Impact of Structured Teaching Program on ICU Nurses’ Knowledge and Practice in Prevention of Ventilator Associated Pneumonia in Khartoum, Sudan
Background: Ventilator-Associated Pneumonia (VAP) is a prevalent hospital-acquired infection associated with increased mortality rates. Nurses play a significant role in preventing VAP by providing round-the-clock care to critically ill patients. This study aimed to evaluate the effectiveness of a Structured Teaching Program (STP) on ICU nurses’ knowledge and practices regarding VAP prevention in Khartoum. Methods: A quasi-experimental study with comparison groups (intervention and control) was conducted using purposive sampling. Data on knowledge and skills were collected from 120 ICU nurses using a structured knowledge questionnaire and direct observation checklist. The STP was implemented, followed by a post-test and final assessment after two weeks, using the same questionnaire and checklist. Data were analyzed using the Statistical Package for the Social Sciences (SPSS) program version 20. Results: The overall mean pre-test knowledge scores on VAP prevention were 17.95 out of 40 for the intervention group and 18.5 out of 40 for the control group, with a statistically insignificant difference (p=0.617>0.05). The post-test scores were 32.05 out of 40 for the intervention group and 20.83 out of 40 for the control group, showing a statistically significant difference (p=0.000<0.05). The overall mean initial assessment of practice compliance was 9.27 out of 20 for the intervention group and 4.97 out of 20 for the control group, with a statistically significant difference (p=0.000<0.05). In the final assessment, the mean scores were 12.77 out of 20 for the intervention group and 5.7 out of 20 for the control group, also showing a statistically significant difference (p=0.000<0.05). The VAP incidence rate during the pre-intervention phase was 54.4 cases per 1000 ventilator days for the intervention group and 40.35 cases per 1000 ventilator days for the control group. In the post-intervention phase,the rates were 39.6 cases per 1000 ventilator days for the intervention group and 64.9 cases per 1000 ventilator days for the control group. Conclusion: The findings indicate a knowledge deficit and inadequate practice compliance among ICU nurses regarding VAP prevention before the intervention. The structured teaching program effectively improved their knowledge and practice compliance, resulting in a reduction in VAP incidence rates.
Introduction
Ventilator-associated pneumonia (VAP) is the most common infectious complication among patients admitted to intensive care units (ICUs), it refers to pneumonia that has developed in patients who are receiving mechanical ventilation and develop it within 48 to 72 hours after tracheal intubation [1].
VAP represents a common nosocomial complication arising in the ICU, affecting 8 to 20% of ICU patients and up to 27% of mechanically ventilated patients [2]. VAP is the leading cause of hospital-acquired infections in the ICUs [3]. In 2002, an estimated 250,000 healthcare-associated pneumonias developed in U.S.A. hospitals and 36,000 of these were associated with deaths. Patients with mechanically- assisted ventilation have a high risk of developing healthcare- associated pneumonia. For the year 2010, National Health care Safety Network (NHSN) facilities reported more than 3,525 VAPs and the incidence for various types of hospital units ranged from 0.0-5.8 per 1,000 ventilator days [4]. Mortality rate in patients with VAP range from 20 to 50% and may reach more than 70% when the infection is caused by multi-resistant and invasive pathogens [5, 6, 7].
VAP is a significant concern in developing countries, occurring at a rate of 37.2 cases per 1000 ventilation days with an alarming 80% mortality rate. It leads to prolonged ICU stays, extended mechanical ventilation, and higher hospitalization costs [5, 8, 9, 10]. The main cause of VAP is microaspiration of or pharyngeal organisms around the end tracheal tube’s cuff, leading to bacterial proliferation and lung infection. Pseudomonas aeruginosa, Klebsiella species, Enterobacter species, and nontypable Homophiles influenzae are common gram-negative isolates, while Staphylococcus aureus, including resistant strains, is the most frequent gram- positive isolate [11, 12]. Diagnosing VAP is complicated due to the lack of a gold standard, but the CDC has established clinical criteria involving abnormal chest radiographs and specific symptoms for confirmation in patients ventilated for 48 hours or more [10].
Given the above statistics, it would be safe to conclude that the high incidence, costs of treatment and the high mortality rates associated with VAP are suggestive of either a gap in knowledge of VAP or a failure to translate that knowledge into practice by those caring for this patient population. Healthcare delivery has shifted toward evidence- based practice in recent years and the goal of evidence-based practice is to improve and provide high quality health care, resulting in positive patient outcomes [13].
A number of evidence-based guidelines have been developed in recent years to direct clinical practice in an attempt to improve patient care, and in particular care of the critically ill. Specificguidelines have been developed to both prevent VAP and treat it appropriately as soon as possible. Main preventive strategies include proper positioning, use of sterile equipment and educational strategies for educating health care personnel regarding prevention of VAP [14].
Numerous studies exist regarding evidence- based measures for preventing VAP, however, only a few studies have been performed in recent years to assess the impact of an educational program on knowledge and its impact on practice in preventing VAP [13, 15]. Although there is currently no literature to show a definitive correlation between the use of ventilator bundles and a decrease in VAP rates, there is strong evidence to suggest a positive association between the two [16]. There also remains a deficiency in literature regarding nurses’ knowledge of VAP and its preventive measures.
VAP is a serious complication of mechanical ventilation with high morbidity and mortality rate [7, 17]. ICU nurses’ knowledge and role in preventing VAP is paramount in reducing its occurrence. According to Vandijck, Lobeau, Volgelares and Blot, knowledge is a primary precondition for compliance with protocol for preventing VAP [18]. Given the deficiency in current literature regarding direct studies to examine ICU nurses’ knowledge of VAP, this study will provide an opportunity to examine groups of ICU nurses’ knowledge before and after an educational program on VAP. The study will also assess the impact of that educational intervention on nursing practice in preventing VAP.
Methods
Study Design
This is a quasi-experimental study design. This study employed the equivalent groups design (EGD), which comprised of a pretest and a posttest for intervention and control group. The study was carried out in three ICU environments in three phases. Two ICU were used as the control and the other one as the experimental unit.
Study Population
The target population of the study was: • Registered Staff Nurses working at Khartoum Teaching
Hospital, The National Ribat University Hospital and Omdurman Military Hospital. A total number of 120 subjects were chosen for the study. • Adult patients on mechanical ventilation admitted to ICU at Khartoum Teaching Hospital, Omdurman Military Hospital and The National Ribat University Hospital during the study period.
Criteria for Selection of the Sample for Nurses
Inclusion Criteria:
- Registered nurses with an intensive care (ICU) qualification, including permanent and temporary staff.
- Registered nurses with no formal training in ICU. These nurses were included as they are in close contact with mechanically ventilated patients and need to be familiar with ventilator associated pneumonia and the current evidence based guidelines for prevention of VAP.
- Nurses who were available at the time of data collection.
- Nurses who were willing to participate in the study.
Exclusion Criteria:
- Enrolled and auxiliary nurses as their category of nursing are not expected to have skills and in depth knowledge of mechanical ventilation and evidence based guidelines on prevention of VAP.
- Nurses who were working in areas other than Adult Intensive Care Unit.
For Patients
Inclusion Criteria:
- Adult patients on mechanical ventilation during the Period of the study. Exclusion Criteria:
- Patients develop pneumonia in less than 48 hrs. from initiation of mechanical ventilation.
- Transferred patients from other hospital on mechanical ventilation.
- Patient with Pneumonia before the initiation of mechanical ventilation.
Study Phases
Phase 1: The researcher observed the participants practice compliance regarding twenty elements of the ventilator associated pneumonia prevention international guidelines from CDC 2003 that related to nursing practice (infection control measures, ventilator care measures, end tracheal care measures and aspiration and colonization prevention strategies) and measured the VAP incidence rate in both the intervention and control groups prior to the educational session on at least 90 ventilator days.
Phase 2: In phase 2, participants in the interventional group and control group completed the multiple choice question (MCQ) assessment tests before an educational program on VAP.The intervention consisted of small group sessions of a 60-minute on VAP and its prevention strategies in order to afford all nurses an equal opportunity to participate. The Structured education program was prepared and delivered by the researcher. The researcher collaborated with the clinical nurse educators to design and put together handouts (self-study education modules) (annex I), a power point presentation and wall poster about VAP prevention keys (annex II).The pretest was administered to all participants during their work hours. Small group educational sessions were given immediately following the pretest. Participants were afforded time to ask questions regarding subject material covered during the educational program. To ensure that all nurses in intervention group will attend the education program. The researcher administered the sessions in the morning and evening nurses working time for un busy nurses by head nurses team coordinate, and to encourage them more to participate in the study the researcher coordinates with ICU matron to afford the nurses attendance certificate from the hospital administration in educational program for VAP prevention after they completed the post- test questionnaire.A posttest was then administered after 2 weeks from end of the educational program and the attendance certificate in the program was awarded to the participants (Annex III). The VAP prevention key poster also putted in ICU wall to remind the staff all the time. In the same time the post-test also administered to control group.
Phase 3: An observation of VAP practice in the intervention and control ICU was conducted during this phase. The researcher performed the observation over a two-week period and results were collected and tallied, and VAP incidence rate was measured for at least 60 ventilator days.
Study Setting
The study was conducted in the Khartoum Teaching Hospital, Omdurman Military Hospital and Al-Ribat University Hospital. The criteria for selecting these setting were geographical proximity, feasibility for conducting the study, availability of the required sample because nurses working in these units are responsible for a larger population of mechanically ventilated patients than other nurses in an acute care hospitals, and familiarity of the investigator with these settings.The military hospital is located in Omdurman district beside the Nile in the Morgan area (annex IVa). It provides all health services for army forces and their families (during service and retirement). It consists of many clinics and many wards such as; medical wards, obstetrics and gynecology, pediatrics wards, nursery, ICU and CCU and surgical wards. The ICU department receives the medical and surgical cases, in addition to emergency admissions provide a comprehensive intensive care. There are 22 beds in the ICU and covered by 109 nurses, working in two shift; 8 hours morning shift and 16 hours afternoon and night shift with 1: 1 nurse to patient ratio. Al-Khartoum teaching hospital is the largest hospital in Sudan, a public hospital, located in the center of Khartoum, near to Khartoum University, faculty of medicine (annex IVb). It consists of many clinics and many wards such as; medical wards, obstetrics and gynecology, pediatrics words, nursery, ICU and CCU and surgical wards. The ICU department receive the medical and surgical cases, in addition to emergency admissions, it provides intensive care by limited resources. There are 16 bed in the ICU, and covered by 58 nurses working in two shifts; 8 hours in morning and 16 hours in afternoon and night shift. The Ribat University Hospital is well equipped building to present the ideal health services for the surrounding population. It locates at Burry area of Khartoum (annex IVc). The Ribat University Hospital is the central hospital which was established to offer medical care to police forces and their families (during service and retirement) and for chronic cases referred from different state police hospitals. It consists of many clinics and many wards such as; medical wards, obstetrics and gynecology, pediatrics wards, nursery, ICU and CCU and surgical wards. The ICU department receives the medical and surgical cases, in addition to emergency admission, provide intensive care by limited resources. There are 10 beds in the ICU, and covered by 24 nurses, working in two shifts; 8 hours in morning and 16 hours in afternoon and night shift.
Sampling
Sample Size: The sample size for the present study was 120 nurses and 113 Patients.
Sampling Technique
- For Nurses: This study utilized a nonprobability sampling of 120 ICU nurses from Khartoum Teaching Hospital, Omdurman Military Hospital and the National Ribat University hospital. Sixty nurses (from Omdurman military hospital) were in the interventional group as total coverage sample and 60 nurses (from Khartoum Teaching Hospital and the National Ribat University Hospital) were in the control group as convenience sample.
- For Patients: This Study utilized Total covering Sample for adult patients on mechanical ventilation that admitted during the period of the study who met the study inclusion criteria (annex V).
Data Collection
Selection and Development of Tools: A structured knowledge questionnaire, Observation check list were selected for the study to assess nurses’ knowledge and practice compliance and patient ICU sheet to measure the incidence of VAP among patients under study. It was considered to be the most appropriate instrument to elicit the response from subjects.
Preparation of Structured Teaching Program (STP) a) Preparation of First Draft of STP: First draft of STP was developed, keeping in mind the objectives, criteria checklist, literature reviewed and the opinion of experts. The main factors that were kept in mind while preparing STP were: professional qualification of the subjects, method of teaching to be adopted, simplicity of language, and relevance of teaching aids. b) Content Validity of the Teaching Plan: The initial draft of structured teaching program was given to experts in the field along with the tools. The suggestions were incorporated in the structured teaching program and tools. c) Preparation of Final Draft of STP: The final draft of STP was prepared after incorporating expert’s suggestion; the final teaching plan got its shape after the modifications based on the opinion of guide. d) Selecting the Method of Teaching: Lecture cum discussion method was selected as an appropriate method of teaching staff nurses. It was planned to teach in small groups. e) Selection and Preparation of Appropriate Audio- Visual Aids: LCD, Flash cards, chalk board and charts were considered appropriate to increase the impact of teaching. f) Planning to Implement the Structured Teaching Program: The time and date to implement the structured teaching program was planned and decided in co- ordination with the Medical Superintendent/Director and the Nursing superintendent of the concerned hospitals. g) Determining the Method of Evaluating the Structured Teaching Program: The evaluation of structured teaching program was planned through conducting post-test after 2 weeks of implementation of structured teaching program. h) Description of Structured Teaching Program: The STP was titled “Prevention of Ventilator Associated Pneumonia”. The STP was structured for one session, which was prepared to enhance knowledge of ICU staff nurses regarding Ventilator Associated Pneumonia and its prevention.
Pilot Study
A pilot study was conducted from 30-8-2014 to 5-09- 2014 at Omdurman Military Hospital, Khartoum, Sudan.
Administrative approval was obtained from the Hospital administration to conduct the pilot study. The purpose of the pilot study was to:
- Evaluate the effectiveness of structured teaching program and reliability of tools
- Find out the feasibility of conducting the final study and
- Determine the method of statistical analysis After selecting 10 staff nurses by purposive sampling technique, pre-test was administered by using the structured knowledge questionnaire and initial assessment of performance by direct observational check list. On the same day, STP was administered for 60min.After 7days, the post-test was administered by using the same structured knowledge questionnaire and observation check list to evaluate the effectiveness of STP on the knowledge and practice compliance regarding Prevention of VAP and reliability of tools. The findings of the Pilot Study revealed that the Study is feasible.
Period of Data Collection: Formal permission was obtained from the Director and Medical Superintendent of Khartoum Teaching Hospital, the National Ribat University Hospital and Omdurman Military Hospital (annex X).
Variables under Study a) Independent Variable (IV): Structured Teaching Program (STP) b) Dependent Variable (DV): Knowledge of ICU Staff Nurses on prevention of VAP, incidence of VAP and Practice of ICU Staff Nurses on prevention of VAP. c) Attribute Variables (AV): Personal characteristics which include Age, Professional Educational qualification, and total clinical experience in years, and previous education training program on VAP.
Data Analysis
The data obtained were analyzed in terms of achieving the objectives of the study using descriptive and inferential statistics.
Descriptive Statistics:
- Frequencies and percentage distribution were used for analyzing of socio demographic characteristics and the level of knowledge.
- Mean, Mean percentage and standard deviation were used for analyzing pre-test and post- test scores.
Inferential Statistics:
- Application of paired ‘t’ test to ascertain whether there is a significant difference in the mean knowledge score and practice compliance scores of pre-test and post-test values for intervention and control groups.
- Application of independent ‘t’ test to ascertain whether there is a significant difference in the mean knowledge score and practice compliance scores of intervention and control groups pre-test and post-test values.
Results
Section I: Demographic Date The majority of the participants in the intervention group age between (21-27 years), while in the control group the age between (25-33 years). Most of the participants in the intervention and control group were females. The experience of the intervention group and the control group varies. Also the education level varies for both groups (Table 1).
| Variables | Intervention (n=60) | Control (n=60) | Significant | |||
|---|---|---|---|---|---|---|
| Freq. | Percent | Freq. | Percent | Chi x2 | p value | |
| Gender | ||||||
| - Male | 13 | 21.67 | 21 | 35 | 3.065 | 0.08 |
| - Female | 47 | 78.33 | 39 | 65 | ||
| Age | ||||||
| - Mean | 23.98 | 29.45 | 0.000* | |||
| - Std. deviation | 2.81 | 4.02 | ||||
| Level of qualifications | ||||||
| - Diploma | 0 | 0 | 9 | 15 | ||
| - Bachelor | 57 | 95 | 47 | 78.33 | 4.095 | 0.06 |
| - Master | 3 | 5 | 4 | 6.67 | ||
| Experience years | ||||||
| - Less than 1 year | 40 | 66.67 | 17 | 28.33 | ||
| - (1-5) years | 14 | 23.33 | 33 | 55 | 29.42 | 0.000* |
| - (6-10) years | 3 | 5 | 8 | 13.33 | ||
| - More than 10 years | 3 | 5 | 2 | 13.33 | ||
| Possession Diploma in I.C.U | ||||||
| - Yes | 5 | 8.33 | 19 | 31.67 | 17.17 | 0.000* |
| - No | 55 | 91.67 | 41 | 68.33 | ||
| Attendance an education program in infection control: | ||||||
| - Yes | 31 | 51.67 | 33 | 55 | 2.055 | 0.1 |
| - No | 29 | 48.33 | 27 | 45 |
Table 1: Distribution of study subjects (Intervention and control groups) regarding their demographic background (n=120).
*significant at 5% level. Table 1: Distribution of study subjects (Intervention and control groups) regarding their demographic background (n=120).
Section II: Effect of Educational Program on Nurses Knowledge The knowledge levels for the intervention group of pre and post- test were significant different (p=0.000<0.05).
Knowledge level Category Pre-test (n) Post- test (n) (x2) p value Inadequate < 50% Score 36 0
0.000* Moderate 50-75 % Score 24 17
Adequate > 75% score 0 43
Where the majority of the participants in pre- test had inadequate knowledge level, while in the post-test had adequate level of knowledge (Table 2).
Respondents of knowledge (Intervention group )
Total 60 60
* Significant at 5% level X2(2df) =80.95. Table 2: The difference in pre and post-test knowledge level for study subjects (intervention group) to assess the ICU nurses knowledge regarding VAP prevention (n=60).
The education program improved the nurses’ knowledge scores. Where the overall mean of pre-test knowledge scores for the intervention group was (17.95 out of 40) and become (32.05 out of 40) in post-test (Table 3).
| Test time | Max score | Respondents Knowledge (intervention group) | Paired “t” test p value | |
|---|---|---|---|---|
| Mean | SD | |||
| Pre-test | 40 | 17.95 | 5.58 | 0.000* |
| Post-test | 40 | 32.05 | 3.77 | |
| Enhancement | 14.1 | 4.75 |
Table 2: Overall mean of pre and post-test knowledge scores for (intervention group) subjects regarding prevention of VAP (n=60).
*significant at 5% level. t (59)=-16.31. Table 3: Overall mean of pre and post-test knowledge scores for (intervention group) subjects regarding prevention of VAP (n=60).
The means of pre and post-test knowledge aspects scores for the intervention group were significantly different (p=0.000<0.05) which indicated the education program enhanced and improved all knowledge aspects of VAP prevention for nurses’, especially regarding general information of VAP and diagnosis and treatment of it (Table 4).
| No | Knowledge aspects | Respondents knowledge (intervention group) | Paired “t” test p value | ||||
|---|---|---|---|---|---|---|---|
| Pre test | Post test | Enhancement | |||||
| Mean | SD | Mean | SD | Mean | |||
| I | General information of VAP | 2.85 | 1.36 | 5.1 | 0.85 | 2.25 | 0.000* |
| II | Anatomy of Lungs | 0.88 | 0.84 | 2.17 | 0.8 | 1.29 | 0.000* |
| III | Mechanical ventilation | 3.02 | 1.58 | 4.38 | 0.73 | 1.36 | 0.000* |
| IV | Diagnosis and treatment | 1.88 | 1.3 | 4.15 | 1.19 | 2.27 | 0.000* |
| V | International guidelines for VAP Prevention | 9.58 | 2.67 | 16.2 | 1.91 | 6.62 | 0.000* |
Table 3: Means of pre and post-test Knowledge aspects scores for (intervention group) subjects regarding Prevention of VAP (n=60)
*significant at 5% level. Table 4: Means of pre and post-test Knowledge aspects scores for (intervention group) subjects regarding Prevention of VAP (n=60).
The knowledge level of the control group was not different in pre and post- test (p=0.111>0.05). Where the majority of the participants had an inadequate knowledge level in pre and post-test (Table 5).
| Knowledge level | Category | Respondents of knowledge (Control group) | (x2) p value | |
|---|---|---|---|---|
| Pre test | Post test | |||
| Inadequate | < 50% Score | 41 | 30 | 0.111 |
| Moderate | 50-75 % Score | 17 | 28 | |
| Adequate | > 75% score | 2 | 2 | |
| Total | 60 | 60 |
Table 4: ** The difference in the pre and post-test knowledge level among (control group) subjects regarding prevention of VAP (n
* Not Significant at 5% level X2(2df) =4.39 Table 5: The difference in the pre and post-test knowledge level among (control group) subjects regarding prevention of VAP (n=60).
The overall mean of knowledge scores for the control group was not different in pre and post- test (p=0.08>0.05) (Table 6).
| Time of test | Max score | Respondents Knowledge (control group) | Paired “t” test p value | |
|---|---|---|---|---|
| Mean | SD | |||
| Pre-test | 40 | 18.5 | 6.39 | 0.08 |
| Post-test | 40 | 20.83 | 5.74 | |
| Enhancement | 2.33 | 9.8 |
Table 5: Overall mean of pre and post-test knowledge scores for (control group) subjects regarding prevention of VAP (n=60).
*Not significant at 5% level. t(59)=-1.733 Table 6: Overall mean of pre and post-test knowledge scores for (control group) subjects regarding prevention of VAP (n=60).
The means of pre and post-test knowledge aspects scores for the control group were not different (p>0.05), except regarding general information about VAP where there was a significant difference (p=0.001<0.05), also regarding mechanical ventilation care (p=0.008<0.05) (Table 7).
| No | Knowledge aspects | Respondents knowledge (control group) | Paired “t” test p value | ||||
|---|---|---|---|---|---|---|---|
| Pre test | Post test | Enhancement | |||||
| Mean | SD | Mean | SD | Mean | |||
| I | General information of VAP | 2.35 | 1.54 | 3.3 | 1.16 | 0.95 | 0.001* |
| II | Anatomy of Lungs | 1.47 | 1.01 | 1.67 | 0.95 | 0.2 | 0.344 |
| III | Mechanical ventilation | 2.3 | 1.03 | 2.83 | 1.04 | 0.53 | 0.008* |
| IV | Diagnosis and treatment | 2.53 | 1.7 | 2.8 | 1.61 | 0.27 | 0.406 |
| V | International guidelines for VAP Prevention | 9.85 | 3.74 | 10.2 | 3.32 | 0.35 | 0.593 |
Table 6: Means of pre and post-test Knowledge aspects scores for (control group) subjects regarding Prevention of VAP (n=60).
*significant at 5% level. Table 7: Means of pre and post-test Knowledge aspects scores for (control group) subjects regarding Prevention of VAP (n=60).
Section III: Effects of Educational Program in Nurses Practice The majority of the study subjects in the intervention group improved in practicing compliance in final assessment No. Practice items Infection control measures
1 Wash hand before and after patient contact. 40 63.3 0.03* 26.7 33.3 0.48
2 Wash hand between patients. 46.7 66.7 0.05 36.7 36.7 1
3 Change gloves between patients. 46.7 73.3 0.003* 30 40 0.32
Ventilator care measures
4 Drain and discovered periodically any condensate that collects in the tubing of M.V. 53.3 76.7 0.006* 30 43.3 0.25
5 Humidity respiratory circuit using humidifier. 93.3 96.7 0.57 30 50 0.08
6 Using new ventilator circuits for each patient. 100 100 - 73.3 93.3 0.03*
7 Changing ventilator circuits when become soiled 63.3 66.7 0.78 20 30 0.32
8 Using sterile water to full bubbling humidifier. 60 73.3 0.37 23.3 36.7 0.25
Endotracheal care measures
9 Maintain adequate pressure in endotracheal 73.3 90 0.02* 0 0 -
10 Wear clean gloves with closed suction system. NA NA NA NA NA NA
11 Wear sterile gloves with an open suction system. 66.7 83.3 0.09 46.7 53.3 0.6
12 Using sterile technique when applying tracheal suctioning. 23.3 53.3 0.009* 20 26.7 0.42
13 Sterilization or disinfection of suction equipment. 50 63.3 0.04* 20 16.7 0.76
14 Avoid Saline lavage with suctioning. 40 66.7 0.009* 30 36.7 0.57
Aspiration and colonization prevention measures
15 Monitor continuous patient positions (300-450) if not contraindicated. 53.3 93.3 0.000* 33.3 46.7 0.4 from initial assessment in the most items (p<0.05), while no significant difference found in the control group (p>0.05) (Table 8).
Intervention paired p value
Control paired p value Initial Final Initial Final
% % % %
| 16 | Perform regular oral hygiene with antiseptic mouth wash. | 43.3 | 63.3 | 0.01* | 26.7 | 23.3 | 0.74 |
|---|---|---|---|---|---|---|---|
| 17 | Use topical antimicrobial agents for oral decontamination. | 26.7 | 36.7 | 0.08 | 0 | 0 | - |
| 18 | Perform regular oral suction. | 46.7 | 63.3 | 0.05 | 30 | 26.7 | 0.769 |
| 19 | Continuous aspiration of subglottic secretion if ventilator more than 48 hours. | NA | NA | NA | NA | NA | NA |
| 20 | Check the gastric residual volume (GRV) every 4 to 6 hours. | NA | 53.3 | 0.000* | ND | ND | ND |
Table 7: ** The difference in initial and final assessment of practice compliance for study subjects (intervention and control gr
*Significant at 5% level. NA= Not Available. ND= Not Done.v Table 8: The difference in initial and final assessment of practice compliance for study subjects (intervention and control group) when assess the ICU nurses regarding VAP prevention (n=120) The means of initial and final assessment performance elements compliance had a significant difference in intervention group for all elements (p<0.05), while there were no difference in the control group (p>0.05) (Table 9).
| No | Elements | Max. score | Intervention | Paired p value | Control | Paired p value | ||
|---|---|---|---|---|---|---|---|---|
| Initial mean | Final mean | Initial mean | Final mean | |||||
| I | Infection control measures. | 3 | 1.33 | 2.03 | 0.002* | 0.93 | 1.1 | 0.37 |
| II | Ventilator care measures. | 5 | 3.7 | 4.1 | 0.05 | 1.97 | 2.33 | 0.14 |
| III | Endotracheal suction care. | 6 | 2.53 | 3.53 | 0.000* | 1.17 | 1.33 | 0.47 |
| IV | Prevent aspiration and colonization | 6 | 1.7 | 3.1 | 0.000* | 0.9 | 0.97 | 0.75 |
Table 8: Means of initial and final assessment performance compliance scores for study subjects (intervention and control) with e
*Significant at 5% level. Table 9: Means of initial and final assessment performance compliance scores for study subjects (intervention and control) with elements of VAP prevention (n=120).
The applied education program provided positive impact in nurses performance compliance in intervention group, where there was significant difference between the initial assessment mean and final assessment mean (p=0.000<0.05). While in the control group no significant difference (p=0.07>0.05) (Table 10).
| Max Score | Intervention group | Paired “t test” p value | Control group | Paired “t” test p value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Initial assessment | Final assessment | Initial assessment | Final assessment | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| 20 | 9.27 | 2.8 | 12.77 | 2.31 | 0.000* | 4.97 | 2.15 | 5.73 | 2.13 | 0.07 |
| Enhancement In Mean | 3.5 | 0.76 |
Table 9: Overall mean of initial and final assessment performance scores for study subjects (intervention and control group) rega
*significant at 5% level. Table 10: Overall mean of initial and final assessment performance scores for study subjects (intervention and control group) regarding prevention of VAP (n=120).
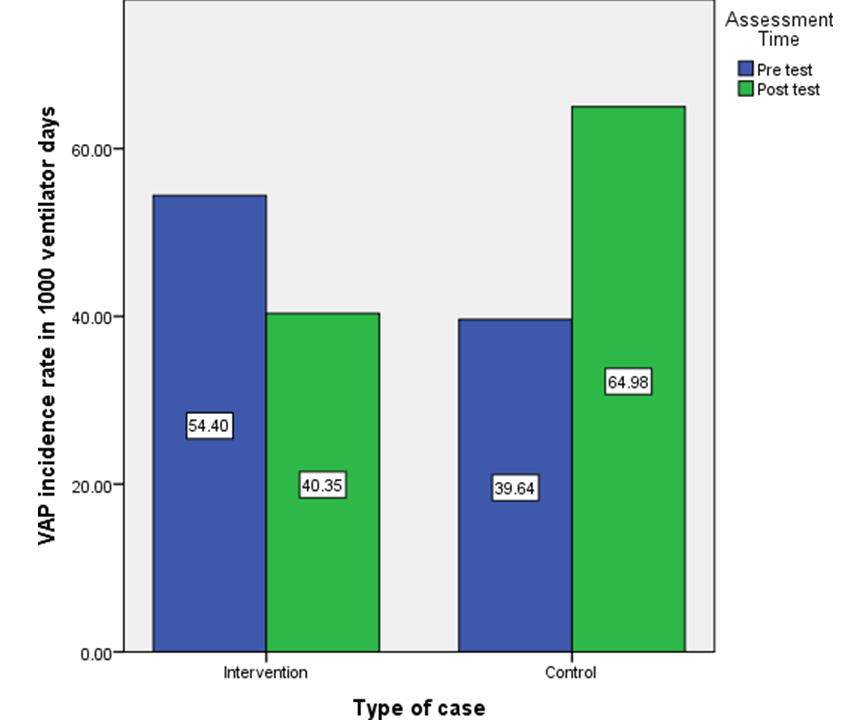
Section IV: Effects of Educational Program in VAP Incidence The VAP incidence rate for intervention group was (54.4/1000 ventilator days) in pre intervention assessment and the rate decreased to (40.53/1000 ventilator days) in post intervention assessment, which reflects the positive impact of education program in decreasing the VAP incidence rate. But for the control group, the VAP incidence rate was (39.6/1000 ventilator days) in initial assessment and became(64.9/1000 ventilator days) in final assessment (Figure 1).
Discussion
This study aimed to evaluate the impact of a structured teaching program on ICU nurses knowledge and practice compliance regarding VAP prevention. Even though there is an extensive body of literature on VAP prevention and protocols, there is paucity of studies focusing on the impact of structured teaching program on increasing knowledge and improving clinical practice for VAP prevention. Moreover, this is the first study addressing this problem in Sudan.
A quasi-experimental study with comparison groups (intervention and control) design, the pre and post-test structured questionnaire was designed to evaluate the knowledge, observation check list to evaluate practice compliance of 120 nurses’ staff regarding prevention of VAP and Patient ICU sheet to calculate the VAP incidence rate.The pre-test and initial assessment followed by implementation of structured teaching program (STP) and post-test and final assessment was conducted after 2 weeks from end STP to evaluate the effectiveness of structured teaching program.
Baseline Assessment of Nurses’ Knowledge and Practice Compliance Regarding Prevention of VAP.
Baseline Knowledge Assessment: The present study confirmed that; the overall mean of pre-test knowledge for the intervention group is (17.95 out of 40) and (18.50 out of 40) for the control group, which is less than 50% of max. score for both groups and revealed that the two groups were comparable in knowledge before intervention (p=0.617>0.05) (table 4-3). The majority of participants(60.0% and 68.3) had inadequate knowledge level (< 20 correct answers), (40.0% and 31.7%) had moderate knowledge level (20-30 correct answers) for the intervention and the control group respectively, and no one of them had adequate knowledge (>30 correct answers) (table 4-5).
These findings are in line with those reported by Modather Osman (2014), who conducted a descriptive study in Sudan in order to assess the nurses’ knowledge and practice regarding application of international guidelines for VAP prevention in majority governmental hospital in Khartoum state. According to the author; the mean of total knowledge for participants was (8.5 out of 20) [19].
These findings also are agreeable with the results of a descriptive study conducted by Vivana Gomes in South Africa (2010) in order to determine the knowledge of nurses’ working in ICU with respect of evidence guidelines for VAP prevention. Her study revealed that; the knowledge of ICU nurses lacking in the evidence guidelines for VAP prevention; where only (21.6%) of participants achieved a pass mark considered to have adequate knowledge level and (78.4%) ofthem didn’t achieved a pass mark and are considered to have inadequate knowledge level and the mean scores of participants knowledge was (4.25±2.37) (11).Another descriptive study conducted by Nahla Ali in Egypt (2013) to assess the critical care nurses’ knowledge and compliance with VAP prevention bundles, revealed that; the participants had unsatisfactory knowledge score (mean=7.46±2.37 out of 20 scores) [20]. Base Line Practice Compliance: The present study confirmed that; the overall mean of initial practice compliance assessment for intervention group was (9.27±2.80 out of 20) and (4.97±2.15 out of 20) for control group with statically significant difference between the two groups (p=0.000<0.05) but this difference not great in the value where the both groups had mean of <50% of the max. Score and didn’t mean much in practical terms, which indicates that there was poor practice compliance of nurses regarding VAP prevention.
These findings are confirmed with Nahla Ali found in her study in Egypt (2013) which revealed that; most of nurses were not compliant with VAP prevention bundle practice (average mean=8.62±7.9 out of 29) [20]. Also it similar with Modather Osman study which conducted in majority of governmental hospitals in Khartoum state, Sudan (2014) and the study found that; (42%) of subjects had poor practice compliance (19).
On the other hand the results of the study conducted by Mujahed Alkhadir in Sudan (2013) differ from the finding of this study, which revealed that; (42.5%) of participants had fair practice level, (32.5%) poor practice and (2.5%) of them had good practice).
Evaluation of the effectiveness of Structured Teaching Program
In knowledge: The present study confirmed that; there was a considerable improvement of knowledge after the application of the Structured Teaching Program and it’s statistically established significant.The overall mean knowledge scores in the pre-test for intervention group was (17.95 out of 40) and (32.05 out of 40) in post-test with 14.1 mean knowledge enhancement (Tables 4-6). This indicates that, education program leads to increase in knowledge which impacted on prevention of VAP.
These findings are in line with those reported by ShilpaRao in India (2013) in order to evaluate the effectiveness of structured education program on knowledge among PICU nursesregarding prevention of VAP. Results of this study revealed that; the overall pre-test mean knowledge scores of PICU was found to be (14.4 out of 40) and (33.76 out of 40) in post-test with 19.36 enhancement in mean knowledge scores [22].
These findings also in agreement with the results of study conducted by Ennis Musvosvi in U.S.A. (2013) in order to examine nurses’ knowledge and compliance with ventilator bundle elements before and after in-service education. Found that; the nurses, who had room for improvement, had a mean score increase of 1.33 in knowledge post-test from pre-test [23]. Another study conducted in Pakistan (2011) by Motherly, to investigate the impact of 5- hours teaching module on nurses’ knowledge to practice evidence based guidelines for the prevention of VAP. The study revealed that knowledge scores of participants increased significantly after the education intervention in the first post-test [24]. In Practice Compliance: The present study confirmed that; there was a considerable improvement of practice compliance after the application of the Structured Teaching Program and it established as a significant statistically. The overall mean practice scores in initial assessment was (9.27±2.8) and (12.77±2.3) in final assessment with (3.5) mean practice enhancement (table 4-10). This indicates that educational program leads to increased practice compliance which has an impact on prevention of VAP.
That resembles the results of Ennis Musvasi study (2013) in U.S.A., which found that; nurses that had room for improvement, had a mean score increase of 4.3% on practice compliance with ventilator bundles elements among the intervention group after education program [23]. Another study conducted in Spain by Gatell Rose, et al. in order to assess the effectiveness of training program on nurses knowledge of VAP, compliance with VAP preventive measures, VAP incidence and determining wither nursing workload affect compliance concluded that; the program improved both knowledge and compliance with VAP preventive measures [25].
Furthermore the present study revealed that; all participants in both study groups (intervention and control) didn’t perform the following (wear clean gloves with closed suction system, continuous aspiration of subglottic secretion) (Tables 4-8) because the closed suction system and subglottic endotracheal tube wasn’t available in the Sudan at all governmental and private hospital, also checking the gastric residual volume every 4-6hrs wasn’t performed by allthe participants, because they believe the presence of ET tube in patient with mechanical ventilation is enough to prevent the aspiration.
These findings confirmed by Nahla Ali study in Egypt (2013) that explored the closed suction, subglottic suction extubation and weaning trials and peptic ulcer prophylaxes practice were not done by nurses [20].
In VAP incidence rate: The VAP incidence rate is collected from patient ICU sheet (Appendix VIII) and calculated by dividing the numbers of VAPs by the number of Ventilator days and multiplying the results by 1000 [4]. In the three months period before the intervention (teaching program), 43 episodes of VAP (21 in intervention and 22 in control), were recorded in the total of 941 ventilator days (386 in intervention and 555 for control) among 66 patient on mechanical ventilation that meet the study inclusion criteria. This corresponded to the infection rate of 54.4 and 39.6 cases per 1000 ventilator days for the intervention and the control group respectively.
This finding is similar with those reported by study conducted in Turkey (2011), in order to assess economic burden of VAP in a developing country, which revealed that; VAP developed in 96 (60%) patient with 47.9/1000 ventilator days [26]. This findings also in agreement with the result of a systemic review study about; VAP in adults in developing countries, conducted by Arabi Y, et al. revealed that; in developing countries the rates of VAP vary from 10 to 41.7 cases per 1000 ventilator days [27].
In the two-month period Following the intervention (Teaching Program), 32 episodes of VAP (14 intervention and 18 control), were recorded in the total of 624 ventilator days (347 in intervention and 277 in control) among 47 patients on mechanical ventilation that meet the study inclusion criteria .This corresponded to the infection rate of 40.3 and 64.9 cases per 1000 ventilator days for the intervention group and the control group respectively (Figure 1).
These findings are in line with those reported by Reem AlSadat, et al. who conducted a similar study in Syria in order to assess use of VAP bundle and statistical process control chart to decrease VAP rate. According to authors; the pre-intervention VAP incidence rate was 39 cases per 1000 ventilator days and reduced to 6.4 cases per 1000 ventilator days post-intervention [28].
The findings of the present study confirm a considerable improvement on VAP incidence rate can be achieved by introducing evidence-based protocols. More specifically, in theintervention group the VAP incidence rate of 54.4 in the pre-intervention period decreased to 40.3 cases per 1000 ventilator days in the post-intervention phase. Thus, the teaching program was effective in reducing the VAP incidence rate.
This finding is also in agreement with the results of four years study conducted in Thailand by Anusha Apisarnthanarak, et al. to evaluate the effectiveness of an education program in reducing VAP in tertiary care center. The authors reported that; 45 episodes of VAP (20.6 cases per 1000 ventilator days) recorded before intervention decreased to (8.5 cases per 1000 ventilator days) following the intervention [29].
Conclusion
A quasi-experimental case-control study design, to evaluate the effectiveness of structured teaching program on knowledge and practice compliance regarding prevention of ventilator associated pneumonia among adult ICU nurses at selected hospitals, Khartoum. The data was collected from 120 subjects through purposive sampling technique. Further the conclusion was drawn on the basis of the findings of the study which includes:
- The overall mean of pre-test knowledge scores on prevention of VAP was found to be (17.95 out of 40) for intervention group and (18.50 out of 40) for control group.
- The overall mean of post-test knowledge scores on prevention of VAP was found to be (32.05 out of 40) for intervention group and (20.83 out of 40) for control group. Which indicates that; nurses in intervention group gained knowledge after teaching program was applied.
- The overall mean of initial assessment practice compliance scores on prevention of VAP was found to be (9.27 out of 20) for intervention group and (4.97 out of 20) for control group.
- The overall mean of final assessment practice compliance scores on prevention of VAP was found to be (12.77 out of 20) for intervention group and (5.7 out of 20) for control group. Which indicate that nurses in intervention group improve their practice compliance after administration of teaching program.
- The VAP incidence rate of pre intervention phase was found to be (54.4 cases/1000ventilator days) for intervention group and (40.35 cases/ 1000 ventilator days) for control group.
The VAP incidence rate of post intervention phase was found to be (39.6 cases/ 1000ventilator days) for intervention group and (64.9 cases/1000 ventilator days) for control group. Which indicate that; the VAP incidence rate for intervention group reduced after teaching program was implanted.
Acknowledgement
I would like to acknowledge nurses who participated in the study.
Ethics Approval
The following ethical requirements were taken into consideration during this study:
- The research proposal was submitted to the University Postgraduate Committee for permission to conduct the study moreover permission was obtained to ensure compliance with ethical standards.
- Ethical clearance and permission were taken from the ministry of health to conduct the study.
- Application for permission to conduct the study was be made to the management of all three hospitals included in the study.
- To ensure confidentiality and anonymity of the participants no names were recorded during data collection and reporting. Consent forms and questionnaires were separated at the time of data collection to maintain anonymity of participants.
Competing Interest
I confirm that I have no conflicts of interest related to the publication of this study. Availability of data and materials: All data and materials related to this study is available upon request from corresponding author.
References
-
Timsit JF, Zahar JR, Chevret S (2011) Attributable mortality of ventilator-associated pneumonia. Current opinion in critical care 17(5): 464-471.
-
Dellit TH, Owens RC, McGowan JE, Gerding DN, Weinstein RA, et al. (2007) Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clinical infectious diseases 44(2): 159-177.
-
Sedwick MB, Smith ML, Reeder SJ, Nardi J (2012) Using evidence-based practice to prevent ventilator - associated pneumonia. Critical care nurse 32(4): 41-51.
-
Dudeck MA, Horan TC, Peterson KD, Allen-Bridson K, Morrell G, et al. (2013) National Healthcare Safety Network report, data summary for 2011, device- associated module. American journal of infection control 41(4): 286-300.
-
Heyland DK, Cook DJ, Griffith L, Keenan SP, Brun-Buisson C (1999)The attributable morbidity and mortality of ventilator-associated pneumonia in the critically ill patient. American journal of respiratory and critical care medicine 159(4): 1249-1256.
-
Society AT, America IDS (2005) Guidelines for the management of adults with hospital acquired, ventilator- associated, and healthcare-associated pneumonia. American journal of respiratory and critical care medicine 171(4): 388-416.
-
Tejerina E, Frutos-Vivar F, Restrepo MI, Anzueto A, Abroug F, et al. (2006) Journal of critical care 21(1): 56- 65.
-
Luna CM, Blanzaco D, Niederman MS, Matarucco W, Baredes NC, et al. (2003) Resolution of ventilator- associated pneumonia: prospective evaluation of the clinical pulmonary infection score as an early clinical predictor of outcome. Critical care medicine 31(3): 676- 682.
-
Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, et al. (2002) Epidemiology and outcomes of ventilator- associated pneumonia in a large US database. Chest 122(6): 2115-2121.
-
Foglia E, Meier MD, Elward A (2007) Ventilator-associated pneumonia in neonatal and pediatric intensive care unit patients. Clinical microbiology reviews 20(3): 409-425.
-
Efrati S, Deutsch I, Antonelli M, Hockey PM, Rozenblum R,et al. (2010) Ventilator-associated pneumonia: current status and future recommendations. Journal of clinical monitoring and computing 24(2): 161-168.
-
Tablan OC, Anderson LJ, Besser R, Bridges C, Hajjeh R (2004) Guidelines for preventing health-care- associated pneumonia, 2003; recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. 53(3): 1-36.
-
Tolentino-DelosReyes AF, Ruppert SD, Shiao S-YPK (2007) Evidence-based practice: use of the ventilator bundle to prevent ventilator-associated pneumonia. American Journal of Critical Care 16(1): 20-27.
-
Gillespie R (2009) Prevention and management of ventilator-associated pneumonia–the Care Bundle approach. Southern African Journal of Critical Care 25(2).
-
Welch S, Austin C (2008) Development of an ICU preceptor program based on the AACN Synergy Model for Patient Care. Critical care nurse 28(2): e6.
-
Lawrence P, Fulbrook P (2011) The ventilator care bundle and its impact on ventilator‐associatedpneumonia: a review of the evidence. Nursing in Critical Care 16(5): 222-234.
-
Augustyn B (2007) Ventilator-associated pneumonia: risk factors and prevention. Critical care nurse 27(4): 32-39.
-
Labeau S, Vandijck D, Rello J, Adam S, Rosa A, et al. (2008) Evidence-based guidelines for the prevention of ventilator-associated pneumonia: results of a knowledge test among European intensive care nurses. Journal of Hospital Infection 70(2): 180-185.
-
Osman MOH (2014) Nurses Knowledge and Practice regard the Application of International Guidelines for Prevention of Ventilator Associated Pneumonia. Nursing sciences, Al-Neelin Sudan, pp: 99.
-
Ali NS (2013) Critical Care Nurses’ knowledge and compliance with ventilator associated pneumonia bundle at Cairo university hospitals. Crit Care 4(15): 66-
-
Alshameri FA (2013) A Thesis submitted in fulfillment of the requirement for the Award of the Degree of Doctor of Philosophy in Medical-Surgical Nursing By. University of Khartoum.
-
Rao SN (2013) A Study to Evaluate the Effectiveness of Structured Teaching Programme on Knowledge Regarding Prevention of Ventilator Associated Pneumonia Among Paediatric Intensive Care Unit Nurses at Selected Hospitals, Bengaluru.
-
Musvosvi E (2013) The impact of in-service education on ICU nurses’ knowledge and compliance with practices for preventing ventilator-associated pneumonia.
-
Meherali Sm, Parpio Y, Ali Ts, Javed F (2011) Nurses’ knowledge of Evidence-Based Guidelines For Prevention of Ventilator-Associated Pneumonia in Critical Care Areas: A Pre and Post Test Design. Journal of Ayub Medical College Abbottabad 23(1): 146-149.
-
Gatell MRJ, Roig MS, Vian OH, Santin EC, Duaso CT, et al. (2012) Assessment of a training programme for the prevention of ventilator‐associated pneumonia. Nursing in Critical Care 17(6): 285-292.
-
Alp E, Kalin G, Coskun R, Sungur M, Guven M, et al. (2012) Economic burden of ventilator-associated pneumonia in a developing country. Journal of Hospital Infection 81(2): 128-130.
-
Arabi Y, Al-Shirawi N, Memish Z, Anzueto A (2008) Ventilator-associated pneumonia in adults in developing countries: a systematic review. International journal of infectious diseases 12(5): 505-512.
-
Alsadat R, Al-Bardan H, Mazloum MN, Shamah AA, Eltayeb MFE, et al. (2012) Use of ventilator associated pneumonia bundle and statistical process control chart to decrease VAP rate in Syria. Avicenna journal of medicine 2(4): 79-83.
-
Apisarnthanarak A, Pinitchai U, Thongphubeth K, Yuekyen C, Warren DK, et al. (2007) Effectiveness of an educational program to reduce ventilator-associated pneumonia in a tertiary care center in Thailand: a 4-year study. Clinical infectious diseases 45(6): 704-711.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City