The Effects of a Health Education Intervention Program on Infantile Colic
Background: Infantile colic (IC) is defined as uncontrollable irritability or crying in a healthy infant. It usually appears under 12-month after birth and about 10-20% infants have suffered it. The parents of infants with IC suffered from physical and mental anxiety and stressful family relationship. Objective: To examine the effects of an Infantile Colic Health Education Program (ICHEP) on parents’ knowledge, attitudes, and behavioral management with IC. Design: Two-group randomised controlled trail. Settings and Participants: A total of 156 infants from birth to 12-month of age that diagnosed with IC from a hospital in South Taiwan. Methods: The participants were randomly assigned to either attend the ICHEP (n=70) or the control group (n=70). The questionnaires included the knowledge, attitudes, behavioral management on infantile colic for parents, and the Cronbach’s α value was between 0.58 and 0.63. Pre-post-test, follow-up test and the re-tracing test were conducted. An independent t-test and the generalized estimating equation (GEE) model were used to compare the differences in the study outcomes. The statistical tests were two-sided and a p-value below 0.05 was considered statistically significant. Results: No difference was detected in the baseline characteristics between two-groups. The ICHEP group scores on knowledge, attitudes and behavioural management in the post-test were significantly higher than the pre-test. The average score of ICHEP in re-tracing test (p<0.001) was significantly higher than the scores of the pre-test (p = 0.08), the post-test (p = 0.001), and follow-up test (p = 0.32). Result was evident that the ICHEP significantly improved parent’ implementation of caring behaviour on IC and reduced the incidence of IC. Conclusions: The ICHEP can not only improve the parent’ knowledge, attitudes and management behaviour on IC but also significantly reduce the incidence of infants with IC. ICHEP can be used as a reference for healthcare workers to immediately provide to parents in the early stages of diagnosis at outpatient clinics in the future. We recommend that ICHEP can include into healthcare workers continues training courses in order to assist in understanding IC, help reduce anxiety and fear of parents, thereby enhancing a harmonious parent-child relationship.
Introduction
Infantile colic (IC) is a common disease that occurs within six weeks after birth [1, 2]. According to Wessel, et al. [3]. IC refers to healthy infants with periods of crying lasting for more than three hours a day, at least three times a week for more than three weeks within the first four months after birth, also called the “3-3-3 principle”. Recently, the definition has been expanded to include infants with irritability and crying for at least a week, and it has been included in the gastrointestinal disorders criteria [4, 5].
The cause of IC is still unknown. The gastrointestinal tract of the infant has not fully developed and is prone to issues, such as flatulence. Whenever infants have physical discomfort, their temperament, mood, sleep quality, and neuroendocrine functions can be affected if they cry for extended periods of time [6]. It might be related to certain internal and external stimulus and being unable to comfort their own emotions; as well as related to indigestion which is caused by gastro‐oesophageal reflux disease (GORD), and cow’s milk protein intolerance (CMPI) cause the infants to cry in pain and inhale a lot of air, further causing infantile colic [7, 8, 9].
Unexplained and constant crying of babies may cause stress upon the primary caregivers of the family (such as parents). Turner TL & Palamountain S [10] pointed out that caregivers of infants with IC could easily become irritable. Family caregivers may also lose their temper due to the infants’ inability to properly express physical discomfort, and the family environment could affect the physical and mental development of infants. Parental behavior has the most direct influence on the infants’ neurodevelopmental maturity, development of temperament, and the ability to adapt to the environment [10]. Because IC is a relatively unfamiliar disease to parents, approximately 14-28% of parents seek help from medical professionals for this situation, accounting for one of the main reasons why babies seek medical treatment in the first year of life [1, 11].
Treatment for IC is diversified, including supportive care (touch and hugs, comfort, and divert attention) [10, 12], diet therapy (breast milk feeding, eliminating protein and lactose, and adding probiotics) [12, 13, 14, 15], infant massage, and other methods [16, 17, 18]. Infant massage is one of the most commonly used methods for the treatment of IC. Clinical research and practice have proven that massage could stimulate both the nervous and gastrointestinal circulation of the infant, help with skin development, relieve pain, and increase soothing and relaxation of the musculoskeletal system. These effects may help reduce muscle tension, increase bone muscle stability, reduce tension and anxiety, improve quality of sleep, increase weight, reduce crying, promote defecation, etc. massage may help parents understand their infants body language expressions faster, increase mutual intimacy and trust, establish a good parent-child connection and sense of attachment, enhance the ability and confidence of parents in caring for infants, and make infants feel be loved and accepted [16]. A present study among patients using Complementary and alternative medicine (CAM) to their babies revealed improved infants comfortable and unknown crying [19]. The most common CAM method used by mothers for their babies was massage (59.0%). The most second frequent methods were determined as fennel tea (48.4%) and rhythmic rocking (48.4%). The least applied methods were amulet (3.0%), acupuncture (3.0%) and poppy oil (3.0%). A minority (4.5%) of mothers swaddled their babies. There was a statistically significant difference between the use of CAM and the education level of mothers (p < 0.05). The results showed that CAM methods can be used in IC treatment.
This study is a randomized controlled trial that examined the effects of IC Health Education Program (ICHEP) among infant diagnosed with IC in Southern Taiwan. Thus, the ICHEP will be developed and established, and the effects of implementation on infants with colic were reported in this paper.
Method
Study Participants, Setting and Design
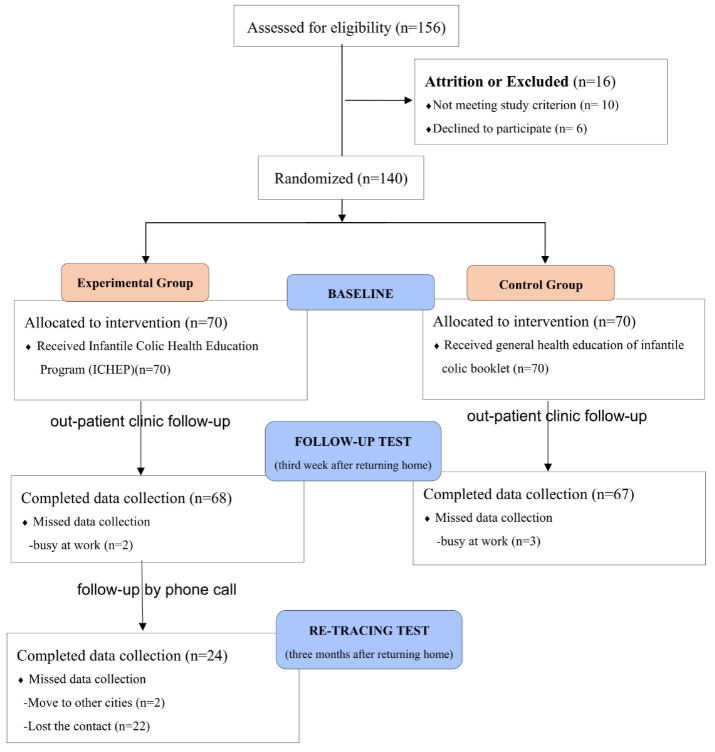
In the power analysis, to calculate the sample size of this study were considered with a significant level of 0.05 and power of 80%, the effect size was 0.452. It was similar studies obtained from Castejon-Castejon, et al. [20] which involved intervention strategies similar to those in the current study. The calculated sample size was 78. A total of 156 participants were initially approached (Figure 1). Inclusion criteria: infants within one year (inclusive) of age, with no congenital malformations, the product of a single or multiple birth, having been diagnosed with IC by a physician. Parents never dealt with IC before and willing to participate and signed the consent form for this study. The recruitment period was from March 11 to November 23, 2017 at paediatric clinic of a teaching hospital in southern Taiwan.
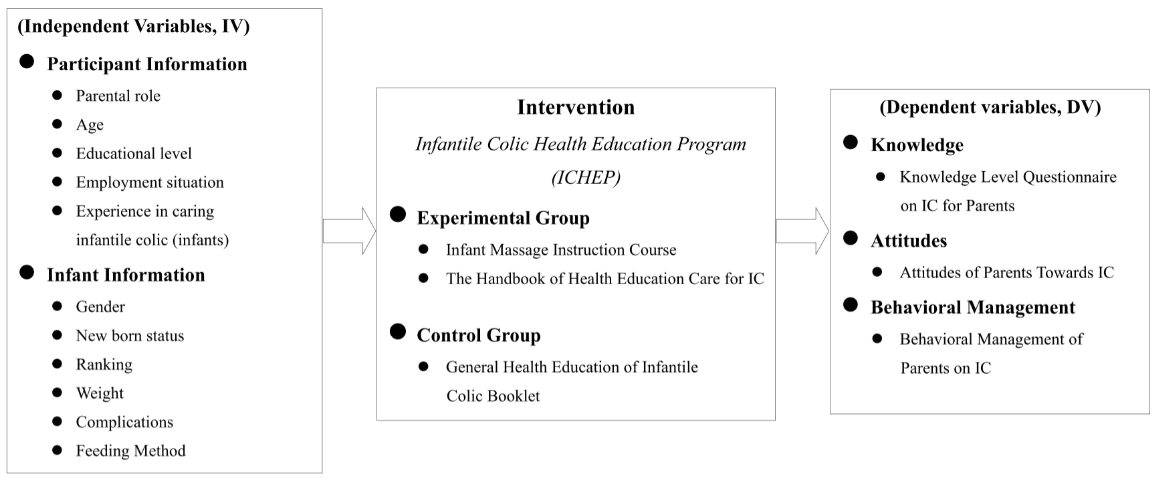
This study used IC Health Education Program (ICHEP)
as intervention program, parental and infant information as independent variables and parents’ knowledge, attitudes and behaviours management on IC as dependent variables to construct the conceptual framework of this research (Figure 2).
Intervention
The participants were randomly assigned to ICHEP or control group by opening playground area next to the pediatric clinic. In ICHEP group, each parent had one face- to-face education session (at least 30 min) including 15 minutes practical lesson on infant abdominal massage skills and 15-minute education course on how to care of IC. Also, parents or other caregivers had the opportunity for online learning at any time anywhere, a QR code of the infant massage video was placed in ICHEP. The video contained the infant abdominal massage techniques and massage songs that were provided by McClure [21] at the International Association of Infant Massage. For the control group, a general health education of IC booklet from clinical station was provided and parents were instructed orally in the infant abdominal massage technique.
The ICHEP was divided into two parts of content, including “Infant Massage Instruction Course” and “The Handbook of Health Education Care for IC”. “Infant Massage Instruction Course” was designed after researcher obtaining a training certificate as an International Infant Massage instructor in February 2016. It was divided into 13- item: (1) history and background of infant massage; (2) guidelines for course instruction; (3) bonding; (4) environment and situation; (5) posture; (6) behavioral state; (7) infant cues; (8) reflex actions during the massage; (9) parental relaxation; (10) obtaining the infants consent; (11) massage benefits; (12) teaching massage procedures (manipulations) for relieving flatulence and IC; (13) theory and discussion. During the 30 minutes course, natural and organic baby oil was provided for the massage, the skills of hugging and touching were encouraged to help relieve the infant’s abdominal discomfort, and improvement of the knowledge and skills of parents on infant abdominal massage was encouraged.
Another, “The Handbook of Health Education Care for IC” complied with “The Handbook of Children Health and Education” issued by Health Promotion Administration, Ministry of Health and Welfare [22] and referenced multiple published books [16, 23]. It was divided into nine items: (1) understanding of IC; (2) common causes of IC; (3) symptoms of IC; (4) how to treat IC; (5) what is an infant massage; (6) the benefits of an infant massage; (7) techniques for infant massage; (8) songs for abdominal massage; (9) questions and answers.
Both groups had pre-test and post-test evaluation, and the follow-up test in out-patient clinic after discharge three- week later. The participant only in ICHEP group, telephone interview was conducted three- month later to track the follow-up results.
Measures
We evaluated the effect of ICHEP by measure of knowledge, attitudes and behaviours management of parents on IC. Those questionnaires were self-developed based on previous research [24, 25, 26, 27, 28]. Five experts (two medical education experts, two paediatricians , and a chief of the medical institution) were invited to review the validity of the questionnaires. The “knowledge level questionnaire on IC for parents” has a content validity index (CVI) of 1.00, “attitudes of parents towards IC” has a CVI of 0.94, and “behavioral management of parents on IC” has a CVI of 1.00. The validity of content more than 0.85 was showed good expert validity [29].
In the questionnaire of “knowledge level questionnaire on IC for parents”, there were a total of 18 questions and scoring awarded points depending on “wrong” and “right “(0 or 1). The highest score achievable was 18 points; the higher the score, the better the knowledge. In the questionnaire of “attitudes of parents towards IC”, there were a total of 15 questions and scoring awarded points depending on a five- point Likert Scale. The highest total score was 75 points, higher scores correlated with positive attitudes of parents towards IC. In the questionnaire of “behavioral management of parents on IC”, there were a total of 8 questions and scoring awarded points depending on a five-point Likert Scale. The highest total score was 40 points, higher score correlated with a positive behavioral management of parents on dealing with IC.
The questionnaire of “basic information of parents” included: the role of the primary caregiver, age, educational level, occupation, marriage, and religious beliefs etc... “Basic information of infants” questionnaire included: gender, age, current weight, sibling ranking, prematurity, comorbidities, and feeding method.
The reliability analysis of the questionnaires showed an internal consensus reliability of the “attitudes of parents towards IC” and “behavioral management of parents on IC” questionnaires of 0.58 and 0.63, respectively. This corresponds with the accepted value of Cronbach’s α in the range of 0.50-0.70 published by Wu [30]. The “knowledge level questionnaire on IC for parents” was elaborated based on the difficulty index (P) and discrimination index (D) of Escudero, et al. [31]. The analysis of this study was above 0.3, interpreted as excellent.
Data Collection
This study was obtained from the Hospital Ethical Committee (no.16-072-A2). Questionnaires were conducted anonymously to protect the rights and interests of participants. An explanation about the purpose and methods of this study was provided to participants. The data taken during the study was coded. The results were published and presented in an anonymous form and provided for academic research only.
Statistical Analysis
All data analyses were conducted by used SPSS 22 for Windows. Results are expressed using descriptive statistics (distribution of times, percentage, mean, standard deviation), inferential statistics (chi-square test χ2, Fisher’s Exact test, t-test, pair t-test, one-way ANOVA), and Pearson product- moment correlation was used to compare categorical variables and continuous variables of the difference between the experimental group and the control group. ANCOVA was used to analyze the control interference to understand the learning effect of the ICHEP on infant abdominal massage.
Descriptive statistics were used to calculate the distribution of basic information in “parental variables” and “infant variables”. A t-test was used to explore the scores of parents in both groups and to establish if there was a difference between pre-test and post-test regarding “knowledge”, “attitudes” and “behavioral management” of IC, to understand whether there was any impact of the ICHEP. The repeated measure ANOVA was used to explore “knowledge”, “attitudes” and “behavioral management” of parents in both groups regarding IC. If the F test reached a significant level (p <.05), it meant that parents had significant differences at the four-time points (pre-test, post-test, follow-up test at three weeks, and re-track test at three months).
Afterwards the least significant difference (LSD) was used to compare results. The generalized estimating equation model was conducted to ICHEP to improve the knowledge, attitudes, and behavioral management of parents whose infants have been diagnosed with IC. This model can handle the randomly missing data mathematically and make the estimation closer to real practice [32]. Any variable that had a p < 0.1 in between-group comparisons at baseline was regarded as the covariate in the adjusted generalized estimating equation model. A two-tailed significance level was set as 0.05.
Results
Participant Demographics
A total of 140 participants were recruited at final. The majority of caregivers were mothers (136, 97.1%), between 31-35 years of age (62, 44.3%). The majority were university graduates (84, 60%) and had experience in caring for only one infant with IC (133, 95%). The average time of infant care was 2.96 hours per day, with mothers as the primary caregivers (52, 37.1%). The results show that infants were full term delivery (125, 89.3%) and most were male (74, 52.9%). The average age was 1.79 months, ranging between one month to eleven months. The average age for diagnosis was one month after birth (99, 70.17%). The most common time for IC was between 6 pm to 12 pm. The typical average crying time was 10-30 minutes. There was no significant difference in basic demographic data between the experimental group and the control group compared by chi-square test or t-test, indicating that the attributes of the demographics of both groups were homogeneous (Table 1).
| Categories | All (n = 140) | Experimental group (n = 70) | Control group (n = 70) | X 2/ t-value p-value | ||||
|---|---|---|---|---|---|---|---|---|
| Number percentage | Number percentage | Number percentage | ||||||
| Infant Gender | X2= 0.12 | 0.74 | ||||||
| Male | 74 | 52.90% | 36 | 51.40% | 38 | 54.30% | ||
| Female | 66 | 47.10% | 34 | 48.60% | 32 | 45.70% | ||
| New born status | X2 = 0.67 | 0.41 | ||||||
| Term delivery | 125 | 89.30% | 64 | 91.40% | 61 | 87.10% | ||
| Premature delivery | 15 | 10.70% | 6 | 8.60% | 9 | 12.90% | ||
| Ranking | .85a | |||||||
| First child | 80 | 57.10% | 42 | 60% | 38 | 54.30% | ||
| Second child | 55 | 39.30% | 26 | 37.10% | 29 | 41.40% | ||
| Third child | 4 | 2.90% | 2 | 2.90% | 2 | 2.90% | ||
| Fourth child | 1 | 0.70% | 0 | 0.00% | 0 | 0.00% | ||
| Weight | X2 = 0.82 | 0.94 | ||||||
| Less than 2500g | 9 | 6.40% | 5 | 7.10% | 4 | 5.70% | ||
| 2501-3000g | 35 | 25.00% | 16 | 22.90% | 19 | 27.10% | ||
| 3001-3500g | 36 | 25.70% | 18 | 25.70% | 18 | 25.00% | ||
| 3501-4000g | 21 | 15.00% | 12 | 17.10% | 9 | 12.90% | ||
| Above 4001g | 39 | 27.90% | 19 | 27.10% | 20 | 28.60% | ||
| Complications | X2 = 0.08 | 0.79 | ||||||
| N/A | 125 | 89.30% | 62 | 88.60% | 63 | 90.00% | ||
| Yes (Respiratory distress, jaundice, etc.) | 15 | 10.70% | 8 | 11.40% | 7 | 10.00% | ||
| Siblings | X2 = 1.41 | 0.23 | ||||||
| N/A | 77 | 55.% | 42 | 60.% | 35 | 50.% | ||
| Yes | 63 | 45.% | 28 | 40.% | 35 | 50.% | ||
| Feeding Method | X2 = 2.93 | 0.23 | ||||||
| Breast Milk | 58 | 41.40% | 25 | 35.70% | 33 | 47.10% | ||
| Formula | 10 | 7.10% | 7 | 10.00% | 3 | 4.30% | ||
| Mix | 72 | 51.40% | 38 | 54.30% | 34 | 48.60% | ||
| Parental role | X2= 0.00 | 1.00 | ||||||
| Father | 4 | 2.90% | 2 | 2.90% | 2 | 2.90% | ||
| Mother | 136 | 97.10% | 68 | 97.10% | 68 | 97.10% | ||
| Age | .55a | |||||||
| 20-25 years old | 9 | 6.40% | 3 | 4.30% | 6 | 8.60% | ||
| 26-30 years old | 30 | 21.40% | 15 | 21.40% | 15 | 21.40% | ||
| 31-35 years old | 62 | 44.30% | 31 | 44.30% | 31 | 44.30% | ||
| 36-40 years old | 34 | 24.30% | 18 | 25.70% | 16 | 22.90% | ||
| Above 41 years old | 5 | 3.60% | 3 | 4.30% | 2 | 2.90% | ||
| Educational level | X2 = 5.19 | 0.27 | ||||||
| Junior High School | 2 | 1.40% | 2 | 2.90% | 0 | 0.00% | ||
| High School | 12 | 8.60% | 3 | 4.30% | 9 | 12.90% | ||
| Junior college | 18 | 12.90% | 9 | 12.90% | 9 | 12.90% | ||
| University | 84 | 60.00% | 44 | 62.90% | 40 | 57.10% | ||
| Master | 24 | 17.10% | 12 | 17.10% | 12 | 17.10% | ||
| Employment situation | .70a | |||||||
| Housewife | 52 | 37.10% | 28 | 40.00% | 24 | 34.30% | ||
| Military police • Civil servant • Teacher | 19 | 13.60% | 9 | 12.80% | 10 | 14.30% | ||
| Businessman • Service | 46 | 32.80% | 21 | 30.00% | 25 | 35.80% | ||
| Healthcare | 9 | 6.40% | 7 | 10.00% | 2 | 2.90% | ||
| Worker | 7 | 5.00% | 3 | 4.30% | 4 | 5.70% | ||
| Others | 7 | 5.00% | 2 | 2.80% | 5 | 7.10% | ||
| Experience in caring infantile colic (infants) | X2 = 0.00 | 1.00a | ||||||
| 1 infant | 133 | 95.00% | 67 | 95.70% | 66 | 94.30% | ||
| 2 infants | 7 | 5.00% | 3 | 4.30% | 4 | 5.70% | ||
| Infant care time (hour/day) | 2.96±2.39 | 2.84±1.73 | 3.09±2.90 | t = -0.64 |
Table 1: Demographic characteristics of infants and parents (n= 140) Note: Category variables were presented as percentages and c
Effect of the Interventions
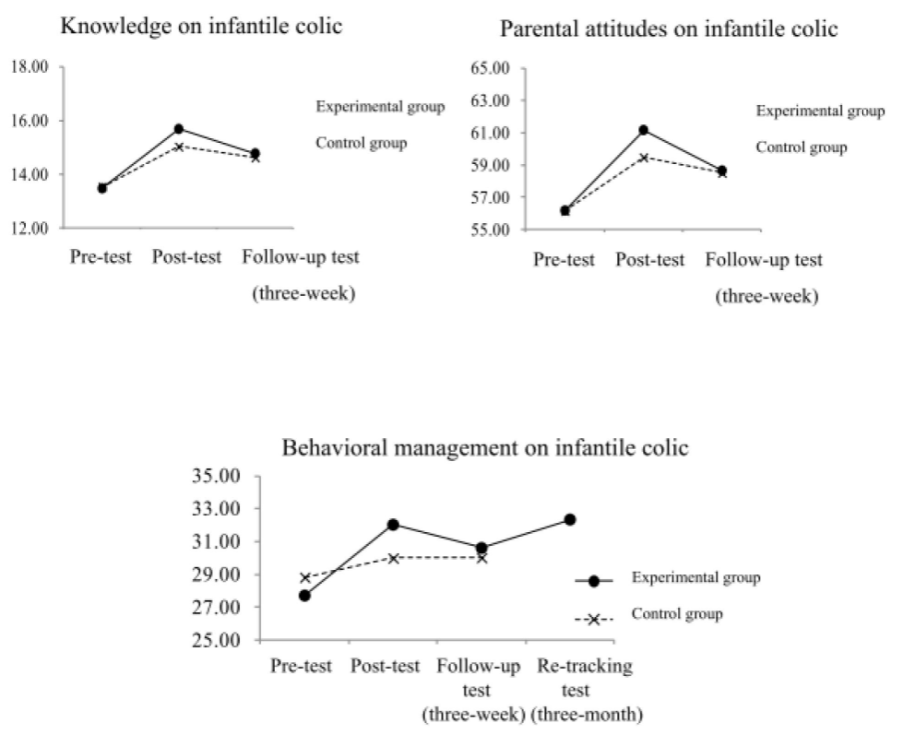
The participants (parents) did not reach a significant level (p> .05) in the pre-test, which indicated that there was no significant difference in the pre-test scores in the “knowledge level questionnaire on IC for parents”, “attitudes of parents towards IC”, and “behavioral management of parents on IC”. In the post-test neither group reached significant levels in “attitudes of parents towards IC” (p >.05). However, a significant difference was achieved in the scores of the “knowledge level questionnaire on IC for parents” and “behavioral management of parents on IC”, and the experimental group scored higher than the control group. The results showed that the effect of the ICHEP was significantly better than in the control group for both the knowledge and behavioral questionnaires. In the third-week after returning home, neither group achieved a significant level (p >.05), indicating that there was no significant difference in the tracking scores for all three questionnaires in both groups after three weeks (Table 2 & Figure 2).
| Group | Pre-test (N=140) | Post-test (N=140) | Group | Follow-up Test (N=135) | F-value | p-value | Comparison |
|---|---|---|---|---|---|---|---|
| M± SD | M± SD | M± SD | |||||
| Experimental group( n = 70 ) | Experimental group ( n = 68 ) | ||||||
| •Knowledge | 13.47±1.73 | 15.69±1.81 | •Knowledge | 15.69±1.81 | 31.69*** | <.00 | 2>3>1 |
| •Attitude | 56.17±4.75 | 61.17±5.97 | •Attitude | 58.66±4.71 | 15.17*** | <.00 | 2>3>1 |
| •Behavioral management | 27.70±3.87 | 32.01±3.52 | •Behavioral management | 30.60±3.68 | 25.31*** | <.00 | 2>3>1 |
| Control group (n=70 ) | Control group ( n = 67 ) | ||||||
| •Knowledge | 13.53±1.95 | 15.03±2.10 | •Knowledge | 14.62±1.73 | 12.56*** | <.00 | 2 - 3>1 |
| •Attitude | 56.14±4.60 | 59.47±4.18 | •Attitude | 58.51±4.69 | 13.14*** | <.00 | 2 - 3>1 |
| •Behavioral management | 28.81±3.58 | 29.99±3.64 | •Behavioral management | 30.01±3.10 | 3.25* | 0.04 | 3>1 |
Table 2: Differences in knowledge, attitudes, and behavioral management of parents on IC (Pre-post-test, n=140; the follow-up tes
Participants in the experimental group achieved a significant level on the F test at the four measurement time points (pre-test, post-test, three weeks after returning home, and three months after returning home). After comparison of LSD, parents in the experimental group whose infants had symptoms of intestinal colic recently (n = 24) had a significantly higher mean score in the re-tracking test (three months) than at the pre-test, post-test, and follow-up test. The mean scores of the post-test and follow-up test were significantly higher than the pre-test (Table 3 & Figure 3). The effect of the “behavioral management of parents on IC” in the experimental group in the re-tracking test was better than in the post-test and the follow-up test, indicating that the parents in the experimental group had significant effects on the behavioral management on IC(p <0.001).
In order to examine the effectiveness of the ICHEP, the generalized estimating equation (GEE) model was used for analysis. The factors include “group” (experimental group and control group), “time point” (pre-test, post-test, three- week test) and “interaction” (group × time point).
In the behavioral management on IC (Tables 4), “experimental group × post-test” (B = 3.14, p <.001) and “experimental group × three- week test” (B = 1.69, p = .026), the effects reached a significant level (p <.05), indicating that the two groups of participants have significant differences in the behavioral management on IC from the pre-test to the post-test and follow-up test.
| Time-point | Mean | Standard deviation | Source | Sum of squares | Degrees of freedom | Mean square sum | F | p-value | Comparison of LSD after test |
|---|---|---|---|---|---|---|---|---|---|
| ( 1 ) Pre-test | 26.79 | 3.74 | within group | 1518.45 | 3 | 506.15 | 44.64*** | <.00 | |
| ( 2 ) Post-test | 31.21 | 3.35 | deviation | 782.3 | 69 | 11.34 | 4>2>3>1 | ||
| ( 3 ) Follow- up test (three- week) | 29.92 | 4.17 | deviation | 782.3 | 69 | 11.34 | |||
| ( 4 ) Re- tracking test (three-month) | 37.71 | 3.82 |
Table 3: Analysis of the difference in behavioral treatment of infants with colic in the experimental group before and after the
Table 3: Analysis of the difference in behavioral treatment of infants with colic in the experimental group before and after the test, the follow-up test (third week after returning home) and the re-tracing test (three months after returning home, n = 24) Note: In the experimental group, 24 infants had symptoms of infantile colic for all 4 time points; ***p < .001
| Predictor variable | Knowledge on infantile colic | Behavioral management on infantile colic | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 95%CI | S.E. | Wald χ² | p value | 95%CI | S.E. | Wald χ² | p value | 95%CI | S.E. | Wald χ² | p value | |
| Experimental group | 13.53 (13.07 to 13.98) | 56.14 (55.07 to 57.21) | 28.81 (27.98 to 29.65) | |||||||||
| Groupa1 | -0.06 (-0.66 to 0.55) | 0.31 | 0.03 | 0.853 | 0.03 (-1.51 to 1.57) | 0.78 | 0 | 0.971 | -1.11(- 2.34 to 0.11) | 0.63 | 3.17 | 0.075 |
| Timea2 Post-test | 1.5 (0.82 to 2.18) | 0.35 | 18.58*** | <.001 | 3.33 (2.06 to 4.59) | 0.65 | 26.59*** | <.001 | 1.17 (0.02 to 2.32) | 0.59 | 4.00* | 0.045 |
| follow-up test (third week after returning home) | 1.1 (0.50 to 1.69) | 2.38 (1.04 to 3.72) | 1.2 (0.17 to 2.23) | |||||||||
| Group ×Time a3 Experimental group× Post-test | 0.71 (-0.14 to 1.57) | 0.44 | 2.7 | 0.101 | 1.67 (-0.33 to 3.68) | 1.02 | 2.67 | 0.102 | 3.14 (1.51 to 4.77) | 0.83 | 14.26*** | <.001 |
| Experimental group× follow- up test (third week after returning home) | 0.19 (-0.61 to 1.00) | 1.69 (0.20 to 3.19) |
Table 4: GEE models of two groups of participants at different time points a1:Group reference category:Control groups a2:Time ref
Discussion
The results showed that the p-value of the t-test of both the experimental group and the control group in the knowledge, attitudes, and behavioral management in the pre-test were higher than .05, indicating that the test results did not have a significant difference. In other words, the knowledge, attitudes, and behavioral management to IC of both groups were similar before the ICHEP. This result coincides with Al Qahtani AM & Ahmed HM [33] from Saudi Arabia for knowledge, attitudes, and practice of infant massage from mothers in 2020. However, the post-test after the intervention program found that parents of both groups had significant differences in the knowledge and behavioral management questionnaires. Scores from the experimental group were higher than for the control group. According to Davenport TH & Prusak L [34], knowledge can be changed and updated through stimulation and learning. Furthermore, behavior is a pattern reflected by individuals towards people, events, time, place, and position for the first time. Thus, behavior easily changes with direct increase of knowledge. However, there was no significant difference (p >.05) in parental attitudes. Marcon, et al. [35] reported that attitude is the process of emotionally, perceptually, and cognitively reacting to certain things through stimulation and must be obtained through an extended period of study. Therefore, the reason for not having a significant difference in attitudes might be that this study conducted the post-test immediately after the intervention program without the accumulation of learning time. Indicating that changes in attitudes may need time to develop.
The differences in among knowledge, attitudes, and behavioral management in three-time points (pre-test, post-test, and three weeks after) was analyzed. The results showed that the F test of all questionnaires reached a significant level after the intervention. This indicates a considerable benefit on the knowledge, attitudes, and practice towards IC after parents received ICHEP. This result was consistent with Pillitteri [36] and Chou, et al. [37] that reported that providing health education on diseases by nursing staff could increase the knowledge of caring for and the confidence in handling infants, and reduce parents anxiety of care. Indeed, some parents of the experimental group significantly improved their knowledge, attitudes, and behavioral management on IC compared to the control group after intervention program. Although the scores of knowledge, attitudes, and behavioral management in the experimental group were lower in the follow-up test three weeks after returning home, the effects were still better than in the control group. By analyzing and comparing the knowledge level before and after the intervention program, the result showed an increased knowledge level on IC from parents. This result was similar to results published by many scholars in Taiwan [38, 39], indicating that it would be beneficial to provide parents with health education and care knowledge by healthcare professionals about infant diseases early on. In the process of receiving health education, parents could promptly ask questions and clarify their doubts about infant disease care. Health care professionals could also be aware of the care issues faced by parents and immediately resolve doubts and guide parents. In terms of attitudes, the result was similar to Chen [40]. The reason for these results could be that parents in the experimental group still tended to be anxious and afraid even after the intervention program. However, attitudes in the experimental group changed in a more positive way after the addition of the follow-up telephone interview and discussion.
It also showed that after ICHEP parental attitudes toward IC had a more remarkable change in the experimental group than the control group. Yen, et al. [41] pointed out that parents’ behaviors were hard to change without a positive attitude. The ICHEP in this study could guide and encourage parents to talk about the care of infants with IC through two- way discussion and sharing. Not only the positive attitude of parents would be enhanced to face this disease, but the behavior of caring could also improve. Chiou, et al. [42] proposed that one-one health education model could shorten the gap between healthcare staff and patients. By providing the parents with verbal affirmation and appreciation during the interaction, mutual trust increased. Increasing mutual trust would allow parents to have a more positive attitude towards medical diagnoses and care plans. At the same time, by improving knowledge in the experimental group, behavioral management was transformed into effective care measures.
Finally, to deeper understand the situation of infants with IC after three months; this study performed a telephone interview. In the telephone interview, it was found that 24 of 70 infants in the experimental group had repeated IC during the three months of returning home. However, the parents of those 24 infants made fair use of the infant massage techniques and dietary precautions taught in the handbook to relieve IC. There was no emotional anxiety and fear during the treatment process and infants would not be taken to a physician for treatment unless multiple interventions were ineffective. For this study, a video of the infant massage technique from the International Association of Infant Massage was used to strengthen the behavioral management of parents on IC. The parents could read and practice at any time by scanning the QR code available in the handbook of health education care for IC. This extra step could enhance care knowledge and processing ability of parents, thereby reducing anxiety and stress. The handbook content design was similar to the one by Chou, et al. [43]. Knowledge transferred through electronic media was more effective than traditional narration; it enhanced parents’ positive attitudes and confidence in care, and changed the behavioral management on IC at home.
This study has two limitations. First, due to time and human resources constraints, only one hospital provided the ICHEP to parents of infants less than one year diagnosed with IC. It was indeed time-consuming and labor intensive to conduct one-on-one individual teaching in the hospital outpatient department. Second, we only measured the participants in ICHEP group in the follow up after three- month by telephone interview.
Conclusion
The results confirmed that the ICHEP improved the parents’ knowledge, attitudes, and behavioral management on IC. Because of the design and methods used, this evidence that ICHEP can enhance aspects of attitudes, knowledge level and behavioral management appears powerful and useful. Physicians have heard from parents about the anxiety and fear that crying infants provoke for unknown reasons. Some physicians, especially novices, are slightly unfamiliar with the treatment of IC. Therefore, it is essential to guide family members in observing whether crying is a symptom of IC to immediately provide correct care measures and reduce the anxiety of caregivers. The ICHEP designed by this institute could provide physicians with a systematic practical guideline on massage techniques and care details for on-the-job education and training courses. It could help understand the underlying causes of IC further. IC should be included in nursing textbooks to help students understand the cause and treatment of IC early on. Future research should include several hospitals and participants to facilitate the establishment of this guideline as a reference for clinical practice.
Conflict of Interest
The author declares that they have no competing interest.
Ethical Approval and Consent to Participants
An ethical permission was obtained from university ethical committee and consent form was sought from participant to the study.
Acknowledgments
The author wants to acknowledge a grant that supported this research: Department of Education and Medical Research at St. Joseph Hospital (Taiwan) and also wishes to thanks you all of the participants in this study.
References
-
Lewandowska A, Zych B (2017) Intestinal colic in newborn babies: incidence and methods of proceeding applied by parents. Journal of Education Health and Sport 7(6): 63-76.
-
Wolke D, Bilgin A, Samara M (2017) Systematic review and meta-analysis: fussing and crying durations and prevalence of colic in infants. The Journal of paediatrics 185: 55-61.
-
Wessel MA, Cobb JC, Jackson EB, Harris GS, Detwiler AC (1954) Paroxysmal fussing in infancy, sometimes called colic. Pediatrics 14(5): 421-435.
-
Drossman DA, Hasler WL (2016) Rome IV‐functional GI disorders: disorders of gut‐brain interaction. Gastroenterology 150(6): 1257-1261.
-
Zeevenhooven J, Koppen IJ, Benninga MA (2017) The new Rome IV criteria for functional gastrointestinal disorders in infants and toddlers. Pediatric Gstroenterology Hepatology Nutrition 20(1): 1-13.
-
Sarasu JM, Narang M, Shah D (2018) Infantile colic: an update. Indian paediatrics 55: 979-987.
-
Puntis JWL (2020) Childhood diseases 1. Gastrointestinal problems. Evaluation 14 (47):19.
-
Waddell LJ (2013) Management infantile colic: an update. Journal of Family Health Care 23(3):17-22.
-
Garrison MM, Christakis DA (2000) A systematic review of treatments for infant colic. Pediatrics 106 (1 Pt 2): 184-190.
-
Turner TL, Palamountain S(2008) available at www. uptodate.com/contents/infantile-colic-management
-
Cook F, Bayer J, Le HN, Mensah F, Cann W, et al. (2012) Baby business:a randomized controlled trial of a universal parenting program that aims to prevent early infant sleep and cry problems and associated parental depression. BMC Pediatrics 12(1): 13.
-
Heidi Murkoff, Arlene Eisenberg, Sandee Hathaway (2015) Infantile Colic. In: Liou HY, What to Expect the First Year. 3rd(Edn.), Taipei: Yuan-Liou Press, pp: 115- 187.
-
Aksoy Okan M, Gunduz M, Okur M, Akgun C, Esin K (2016) Does maternal diet affect infantile colic?. The Journal of Maternal-Fetal Neonatal Medicine 29(19): 3139-3141.
-
Chau K, Lau E, Greenberg S, Jacobson S, Yazdani- Brojeni P, et al. (2015) Probiotics for infantile colic: a randomized, double-blind, placebo controlled trial investigating lactobacillus reuteri DSM 17938. The Journal of Pediatrics 166(1): 74-78.
-
Critch J (2011) Infantile colic: is there a role for dietary interventions? Paediatrics Child Health 16(1):47-49.
-
McClure VS (2016) The Handbook of Instructor of Infant Massage. Taiwan: The International Association of Infant Massage.
-
Nahidi F, Gazerani N, Yousefi P, Abadi AR (2017) The comparison of the effects of massaging and rocking on infantile colic. Iranian journal of nursing and midwifery research 22(1): 67-71.
-
Bahrami H, Kiani MA, Noras M (2016) Massage for infantile colic: Review and literature. International Journal of Pediatrics 4(6): 1953-1958.
-
Oflu A, Bukulmez A, Gorel O, Acar B, Can Y, et al. (2020) Complementary and alternative medicine experiences of mothers in the treatment of infantile colic. Sudanese Journal of Paediatrics 20(1): 49-57.
-
Castejon-Castejon M, Murcia-Gonzalez MA, Gil JM, Todri J, Rancel MS, et al. (2019) Effectiveness of craniosacral therapy in the treatment of infantile colic. A randomized controlled trial. Complementary therapies in medicine 47:102164.
-
McClure VS (2017) Minor Illness and colic. In: Vimala Schneider McClure, Infant massage: A handbook for loving parents, United States: Bantam Press, pp: 203- 214.
-
(2020) Copyright and Permission Use of Health Promotion Administration, MOHW Website Text and Materials (The handbook of children health education).
-
Karp H (2021) The Happiest Baby on the Block; Fully Revised and Updated Second Edition: The New Way to Calm Crying and Help Your Newborn Baby Sleep Longer. Random House Publishing Group.
-
Nam SK, Park S, Lee J, Jun YH (2019) Clinical Characteristics of Infantile Colic. Neonatal Medicine 26(1): 34-40.
-
Indrio F, Miqdady M, Al-Aq F, Haddad J, Karima B, et al. (2017) Knowledge, attitudes, and practices of pediatricians on infantile colic in the Middle East and North Africa region. BMC paediatrics 17(1):1-7.
-
Al-Shehri H, Al-Mogheer BH, Al-Sawyan TH, Abualalaa AB, Jarrah OA, et al. (2016) Assessment of maternal knowledge about infantile colic in Saudi Arabia. Electronic Physician 8(12): 3313-3317.
-
Cetinkaya B, Basbakkal Z (2007) A validity and reliability study investigating the Turkish version of the Infant Colic Scale. Gastroenterology Nursing 30(2): 84-89.
-
Chen IL, Chwo MJ (2009) The problems and management of excessive crying and fussing in infants. Hu Li Za Zhi. The journal of nursing 53(4): 17-23.
-
Polit DF, Beck CT, Owen SV (2007) Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Research in Nursing Health 30(4): 459-467.
-
Wu ML (2010) Practice of questionnaire statistical analysis SPSS operation and application, In: Long WM.Chongqing: Chongqing University Press, pp: 1-539.
-
Escudero EB, Reyna NL, Morales MR (2000) The level of difficulty and discrimination power of the Basic Knowledge and Skills Examination (EXHCOBA). Revista electronica de investigacion educative 2(1): 2-16.
-
Ma Y, Mazumdar M, Memtsoudis SG (2012) Beyond repeated-measures analysis of variance: advanced statistical methods for the analysis of longitudinal data in anesthesia research. Reg Anesth Pain Med 37(1): 99- 105.
-
Al Qahtani AM, Ahmed HM (2020) The Effect of Educational Program for New Mothers about Infant Abdominal Massage and Foot Reflexology for Decreasing Colic at Najran City. Comprehensive Child and Adolescent Nursing 44(1): 63-78.
-
Davenport TH, Prusak L (1998) Working knowledge: How organizations manage what they know, Publisher: Harvard Business School Press, pp: 1-15.
-
Marcon ACC, Vieira MC, Morais MB (2014) Conhecimentos do pediatra sobre o manejo do lactente que chora excessivamentenos primeiros meses de vida. Revista Paulista de Pediatria 32(2): 187-192.
-
Pillitteri A (1999) Ch. 24. Nursing Care of the Child with a Gastrointestinal Disorder. In: Lippincott Williams & Wilkins, Child health nursing: care of the child and family 1rd (Edn.), Philadelphia, United States, pp: 796-810.
-
Chou YC, Yip WH, Chang LY, Lin CH (2012) Reducing Neonatal Vaccination Pain: The Effectiveness of Behavioural Interventions. Journal of Nursing Healthcare Research 8(1): 3-13.
-
Hsu HC, Chen SJ, Huang MC (2012) Efficacy of cultural- appropriate health education on information, motivation and behavioural skills of Fever management for children in new immigrant vietnamese mothers. Hu Li Za Zhi 59(6): 55-64.
-
Chen CF, Huang MC, Chen JY, Kuo PC (2012) Improving the attitudes, knowledge, concerns and practices of primary caregivers of febrile convulsion children: The efficacy of systematic nursing instruction. Journal of Nursing and Healthcare Research 8(4): 278-287.
-
Chen CF (2011) Effects of Systematic Nursing Instruction on Attitudes, Knowledge, Concerns and Practices Change of Primary Caregiver Having Febrile Convulsion Children. Thesis. institute of Nursing, Chung Shan Medical University. Taichung, Taiwan.
-
Yen CF, Tang TC, Ko CH, Lo WC (2005) The Influence of Depression on the Associations Between Substance Use and Other Risk Behaviours Among Adolescents. National Science Council, Executive Yuan.
-
Chiou MH, Wang HH, Yang YH (2007) Effect of systematic menstrual health education on dysmenorrheic female adolescents’ knowledge, attitudes, and self-care behaviour. The Kaohsiung journal medical sciences 23(4): 183-190.
-
Chou YY, Lee TY, Gau ML, Chen PJ, Chuang UL (2008) Effectiveness of a Video-based Breastfeeding Program on Breastfeeding Knowledge and Attitude among High School Students. Chang Guang Nursing 19(4): 461-471.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City