recovery of the blood, so it is necessary to assess their benefits [9]. Homologous blood transfusions can be packed erythrocytes or red blood cells, platelets and coagulation factors. Homologous blood transfusions have complications, ranging from the reaction to their components, up to the possibility of transmitting diseases [10]. There are authors [11, 12, 13, 14], that relate the transfusion with postoperative complications, and long- term morbidity. Numerous reports and cohort studies have related homologous blood transfusions with nosocomial infections, such as viral hepatitis C, T-virus, and herpes virus, human VIII Kaposi's sarcoma and HIV [15]. Despite of the extreme care and monitoring during the processes of donation and transfusion, these complications, although rare, are potentially serious [13], and although they have low incidence in developed countries, they represent an important problem in less developed ones. Ferraris [16], said that there is a widespread fear in society with regard to transfusions, having knowledge of the short- and long-term impacts, and that there are no laboratory tests to detect all the infectious agents, and the existing ones are not 100% effective. In this sense, despite the attempts of standardization through publication of various guides, manuals, and protocols of transfusion [17], each institution has its own health transfusion criteria. The recent study Transfusion requirements after cardiac surgery (TRACS), showed that the characteristics of the cardiovascular patient have to be taken into account. On the other hand, the scarcity of donations of blood products, resulting in insufficient reserves in blood banks, increases the need to develop procedures for the conservation of blood of the patient [18]. This need for blood transfusions [1], in cardiac surgery and its relationship with postoperative complications, and long-term morbidity, highlights the advisability of launching alternatives to reduce the need for transfusion of homologous blood products [19]. It is therefore interesting to investigate techniques such as the CS, which can be an alternative to reduce the need for transfusion of blood products in cardiac surgery [20, 21]. The CS is used as a fundamental strategy for saving of homologous blood, needed by patients after cardiac surgery, as declared by the autologous transfusion study Committee (AABB) [22], and many other studies that indicate that their use is safe, effective and efficient for the reduction of homologous blood transfusion [5, 6, 7, 8, 9]. In addition, the study by Booke [23], claim that the use of the CS in the surgical context, decreases by more than 90% the need for transfusion with blood products and poses a lesser risk for the cardiovascular patient and represents a lesser cost to the hospital [18, 19, 20, 21].
Methods
This research is observational and cross sectional and was carried out from January to October 2014our hospital. Patients scheduled by the cardiovascular service for cardiovascular surgery interventions under EC, and interventions where CS was going to be used as an alternative to homologous blood transfusion. The inclusion criteria were patients with age greater than or equal to 18 years to be accepted on a voluntary basis to participate in the study after having been verbally informed of the characteristics of the same and had signed the informed consent. Exclusion criteria: patients with clotting disorders, kidney failure, impaired liver function, with malignancies, HIV seropositive, hepatitis B - C, septic pathology. Patients with clotting disorders prior to surgery, with bleeding twelve hours before the scheduled surgery or reoperated on an emergency basis, Nursing & Healthcare International Journal
because they would be strong candidates to be transfused and could alter the collected data. Patients who did not accept their participation. We selected all the cardiovascular patients that were scheduled for cardiac surgery under EC, with use of the CS from January to October 2014, a total of 162 patients, data provided by Application for the management of the Demand.
Ethical Considerations
The project was developed at any time by following the ethical principles embodied in the Declaration of Helsinki, declaration on principle for the ethical medical research in human beings made in Helsinki (1964), and subsequently revised in Tokyo (1975), Venice (1983), Hong Kong (1989), Somerset West (1996), Edinburgh (2000), Washington (2002), Seoul (2008), including the application of informed consent to all the patients that were included [14]. All the records and the corresponding informed consent from each patient are properly file protected, still identified only by the number assigned, this complies with the Spanish laws on data protection (Organic Law 15/1999 of December 13th). This project has obtained the approval of the Commission on Ethics and Clinical Research our hospital, with approval number 2009.
Measurements / Instruments
For the surgical procedure conventionally patient under general anesthesia, using the appropriate protocol for patien weight heparin at the start of the intervention, being used also at the end of cardiopulmonary bypass, protamine protocol which was suitable to the initial dose of heparin. And I prepared radial arterial line, central three-way catheter through the subclavian vein and bladder catheter was placed. The approach was performed through a longitudinal sternotomy and protocol of anticoagulation with heparin and cannulation for cardiopulmonary bypass, was similar in all patients. cardioplegic arrest was induced and the scheduled procedure was performed. To keep clean surgical field aspirators connected to cardiopulmonary bypass during the time that lasted this derivation were used. After the cardiopulmonary bypass, the heparin effect was reversed, hemostasis was performed and the chest wall was closed leaving drainage tubes connected to a suction system seal 20 cm H20.
For cell recovery they were used suction through a double-lumen tube which allowed the volume sucked contact with a saline solution 1000cc, combined with 25,000 units of heparin. Washing in centrifugal hood, 3000 cc of saline was used at a speed of 2,000 revolutions per minute in order to keep only the red cells which was reinfused back into the patient intravenously.
Data Collection / Procedure
A collection data sheet was designed for compilation of the information. The variables of the study were collected in a standardized format being collected variables in the preoperative period were: hemoglobin - expressed in gr/dl-, hematocrit - expressed in % -, total protein - expressed in gr/dl-, platelets expressed in 103mm-, prothrombin time (PT) - expressed in seconds-, activated partial thromboplastin time (APTT) - expressed in seconds-, activated clotting time (ACT) - expressed in seconds-, international normalized ratio (INR) - expressed in seconds -. The profile of patiens (age, sex, height, weight, body mass index (BMI), body surface index (BSA), medical diagnosis (reason for hospital admission) and surgical treatment. The variables that were collected in the intraoperative period (after completion of cardiopulmonary bypass) were: Cell saver (CS), (volume of autologous blood recovered and processed, volume of red blood cells obtained and reinfunsed, these variables were expressed in milliliters, and evaluated according to the data obtained from the CS. Washing program (washing of high quality, high-quality, fast, super fast, and emergency washing). Revolutions per minute of processing (rpm). Processing time, expressed in minutes and problems using the CS, evaluated with dichotomous responses (yes or no). These variables were obtained from data provided by the CS on its digital display. The variables that were collected in the postoperative period(12 hours after surgery practiced)were: hemoglobin - expressed in gr/dl-, hematocrit - expressed in % -, total protein - expressed in gr/dl-, platelets expressed in 103mm-, prothrombin time (PT) - expressed in seconds-, activated partial thromboplastin time (APTT) - expressed in seconds-, activated clotting time (ACT) - expressed in seconds-, international normalized ratio (INR) - expressed in seconds – and haemorrhage. – expresed in units-.
Data Analysis Used
For the descriptive study, numeric variables they
Nursing & Healthcare International Journal
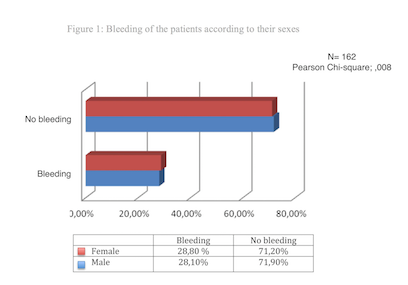
expressed as mean, standard deviation and the nominal variables on average. For the quantitative variables, the mean mean and standard deviation were used. The Pearson Chi-square test and Fisher's exact test were used through the elaboration of cross tables 2x2 as appropriate. The statistical significance level was set at a p value of < 0.05 (Figure 1). Statistical analysis was conducted using the statistical package SPSS version 22.0 for Windows.
Results
Of the 478 (100 %) patients scheduled by the cardiovascular surgery service, 162 were included (33.8 % ), 316 (66.2 %) patients were excluded in whom: 254 (53.2 %) the CS was not used in the absence considerable blood loss, 1 (0.2 %) had bleeding twelve hours before the scheduled surgery; 8 (1.6 %) had blood clotting disorders prior to the surgery; 5 (1 %) were infected with hepatitis B; 2 (0.5 %) were hepatitis C virus carriers; 2 (0.5 %) had neoplasms; 2 (0.5 %) were infected with the HIV virus; 34 (7.1 %) had to be reoperated on an emergency basis and 8 (1.6 %) did not sign the informed consent. We analyzed the data of 162 patients, 96 males (59.3 %) and 66 females (40.7 %), with a mean age of 61.99 years. Cardiovascular diagnoses we encountered were: aortic valvular disease (37.7 %) more than two cardiovascular pathologies (28.3 %) coronary arteriosclerosis (17.3 %), mitral valve disease (14.2 %) and tricuspid valve disease (2.5 %).Cardiovascular procedures we encountered were: replacement / repair of the aortic valve (37.7 %) more than two surgical procedures in the same patient (27.1 %), of replacement / repair of the mitral valve (15.4 %), coronary bypass (17.3 %) and replacement / repair of the tricuspid valve (2.5 %). The CS: the average volume of autologous blood recovered and processed was 1800 ml, being 580 ml of red blood cells, the average volume obtained and reinfused again in the patient.
Preoperative Period
Hb 12.9 g/dl, standard deviation 2, 04. Hc 38.5 %, standard deviation 6, 1 6. Total protein 7.6 gr/dl, standard deviation 8, 27. Platelets 214.3 103mm, standard deviation 80,6. PT 13.8 seconds, standard deviation 5, 58. PTTa 38.2 seconds, standard deviation 17,2. ACT 118 seconds, standard deviation 18,97. INR 1.22 seconds, standard deviation, 41.
Intraoperative Period
The CS in 100% (N=162) of the cases, worked with: high quality heading of washing, at a processing speed of 2000 rpm, there were no problems using the CS, the average time for processing autologous blood recovered was 20.02 minutes, with a minimum of 10 minutes, maximum of 51 minutes and a standard deviation of 5.84. A mean of 1800 ml of autologous blood was recovered and processed with a mean volume of 580 ml of red blood cells obtained and reinfused.
Postoperative period
Hb 11.9 g/dl, standard deviation 1,75. Hc 32.9 %, standard deviation 5,32. Total proteins 5.2 gr/dl, standard deviation, 81. Platelets 164.3 103mm, standard deviation 72,68. TP 14.6 seconds, standard deviation 5,42. PTTa 35.6 seconds, standard deviation 9,16. ACT 103.7 seconds, standard deviation 17,24. INR 1.28 seconds, standard deviation, 48. 71.6 % (N=116) of the patients had no episodes of bleeding, 28.4 % (N=46) had bleeding: Standard Deviation of 0,45. In response to the hemorrhage by genus there are no significant statistical differences (n=162, Chi-square test; 0,008). See figure nº. 1
Discussion
With respect to the profile of the patients studied in regard to gender, our results are consistent with the statistics provided in the European forum of cardiovascular disease (ECVD) [24], affect slightly more men than women, in his study 59.3 % males and 40.7 %
Nursing & Healthcare International Journal
women. According to the National Statistics Institute (INE) [25], this is relative, because in the next decade, the percentages will match in both sexes, CVD being more frequent in advanced ages, where the number of women with CVD is higher than the number of men. In regards to age, the study SYNTAX [17], reports that it is a factor to take into account in patients after heart surgery, being its greatest prevalence at 75 years, in both sexes. Our patients had an average of 62 years. This shows that there is a tendency of younger patients to undergo cardiac surgery compared with the American studies. Despite the fact that all the patients studied arrived at the operating room with analytical values within the normal range, due to blood loss, there is a lowering of the hemoglobin, hematocrit, total proteins and platelets that remain low during the postoperative period. However, with the re-infusion of red blood cells from the CS, these values increase. The use of the CS did not cause problems in the recovery of autologous blood. We agree with the studies of Manjuladevi [26] and others [27], and who claim that the use of the CS is an effective and safe measure to save intraoperative blood. According to the Spanish Society of Thoracic and Cardiovascular Surgery (SECTCV) [28], the CS is effective in cardiac surgery scenarios, although difficult to assess, because the decision to use the CS is based mainly on the availability and preference of the nurse perfusionist. Despite the difficulties mentioned, the use of CS in the patient’s operated heart, reduces the bleeding rates (according to our results, 28%), compared to those in which it is not used, increasing the possibility of bleeding by 60% [29]. We can assume, that from limited data and in an attempt to avoid the homologous blood transfusion in cardiac surgery under EC, the use of new technologies such as CS, need solid evidence to support its use [3, 4, 13, 18]. Despite the fact that in Spain, the CS has been introduced as an alternative to homologous blood transfusions, any intervention that is part of a strategy for blood presservation, needs a critical analysis in regards to cost-effectiveness. To provide scientific evidence for use of the CS, more comparative tests are necessary to evaluate the relative efficacy, security, and cost effectiveness of the CS in different surgical procedures. Our study is a starting point. The American Heart Association and the American College of Cardiology (AHA/ACC) [1] points out that it is reasonable to carry out any study demonstrating satisfactory reduction of hemorrhage in cardiac surgery, as it provides scientific evidence to programs aimed at the conservation of blood.
Conclusions
Patients who underwent surgery with EC and using the CS 30% of patients had no episodes of bleeding in the immediate postoperative period, compared to other studies that claim that 60% of patients were suffering bleeding if not using the CS. And the profile of patients treated were mainly men of advanced age and overweight, with medical diagnosis of aortic valvular disease which underwent surgery for aortic valve surgery, with analytical values within the normal parameters in the preoperative period, which fell below intraoperatively and remained in that range in the postoperative period.
References
-
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, et al. (2014) AHA/ACC Guideline for the management of patient with valvular heart disease. J Am Coll Cardiol 63(22).
-
Shander S (2012) Strategies to reduce the use of blood products: US perspective. Cur Opin Anesth 25: 50.
-
Gomar C, Pomar JL, 2nd (Edn.) (Barcelona): Ergon (2013) Pathophysiology and cardiopulmonary bypass techniques. Spanish Perfusionists Association(AEP) 125-129
-
Leal Noval SR, Munoz M, Asuero M, Contreras E, Garcia Erce JA, et al. (2013) Spanish Consensus Statement on alternatives to allogeneic blood transfusion: the 2013 update of the "Seville Document". Blood Transfus 11(4): 585-610.
-
Sunil V (2010) Bleeding in patients with acute coronary syndromes: a disturbing finding a major challenge. J Am Coll Cardiol 63(01): 1-4.
-
Piednoir P, Allou N, Provencheres, Berroeta C, Huisse MG, et al. (2012) Heparin-induced thrombocytopenia after cardiac surgery: an observational study of 1,722 patients. J Cardiothorac Vasc Anesth 26(4): 585-590.
-
Williams JB, DeLong ER, Peterson ED, Dokholyan RS, Ou FS et al. (2011) Secondary prevention after coronary artery bypass graft surgery: Findings of a national randomized controlled trial and sustained society-led incorporation into practice. Circulation 123: 39-45. Nursing & Healthcare International Journal
-
Naranjo A, SelmanHousein E, Marcano LE, et al. (2013) Twenty Three years of surgical treatment adult with congenital heart disease in the Cardiology William Soler 19(1).
-
Vergara JC (2012) Postoperative bleeding in cardiac surgery 1-107.
-
García E (2013) Guidelines transfusion in surgical patients. J Anesth Resus 12(3).
-
Ferraris VA, Brown JR, Despotis GJ, Hammon JW, Reece TB, et al. (2011) Update to The Society of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologist Blood Conservation Clinical Practice Guideline Ann Thorac Surg 91(3): 944-982.
-
Perez Valdivieso JR, Monedero P, García Fernández N et al. (2013) Intraoperative transfusion in cardiac surgery. Retrospective nested ase-control. J Anesth Resus 60(2): 79-86.
-
Lelubre C, Vicent JL (2013) Relationship between red cell storage duration and outcomes in adults receiving red cell transfusions: a systematic review. Critical Care 17(2): R66.
-
Nicolaides A (2016) Bioethical considerations, the Common Good Approach and some shortfalls of the Belmont Report. Medical Technology 30(1): 15-23.
-
Weightman WM, Gibbs NM (2012) Management of coagulation: an Australian perspective. Curr Opin Anaesthesiol 25(1): 86-95.
-
Ferraris VA, Suellen P, Saha S, Hessel EA, Haan CK et al. (2007) Perioperative Blood Transfusion an Blood Conservation in Cardiac Surgery: The Society of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologists Clinical Practice Guideline. Ann Thorac Surg 83: S27-86.
-
Morice MC, Serruys PW, Kappetein AP, Ferldman TE, Ståhle E, et al. (2014) Five –year outcomes in patients with left main disease treated with either percutaneous coronary intervention or coronary artery bypass grafting in the SYNTAX trial. Circulation 129(23): 2388-2394.
-
Taggart DP (2013) CABG or stents in coronary artery disease: end of the debate? Lancet 381(9867): 605- 607.
-
Nallas BP, Freedman J, Hare G, Mazer D (2012) Update on blood conservation for cardiac surgery. J Cardioth Vasc Anesth 26(1): 117-133.
-
Sniecinski RM, Levy JH (2011) Bleeding and management of coagulopathy. J Thorac Cardiovasc Surg 142(3): 662-667.
-
Igual A, Mestres CA (2013) Cardiovascular surgery in Spain in the years 2009-2010 by the Spanish Society of Cardiovascular Surgery Torácica- (SECTCV). Cardiovasc Surg 20: 74-88.
-
AABB (1997) Guidelines for blood recovery and reinfusion in surgery and trauma. Bethesda: American Association of Blood Banks, Autologous Transfusion Committee.
-
Booke M, Van Aken H, Storm M et al. (1997) Fat removal during intraoperative auto transfusion in vitro research. Analgesic Anesth 85(5): 959-962.
-
Broughton A (2010) Europa: Work related stress. Eur Work.
-
Statistics National Institute (2010) Hospital Morbidity Survey pp: 10.
-
Manjuladevi M, Vasudeva KS (2014) Techniques for intraoperative blood saving. Indian J Anaesth 58(5): 573-580.
-
Carless PA, Henry DA, Moxey AJ, O'Connell D, Brown T, et al. (2010) Cell salvage for reducing transfusions with donated blood.
-
Igual A, Mestres CA (2012) Cardiovascular surgery in Spain in the years 2009-2010 by the Spanish Society of Cardiovascular Surgery Torácica- (SECTCV) Cardiovasc Surg 19(3): 315-328.
-
Silveira Álvarez A, Milán Gónzalez E, Fernández García RA et al. (2011) Characterisation of reoperation for excessive bleeding in heart surgery. Rev Fed Arg Cardiol 40(4): 349-355.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City