Hypertension and Type 2 Diabetes Mellitus Secondary to Acromegaly, A Rare Endocrine Disease: A Case Report
Background: Acromegaly is a rare endocrine disorder that emanates from excessive release of growth hormone leading to the production of insulin-like growth factor I (IGF-I) which causes most of the clinical features of the disease. Methods: A case report study of Acromegaly that presented in the Niger Delta University Teaching Hospital, Bayelsa State, Nigeria. Results: Random Blood Sugar -25mmol/dl, Fasting Blood Sugar-17.8mmol/dl, HbAIc-13.0%, Prolactin-6.64ng/ml, Cortisol- 12.5ug/dl, FSH-0.20Miu/ml, Testosterone-0.35ng/ml, TSH-1.26Uiu/ml, Growth Hormone; Insulin-like Growth Factor 1->1600ng (115-307). Her Blood Pressure was 180/120 mmHg. Heart sounds were S4, 1 and 2.Echocardiogram revealed concentric LVH, no regional wall motion abnormality. Perimetry showed inferior nasal defect of the Left eye. Conclusion: This case report reiterates the need for more health education and public enlightenment on clinical entities such as Acromegaly, with an emphasis on debunking some of the myths and social stigma associated with this chronic progressive disfiguring and disabling disease in our environment.
Background
Acromegaly is an endocrine disorder that emanates from excessive release of growth hormone leading to the production of insulin-like growth factor I (IGF-I) which causes most of the clinical features of the disease. It is caused by somatotroph adenomas of the pituitary gland but familiar causes including tumors associated with multiple endocrine neoplasia type I may occur as well.
In the early stages of the disease, diagnosis may be difficult to make because of the insidious onset of symptoms and slow progression in the pathogenesis [1].
The annual incidence of the disease is 3-4 cases per million globally. Men and women have equal frequency and it most often manifest when patients is in their 30s or 40s after being exposed to excessive GH for about 10 years [2]. Hyperprolactinemia accompany about a one third of the cases.
Acromegaly could lead to a two to three-fold increase in mortality in comparison to the age-and sex-matched general population [3, 4].
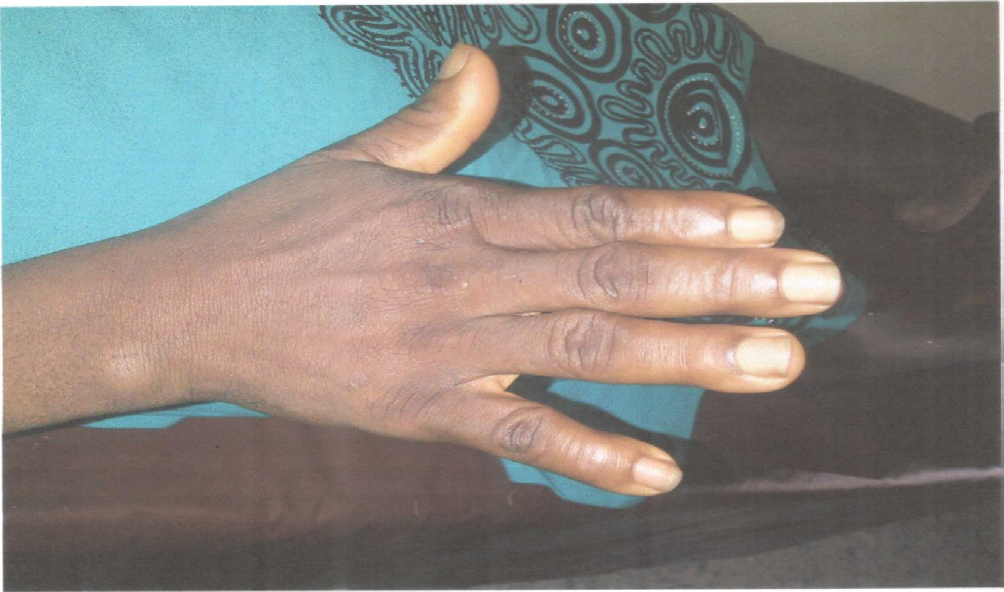
Acral bony overgrowth which occurs in acromegaly is associated with clinical features such frontal bossing, increased hand and foot size, mandibular enlargement among others. Soft tissue swelling resulting from the disease lead to increase in the size of the hand, and foot coarse facial features, including a big nose. Cardiomegaly, macroglossia, and thyroid gland enlargement are some of the visceramegaly that occur in the patients.
Acromegaly results in a number of complications that leads to a two- or four-fold increase in mortality and a decrease in life expectancy by about a decade [5].
Hypertension and type 2 Diabetes Mellitus secondary to acromegaly occurring in one patient is rare in Nigeria and there is dearth of publications in the literature.
A study done at the University College Hospital, Ibadan, Nigeria revealed that six patients were seen with acromegaly over a period of six years. There were 5 males and 1 female giving a sex ratio that is different from the equal sex prevalence in larger Caucasian series [6] Few other cases have been reported in the northern part of Nigeria [7, 8].
Therefore, this is a case report of a late presentation of Acromegaly complicated with type 2 DM and Secondary Hypertension at the Niger Delta University Teaching Hospital, Yenagoa, and South-South, Nigeria.
Case Report
A 45years old female reported to the Medical Outpatient Department of the Niger Delta University Teaching Hospital complaining of amenorrhea, since 10 years, and prominence facial features and enlargement of hands and feet of 4 years duration. Enlargement of face, hands and feet began with the face then progressed to involve the hand and legs.
There was an associated positive history of polyuria, polydipsia, polyphagia, vulva pruritus but no vaginal discharge. She also had a chronic headache and impairment of hearing. Headache was throbbing in nature, focal, affecting left side of the head and associated with dizziness and blurring of vision.
There was history of palpitations and generalized weakness but no history of facial, abdominal or leg swelling. There was a history of progressive weight gain. (Her weight increased from 77 kg to 99 kg and at presentation she had gained 22 kg.) She is not a known Diabetic or Hypertensive prior to the onset of these symptoms.
Physical examination showed a middle-aged woman with coarse facial features including enlarged lower jaw, large nose and lips, and frontal bossing, proptosis and hollow-sounding voice. Her hands and feet were enlarged. Her BMI was 39.2 Kg/m.2 Her pulse was 88 beats/min normal volume and regular. Her Blood Pressure was 180/120 mmHg. Heart sounds were S4, 1 and 2. A clinical diagnosis of Acromegaly associated with type 2 DM and Hypertensive Heart Disease was made and she was placed on Anti-Hypertensives medications and subcutaneous insulin following the results of her Random Blood Sugar of 25mmol/dl.
Investigation results findings were as follows: RBS -25mmol/dl, FBS-17.8mmol/dl, HbAIc-13.0%, Prolactin- 6.64ng/ml, Cortisol-12.5ug/dl, FSH-0.20Miu/ml, Testosterone-0.35ng/ml, serum estradiol 61 pmol/L, TSH- 1.26Uiu/ml, Growth Hormone; Insulin-like Growth Factor 1->1600ng (115-307).
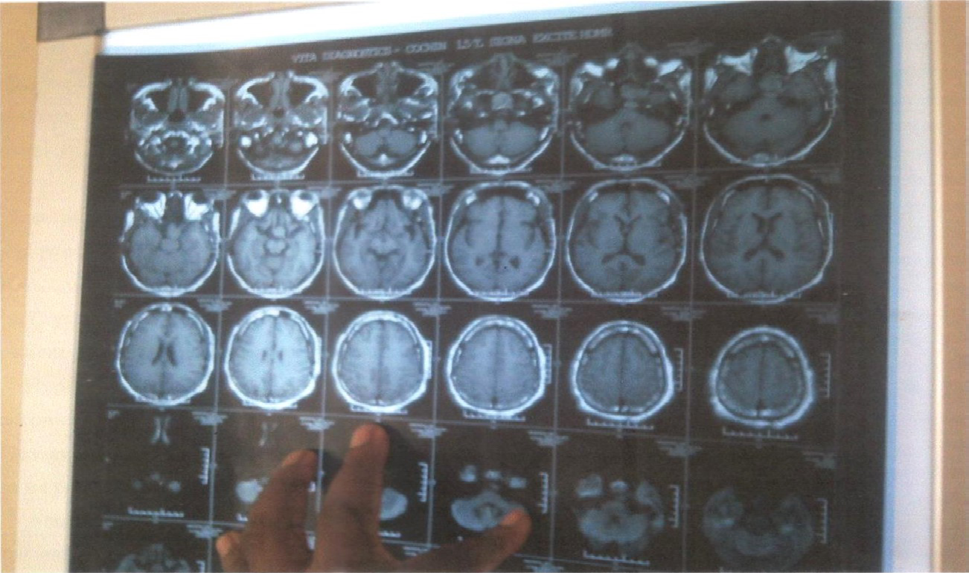
Brain MRI with contrast showed a sellarsuprasellar mass extending into the sphenoid sinus as well as well behind the clivus. There was an encasement of the cavernous carotid by the tumour. Echocardiogram revealed concentric LVH, no regional wall motion abnormality. Perimetry showed inferior nasal defect of the Left eye and bitemporal hemianopia.
The results of investigations supported the clinical diagnosis and she was eventually referred to a Neurosurgeon and she eventually had a trans-nasal, trans-sphenoidal excision to decompress the tumour, followed by post- operative fractionated radiotherapy. Histology report showed Pituitary Adenoma.
She underwent a successful brain neurosurgery and radiotherapy outside Nigeria but could not continue with the follow up because of the high financial cost. She has been placed on Lanreotide and Cabergoline among other medications. She had moderate clinical improvement and was coming for follow up in the Medical Outpatient Department of the Niger Delta University Teaching Hospital before she relocated.


Discussion
Acromegaly is not common in our practice. Our patient presented at age 43 years and had amenorrhea for 10 years, and other features of acromegaly for 4 years prior to presentation. This patient had amenorrhea when she was 33 years when her last child was 2 years old. She presented to us 10 years after the manifestation of the first symptom. This goes to demonstrate the slowly progressive nature of the disease and the lack of health awareness among our people.
This patient sought medical attention because of the progressive changes in her physical appearance and the severe symptoms of DM and Hypertension that manifested much later. Our patient was divorced by her husband because of her changed physical appearance and the myth attached to the disease. This revealed the level of social stigma associated with this chronic disabling and disfiguring condition.
She sought medical attention because of the progressive changes in her physical appearance and the severe symptoms of DM and Hypertension that manifested much later. Random Growth Hormone (GH) level measurements are not very useful in making the diagnosis of acromegaly because GH secretion is pulsatile. Insulin-like Growth Factor-I (IGF-I) levels provide a reliable means of .assessing the GH production and provide a standard screening test for acromegaly.
In this index patient, the serum level of IGF-1 was grossly elevated. The acceptable standard for the blood sugar test in acromegaly is the glucose tolerance test but it could not be carried out because of her elevated blood sugar. The glucose tolerance test was initially deferred because the blood sugar control was suboptimal but when the blood sugar was well controlled she was not willing to do further investigations. Her fasting blood sugar and hypertension was well controlled with high doses of anti-hypertensive and anti-diabetic medications following the surgery.
Thyroid function test, gonadotropins, and sex steroids values were found to be reduced in our patient because of tumor mass effects. Hyperprolactinemia has been the most common pituitary hormone disorder accompanying acromegaly. Acromegaly is complicated with galactorrhea in about one-third of patients.
However, she did not present with galactorrhea and her serum level of Prolactin was found to be normal. Some of the investigations ordered for her including colonoscopy and thyroid ultra sound scans were not done because of financial constraints. The full effect of the conventional radiation therapy that was carried out on her may not be seen for 10 or more years following the treatment so she continued Lanreotide, Cabergoline, bromocriptine, anti-hypertensive and anti-diabetic medications but she could not continue with some of the medications because of the high cost.
The surgery was done outside Nigeria and her post- surgery metabolic parameters were not available when she presented for follow up and repeat of the metabolic parameters could not be done because of financial constraints. She relocated when she was no longer having financial support to continue with the treatment.
Acromegaly accounts for a two- to three-fold increase in mortality rate. Most of the increased mortality is caused by cardiovascular and cerebrovascular diseases due to the increased prevalence of hypertension (25 to 35%) and diabetes mellitus (10 to 25%) in patients with acromegaly [9]. Our patient presented with type 2 DM and severe Secondary Hypertension.
Her Fasting Blood Sugar and Glycated Haemoglobin were 17.8mmol/dl and 13.0%, respectively. Her presenting Blood Pressure was 180/120mmHg. Ylli, et al. [10] found that in a 10-year retrospective review of acromegaly disease, the prevalence of DM and Hypertension was 64% and 55% respectively among the acromegaly patients in Albania.
Conclusions
This case report reiterates the need for more health education and public enlightenment on clinical entities such as Acromegaly, with an emphasis on debunking some of the myths and social stigma associated with this chronic progressive disfiguring and disabling disease in our environment. There is an urgent need for the government to provide the much needed state of the art equipment, qualified manpower and medications in our tertiary hospitals at a subsidized amount. This will go a long way in assisting sufferers of such rare disease accessible, affordable and quality health care.
Acknowledgment
We thank the patient and her father for permitting the use of her photographs. We also thank Drs F.C. Penawei and M. O. Boloupremo for their contributions.
References
-
Valkusz Z, Toth M, Boda J, Nagy E, Julesz J (2011) The importance of early diagnosis of acromegaly. OrvHetil 152(18): 696-702.
-
Melmed S, Larry Jameson J (2006) Disorders of the anterior pituitary and the hypothalamus. In: Larry Jameson J, et al. (eds), Harrison’s Endocrinology. The McGraw-Hill companies (publishers), pp: 19-56.
-
Bates AS, van’t Hoff W, Jones JM, Clayton RN (1993) An audit of outcome of treatment in acromegaly. Q J Med 86(5): 293-299.
-
Orme SM, Mcnally RJ, Cartwright RA, Belchetz PE, et al. (1998) Mortality and cancer incidence in acromegaly: a retrospective cohort study. United Kingdom Acromegaly Study Group. Clin Endocrinol Metab 83(8): 2730-2734.
-
Rajasoorya C, Holdaway IM, Wrightson P, Scott DJ, Ibbertson HK (1994) Determinants of clinical outcome and survival in acromegaly. Clinical Endocrinology 41(1): 95-102.
-
Famuyiwa OO, Bella AF, Akinlade KS (1990) Acromegaly in Ibadan—a report of six cases West Afr J Med 9(3): 232-238.
-
Shehu, B B, Ismail NJ, Jimoh Images AO (2004) In Clinical Practice – Pituitary Macroadenoma. Annals of African Medicine 3(2): 93-94.
-
Anumah F, Danbauchi S, Garko S (2008) Acromegaly Presenting as Cardiac Failure. Ethnicity & Disease 18(1): 104-106.
-
Molitch ME (2012) Anterior Pituitary. In Goldman Cecil Medicine 24th(Edn), The Saunders and Imprint of Elsevier (Publishers), pp: 1436-1437.
-
Ylli Z, Laku AB, Ylli D, Katia M, Fureraj T, et al. (2011) A Study of Epidemiological Characteristics and Treatment Outcome in Albanian Acromegalic Patients. Journal of Medical Research and Science 1(3): 1-9.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City