Endometriosis Mimicking Ovarian Malignancy: Diagnostic Dilemma of Three Cases
Ovarian endometriosis is an estrogen dependent gynecologic disease commonly affecting reproductive age group and 2-5% of postmenopausal women. Widespread endometriosis may be misdiagnosed as metastatic ovarian malignancy by imaging especially when coupled with increased levels of CA125. Present study reviews three such cases highlighting the need for high index of clinical suspicion in the correct case scenario. The clinicians should be aware of this mimicker as misdiagnosis has potential to distort the course of disease and may lead to unnecessary radical surgery in patients.
Introduction
Endometriosis is a benign estrogen dependent progressive disease characterized by endometrium-like tissue outside the uterus and usually affects patients in reproductive age group and 2-5% of postmenopausal women [1, 2]. Widespread endometriosis may mimic malignancy clinically like advanced ovarian or colorectal carcinomas or carcinomatous peritonea. Differential diagnosis is more difficult in peri as well as menopausal women or patients without typical features of endometriosis like infertility and dysmenorrhea. Imaging techniques are also not always effective in establishing correct diagnosis preoperatively. Moreover, problem is confounded by elevated cancer antigen 125 (CA125) levels (at times, 100 folds) and ovarian endometriosis (being a risk factor for malignant transformation). Widespread endometriosis may be misdiagnosed as metastatic ovarian malignancy by imaging especially when coupled with increased levels of CA125. Present study reviews three such cases highlighting the need for high index of clinical suspicion in the correct case scenario. Review of existing literature was based on pathogenesis and cases of ovarian endometriosis spreading in a manner similar to ovarian malignancy.
Case Summaries
Case 1
A 39 years female, P2L2A1, was hospitalized for pain in abdomen with the history of regular cycles & passage of blood clots. Past medical and family history was non-significant. Physical examination revealed pallor and umbilical hernia. Pelvic sonogram showed large multicystic lesion measuring 9.2 x 6.1 x 9.6 cm (volume 286 cc) in right ovary. CECT scan revealed well marginated, multiseptated cystic right ovarian mass closely abutting right posterolateral aspect of uterus and right lateral wall of recto sigmoid colon; suggestive of Neoplastic lesion (O-RADS 5 category). Serum CA125 was elevated (369.96 IU/ml); however CEA and CA19-9 levels were within normal range.
Exploratory staging laparotomy was performed and peroperatively right adnexal mass with capsular breach, adhesions in pouch of douglas (POD), right pelvic peritoneum and rectal wall was noted. Total abdominal hysterectomy with bilateral salpigo-oophorectomy (TAH+BSO), omentectomy, POD and right pelvic peritonectomy specimen was sent for histopathology with clinical diagnosis of Advanced ovarian cancer with peritoneal involvement. Grossly, right cystic ovary measuring 5x3.5x2 cm. with ruptured capsule, right para-ovarian nodule measuring 2.5x1.5x1.5 cm., dilated right fallopian tube and multiple grey white nodules (largest measuring 5.5x3.5x3 cm.) in peritoneal tissue were noticed. Peritoneal wash smears revealed very occasional atypical cells? Reactive?? Neoplastic. Histopathological diagnosis of right adnexal endometrioma with peritoneal endometriosis and adenomyosis was confirmed (Figures 1A & B).
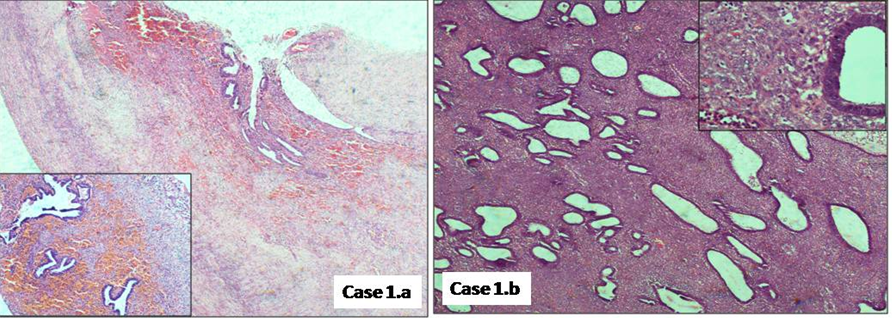
Figures 1A & B: A: Ovarian parenchyma showing presence of endometrial glands with surrounding hemorrhage & B: Nodular peritoneal deposits showing endometrial glands with stroma.
Case 2
A 34 years female, P2L2A3, was admitted with pain in abdomen, dysmenorrhoea and ascitis. Per vaginal examination revealed an ill defined mass in pelvis (size could not be determined), with restricted mobility? Carcinoma ovary?? Metastasis. CECT abdomen showed heterogeneous contrast enhancing multiloculated pelvic solid-cystic lesion measuring 10x10.8x8.5 cm.? Ovarian origin with surrounding omentomesenteric fat thickening and abutting bowel loops? infiltration. Raised CA125 (552 IU/ml) and CA19-9 (350.13 U/ml) levels were observed, while serum AFP, β-HCG and LDH levels were within normal limits. Clinical diagnosis of abdominopelvic mass malignancy was considered. USG guided FNAC and biopsy from the mass as well as ascitic fluid cytology were reported negative for malignancy.
Staging laparotomy followed by TAH + BSO with infracolic omentectomy was performed and sent for histopathology. Peritoneal fluid & frozen section were negative for malignancy. Grossly, right unilocular ovarian cyst measuring 11x9x1 cm. (already cut open) with hemorrhagic inner surface was noticed. Left ovary measuring 4x3x1.5 cm. with ruptured capsule and cut surface exhibiting hemorrhagic cyst measuring 1x1 cm. was observed. Omentum showed multiple hemorrhagic foci and focal thickening, however, no nodular or grey white deposits were seen grossly. Histopathological diagnosis of bilateral ovarian endometriosis with omental endometriosis was rendered (Figures 2A & B).
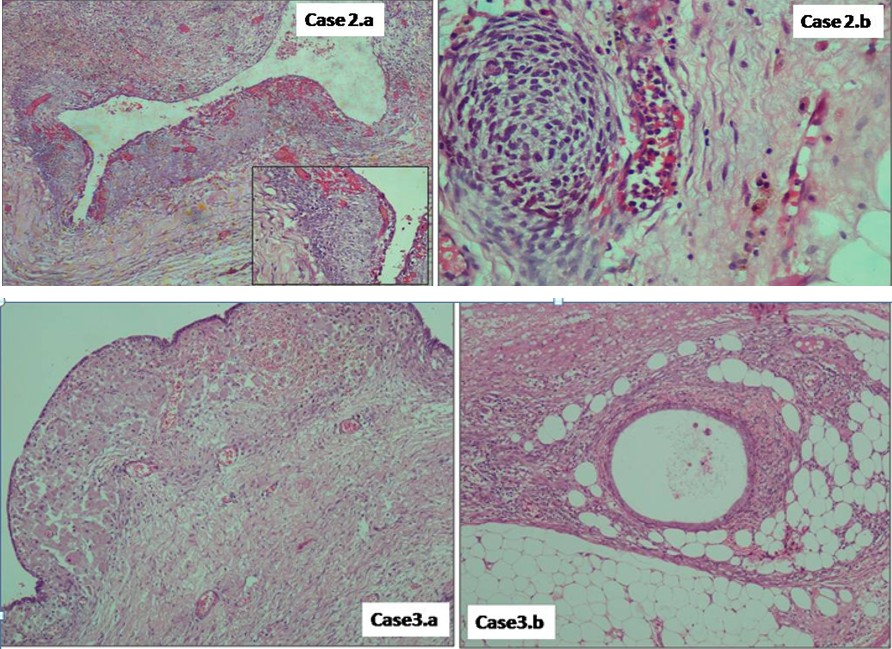
Figures 2A & B: A: Ovarian cyst showing endometrial type epithelial lining with surrounding endometrial type stroma & hemorrhage, B: Omental thickened areas showing focal presence of endometrial stroma.
Case 3
A 39 years female, P2L2, presented with complaints of pain in abdomen, backache, dysmenorrhea & heavy menstrual bleeding. Per-vaginally, a cystic structure measuring 5x6 cm. in right fornix and puckering in posterior fornix adhesions were felt. USG revealed right adnexal complex cystic-solid mass (10.8x8x6 cm.) exhibiting mixed echoic appearance, normal left ovary and thickened endometrium (approximately 15 mm endometrial polyp). Serum CA125 (369.96 IU/ml), CEA (5.41ng/ml) and LDH (190 U/L) levels were elevated. Clinical diagnosis of right complex adnexal mass with endometrial polyp was considered.
Hysteroscopic polypectomy followed by staging laparotomy, TAH + BSO and ometectomy was done in view of peroperatve suspicion of bilateral deep infiltrating endometriosis. Grossly, already cut open bilateral ovaries showed hemorrhagic cysts measuring 3 cm. (right ovary) and 1.5 cm. (left ovary) in maximum diameter. Histopathology confirmed the diagnosis of bilateral ovarian endometriosis with omental endometriosis. Separately lying polypectomy tissue bits were consistent with endometrial polyp (Figures 3A & B).
Figures 3A & B: A: Ovarian cyst wall showing endometrial type epithelial lining with adjacent hemorrhage & pigment laden macrophages, B: Omental tissue showing presence of benign looking endometrial glands with scant stroma & histiocytes.
Discussion
Ovarian endometrioma is a gynecologic disease common presentation in child bearing age group and undergoes changes with every menstrual cycle as well as during pregnancy giving variable macroscopic lesions. Smaller black puckered ‘‘powder burn’’ superficial peritoneal lesions to non-pigmented lesions to deep endometriotic lesions (deeper than 5 mm under the peritoneum, generally more than 1 cm in size, with frequent invasion into bowel wall or neurotropic effect or lymph node involvement) may be associated with ovarian endometriosis. Initially, fresh lesions are predominantly hemorrhagic but with repeated cyclic changes, lesions become more grey white to fibrotic which may mimic peritoneal tumor deposits in chronic disease [3, 4]. Frequently symptomatic patients present with chronic abdominal pain, pelvic infections, infertility, abdominal distension or mass. Limited data is available to prove the association of endometriosis to adenomyosis [3]. Generally, endometriosis is confined to pelvis, but may occur rarely in remote sites like abdominal wall, lung or gastrointestinal tract.
Due to lack of nonhuman model or experimentation, natural history and pathogenesis of endometriosis is not clearly defined, however, a few hypotheses have been suggested. Two most explained ones are implantation theory whether by endometrial cell reflux or retrograde menstruation and coelomic metaplasia theory giving rise to endometriosis via ovarian surface mesothelial cells [2, 3, 5]. Other possible quoted theories include embryonic rest theory and endometrial stem cells migration during embryogenesis. Not a single theory can explain the pathophysiology of endometriosis in all the cases. At the level of molecular mechanism, the genetic / epigenetic theory has been postulated for the development of endometriotic lesions even in unexplained cases. An emerging concept suggested that dysregulation of micro RNA expression may be important in the development of endometriosis. In short, several factors including genetic, epigenetic factors, local microenvironment, immunology, hormones and biomarkers play a key role in the development and progression of endometriosis [5, 6].
Some studies demonstrated that somatic mutations or genetic aberrations in KRAS, P53, PTEN and ARID1A gene regions contributed in the development of endometriosis associated ovarian cancer (EAOC). However, quantitative risk of malignant transformation is controversial. Two pathways have been suggested to understand: firstly, both diseases may coexist due to result of shared risk factors; and secondly, endometriotic cells may transform into malignant cells. Atypical endometriosis may be an intermediate step in progression from benign to malignant course. Another fact is that presence of abundant free iron in endometriotic cysts leads to persistent oxidative stress and subsequent carcinogenesis [5, 6].
New reliable biomarkers are needed for early detection of EAOC. An observation in one study was found that combined use of serum Smac, human epididymis protein 4 (HE4), and CA125 may be of clinical relevance in detection of EAOC [7].
In many instances, unfortunately elevated CA125 alone does not help, infact increased levels may add to clinical suspicion and cause diagnostic dilemma. Levels can be very high during or around menstruation. However, monitoring by serial assay with decreased levels is an important indicator of endometriosis as opposed to endometrioid carcinoma.
Similar to our described cases, Pang et al. discussed a 40 years old patient with ascites, pelvic mass, multiple nodules over fundus of uterus and elevated serum CA-125 levels. With the impression of advanced-stage ovarian cancer with massive ascites, surgical approach was continued and histopathology confirmed the diagnosis of endometriosis [8]. One author observed a suspicious intra-abdominal mass in 31 years old woman with elevated CA125 levels and history of lumbar irradiation which later found to be consistent with endometriosis histomorphologically [9]. Zwierzchowska, et al. and Zutshi V, et al. reported two cases of ovarian endometriomas in postmenopausal women with a solid to cystic adnexal lesions and suspected ovarian malignancy on imaging which later confirmed to be an endometrioma. CA125 levels were elevated one of these two cases [1, 2].
Polypoid endometriosis is a rare type of endometriosis forming polypoid masses mimiking a neoplasm on clinical, intraoperative, and gross pathological examinations. Ji- Young Kim, et al. described a case of multifocal polypoid endometriosis in a 30 years old G0P0 woman with a history of left adnexal mass on USG, gonadotrophin releasing hormone (GnRH) agonist and combined oral contraceptive (OC) intake [10]. Cleo Tsai, et al. discussed a case of polypoid endometriosis in young female presented with irregular shaped, heterogeneous mass at the cul-de-sac and an elevated CA-125 value (1317 U/ml) [11]. Lee, et al. also presented a rare case of ovarian polypoid endometriosis in a 32-year- old woman with bilateral ovarian masses, a highly elevated serum CA-125 level, ascites, peritoneal dissemination, and rectosigmoid involvement with clinicradiological suspicion of ovarian malignancy [12].
Some investigators reported uncommon presentations of endometriosis like 30 year old nullipara, with an umbilical nodule (Sister Mary Joseph’s) and pelvic tumor or cases of decidualised ovarian endometrioma in antenatal patients mimicking ovarian malignancy [13, 14].
Conclusion
Despite being a benign disease, in most advanced cases of endometriosis, pattern of its spread may resemble a neoplastic process. Imaging techniques and elevated CA125 levels are not always effective to confirm ovarian malignancy preoperatively. The clinicians should be aware of this mimicker as misdiagnosis has potential to distort the course of disease and may lead to unnecessary radical surgery in these patients particularly in child bearing age group.
References
-
Zwierzchowska A, Pane G, Gajewska M, Barcz E (2017) Endometriotic lesions mimicking advanced ovarian cancer - A case report and a review of the literature. Eur J Gynaecol Oncol 38(2): 303-307.
-
Zutshi V, Gupta S, Ahluwalia C, Monica R (2021) Endometrioma mimicking ovarian malignancy in a post- menopausal woman. Int J Reprod Contracept Obstet Gynecol 10(8): 3226-3228.
-
Koninckx PR, Ussia A, AdamyanL, Wattiez A, Gomel V, et al. (2019) Pathogenesis of endometriosis: the genetic/ epigenetic theory. Fertility and Sterility 111(2): 327-340.
-
Gałczyński K, Jóźwik M, Lewkowicz D, Semczuk-Sikora A, Semczuk A (2019) Ovarian endometrioma – a possible finding in adolescent girls and young women: a mini- review. J Ovarian Res 12:1-8.
-
Mikhaleva LM, Davydov AI, Patsap OI, Mikhaylenko EV, Nikolenko VN, et al. (2020) Malignant Transformation and Associated Biomarkers of Ovarian Endometriosis: A Narrative Review. Adv Ther 37(6): 2580-2603.
-
Králíčková M, Laganà AS, Ghezzi F, Vetvicka V (2019) Endometriosis and risk of ovarian cancer: what do we know?. Arch of Gynecol Obstet 301(1): 1-10.
-
Xu XR, Wang X, Zhang H, Liu MY, Chen Q (2018) The clinical significance of the combined detection of serum Smac, HE4 and CA125 in endometriosis-associated ovarian cancer. Cancer Biomark 21(2): 471-477.
-
Pang L, Shi H, Wang T, Zhu L, Lang J, et al. (2019) Endometriosis on the surface of the uterusmimicking a malignant tumor a case report with literature review. Medicine 98(21):e15741.
-
Reis-de-Carvalho C, Castro C, Osório F (2021) Unusual endometriosis mimicking disseminatedcancer after hysterectomy in a young woman. BMJ Case Rep 14(1):e241002.
-
Kim JY, Song TJ, Choi HK, Shim JY (2015) Multifocal Polypoid Endometriosis Mimicking Malignancy in a Young Woman with a History of Hormonal Treatment. J Pathol Transl Med 49(5): 418-420.
-
Tsai C, Huang SH, Huang CY (2019) Polypoid endometriosis - A rare entity of endometriosis mimicking ovarian cancer. Taiwanese Journal of Obstetrics & Gynecology 58(3): 328-329.
-
Lee NK, Byung BS, Choi KU, Song YJ, Suh DS, et al. (2018) Polypoid endometriosis of the ovary mimicking advanced ovarian carcinoma with extensive peritoneal metastases. Int J Clin Exp Med 11(4): 4279-4284.
-
ImaraluJO, Ajani MA, Adesina MA, Ojo NK (2019) Endometriosis Misdiagnosed as a Metastatic Ovarian Tumour. Case reports in Clinical Medicine 8(7): 189-195.
-
Wong L, BotolahyV, Carteret T, Marty M, Brun JL (2015) Decidualized Ovarian Mass Mimicking Malignancy. Case Reports in Obstetrics and Gynecology 2015: Article ID 217367, 4 pages.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City