Assessing the Diagnostic Role of Multidetector Computed Tomography in Bronchogenic Carcinoma: Histopathological Correlation and Clinical Insights
Background: Lung cancer is a global health issue, and Multi Detector Row Computed Tomography (MDCT) plays a crucial role in diagnosing and staging bronchogenic carcinoma. Purpose: To document bronchogenic carcinoma’s MDCT features and assess CT scan accuracy compared to histopathological diagnosis. Materials and Methods: Between June 2020 and November 2021, 70 patients with suspected bronchogenic carcinoma underwent clinical assessment and 128-slice MDCT scans from lung apices to upper abdomen, including adrenal glands. MDCT findings were compared to histopathological examination. Statistical analysis using SPSS 16 and Excel determined CT’s positive predictive value against histopathological diagnosis as the reference standard. Results: Out of the 70 patients, 41% were female, and 59% were male. Among those with suspected bronchogenic carcinoma in CT, 86% were confirmed as malignant through histological analysis. The mean age of patients with bronchogenic carcinoma was 61.5 years. Squamous cell carcinoma (43%) was the most common histological subtype, followed by adenocarcinoma (38%). There was a notable male predominance (68%) for bronchogenic carcinoma, with distinct patterns observed for different histological subtypes. MDCT exhibited an 86% positive predictive value in diagnosing bronchogenic carcinoma compared to histopathology. Conclusion: Squamous cell carcinoma emerged as the most prevalent subtype of bronchogenic carcinoma, with MDCT demonstrating high diagnostic accuracy. The study advocates for routine MDCT utilization in the diagnosis and staging of bronchogenic carcinoma. Consider limitations like absent interobserver variation and challenges in distinguishing reactive hyperplasia from metastatic lymphadenopathy. Future research could explore potential implications and applications of the study’s findings.
Introduction
Before 1900 AD, lung cancers were considered medical curiosities with no known medical influence and deemed too rare for practical significance [1]. However, in the modern era, bronchogenic carcinoma has become a prevalent global malignancy, surpassing colorectal, breast, and prostate cancers combined in mortality [2]. This surge is closely tied to widespread cigarette smoking. Lung cancer has emerged as a prominent cause of cancer-related mortality, particularly in developing nations like Nepal [3, 4]. Limited global cancer registries hamper understanding of lung cancer’s true burden, forcing reliance on mortality data due to high fatality rates and consistent survival rates, creating a strong association between mortality and incidence data. This displays the need for the generation of country-based evidence [5].
The early prevention and detection of lung cancer represent a critical public health priority. Imaging techniques are central to its effective management. Although plain radiography is the first step, it falls short in providing the level of detail required for comprehensive assessment. Multi- Detector Computed Tomography (MDCT) has now emerged as the preferred imaging modality for the evaluation of bronchogenic carcinoma. It offers superior spatial resolution, multiplanar imaging capabilities, and precise staging, all of which are indispensable for prognosis [6].
MDCT’s advantages include shorter scan times, greater anatomical coverage in a single breath-hold, patient comfort, and excellent 3D reconstructions. Faster imaging improves contrast enhancement and reduces examination costs [6]. While CT features can suggest some subtypes of bronchogenic carcinoma, histopathological correlation is crucial for definitive diagnosis and prognosis assessment.
Chest ultrasound, with neck screening for metastatic lymphadenopathy, aids lung cancer diagnosis and is valuable for guiding peripheral tumor biopsies and pleural fluid aspirations. However, it’s less suitable for central tumors. MRI is useful for certain bronchogenic carcinomas, such as superior sulcus tumors, and excels in assessing chest wall, pericardial, and diaphragmatic involvement but lags behind CT in evaluating lung parenchymal changes [7].
Positron Emission Tomography-Computed Tomography (PET-CT), with recent advances, plays a role in staging advanced lung cancer and pre-surgical planning for respectable cases. Even when imaging strongly suggests malignancy, tissue diagnosis, and staging remain essential for optimal treatment. Histological confirmation of metastasis is critical for guiding therapy [8].
This study aims to assess bronchogenic carcinoma’s imaging characteristics using MDCT and determine its diagnostic accuracy. In the Nepalese context, limited research has explored the correlation between MDCT findings and histopathological results, which, if strong, could support non-invasive diagnostic approaches.
Material and Methods
This retrospective observational analytical study involved 70 patients with suspected primary lung cancer based on clinical and radiological assessments. It was conducted at the Department of Radiology and Imaging in a Tertiary care center, spanning from June 2020 to November 2021. Ethical clearance was granted by the Institutional Review Committee of the Institute of Medicine, with reference number 79/ (6-11) E2/077/078. The work is reported in line with the Standard for Reporting of Diagnostic Accuracy Studies (STARD) [9]. The study is registered retrospectively in the research registry.
Sample size
A sample size of 65 was calculated using the sensitivity formula with a confidence level of 90%, a level of significance of 10%, the sensitivity of the test being 96% [10] and a reasonable estimate of key proportions to be measured in the study was 16%(3). The study was done in 70 patients (Figure 1).
Inclusion and Exclusion Criteria
The inclusion criteria include patients suspected of having bronchogenic carcinoma and who underwent chest CT scans in the Department of Radiodiagnosis. Exclusion criteria include patients with contraindications for contrast studies, renal impairment, allergies to contrast media, previously diagnosed cases, unwilling consent recipients, and patients with no available histopathological reports.
Study variables include age, sex, smoking history, suspicious CT features of Bronchogenic carcinoma (size, location, margin, wall thickness, enhancement, calcification, and lung effusion), and histopathological examination (HPE) report of lung mass.
Data Collection
Patients underwent a 4-hour fasting period before the CT scan to minimize complications from contrast medium administration. Comprehensive risk information was provided, and informed consent was obtained. Scans, both plain and contrast-enhanced, were conducted using a Siemens Somatom Definition AS 128-slice MDCT machine, employing 120 KVp, 300 mAs, 5mm collimation sections, and retro reconstruction at 0.625mm thickness. Imaging encompassed lung apices to the upper abdomen, including the adrenals.
Sequentially, plain scans were followed by intravenous contrast scans during suspended inspiration. To achieve contrast enhancement, 70-80 ml of 350mg/ml non-ionic iodinated contrast was intravenously injected at a rate of 3-4ml/s, with sections captured after a 35-second venous phase delay.
Post-study retro reconstructions were performed at a 0.625 mm section thickness, with sagittal and coronal reconstructions added as needed. The scans were meticulously reviewed on a dedicated display console, utilizing a variety of window settings. Both pre-contrast and post-contrast images were subjected to a comprehensive analysis by a panel of experienced radiologists (Figures 2A & 2B).

Figure 2A: Non-contrast axial Computed Tomography of chest showing soft tissue density mass with irregular margin in left upper lobe with tiny foci of calcifications.
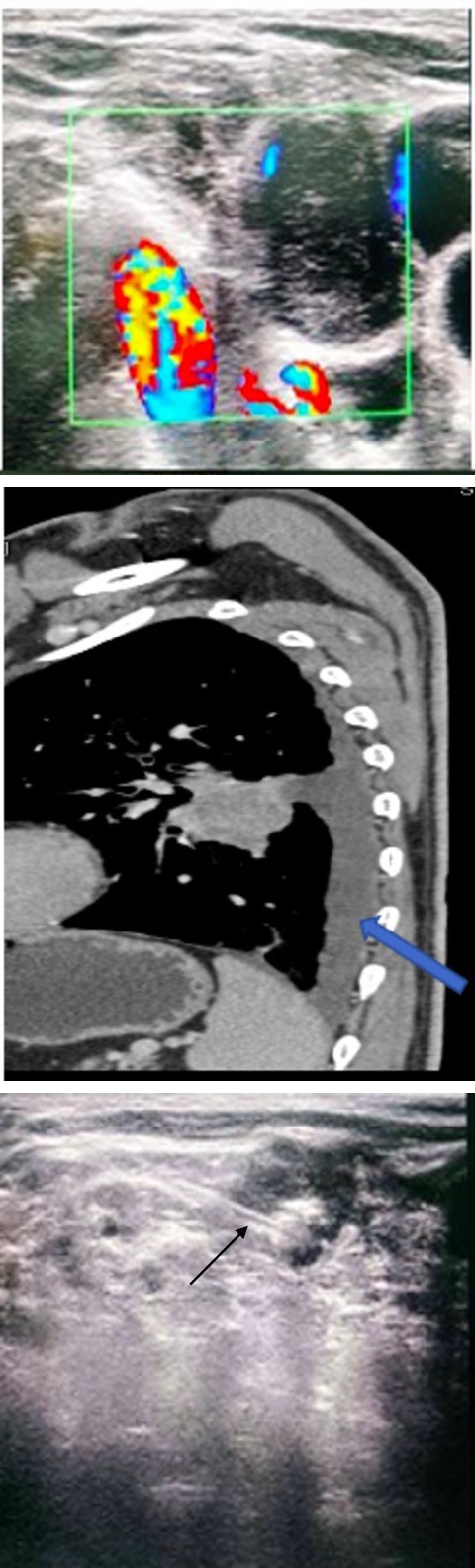
Figure 2B: Post-contrast sagittal Computed Tomography image of the chest showing enhancing soft tissue density mass in the left lung with moderate pleural effusion (purple arrow).
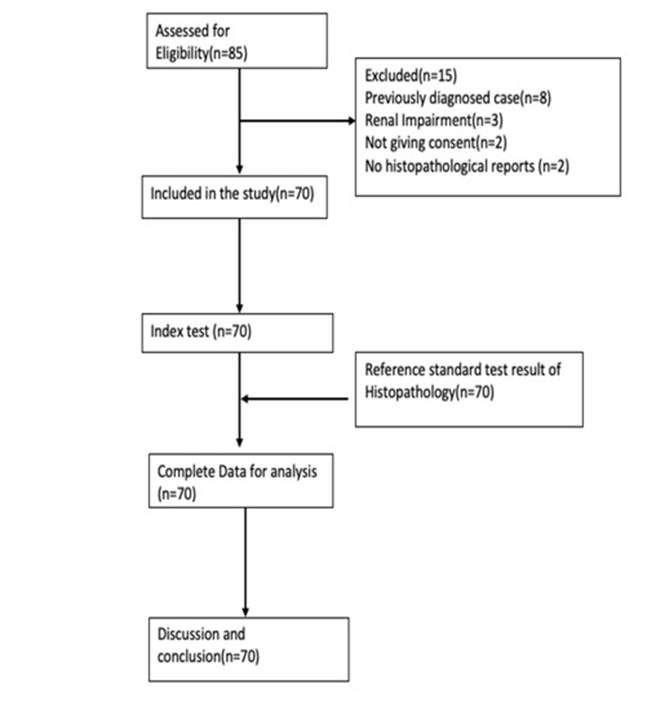
MDCT findings were systematically compared with histopathological analyses of tissue specimens obtained through fine-needle aspiration cytology (FNAC) or biopsies of chest masses and supraclavicular lymph nodes (Figures 3A & 3B). These procedures were conducted with the guidance of ultrasound or CT imaging, and the collected samples were subsequently sent for histopathological examination. To mitigate FNAC inaccuracy or inconclusiveness, we employed a 22G large-size needle for FNAC and incorporated real- time evaluation by experienced pathologists. In cases of inconclusive results, repeat FNAC procedures were conducted. Histopathology serves as the definitive, clinically pertinent, and exceptionally precise method for diagnosing bronchogenic carcinoma, establishing its role as the gold standard in cancer diagnosis. The histopathology reports were acquired through ongoing patient follow-up, with some directly retrieved from centralized laboratories within four tertiary care centers. Characteristics including cellular atypia, mitotic activity, necrosis, lymphovascular invasion, and the predominant histological pattern (solid or solid- cystic) underwent thorough assessment. These parameters were utilized for the grading of lung carcinoma and the subsequent classification into different histological types, all of which were documented in the histopathological report.
Figure 3A: Greyscale color Doppler image showing the enlarged supraclavicular lymph node with necrotic center and surrounding vascularity.
Figure 3B: Ultrasound-guided biopsy of the supraclavicular lymph node with the tip of the biopsy needle (black arrow).
Statistical Analysis
Data were collected in the predesigned Proforma and stored for further analysis. SPSS 16 was used to analyze the data. Microsoft Excel and Microsoft Word were used to make charts and tables. The cases with missing data were excluded from the analysis. Numerical variables were presented in tables and charts. Pearson’s correlation test was used to see the association between the categorical variables. A p-value of <0.05 was considered statistically significant.
Results
A study involving 70 patients suspected of lung carcinoma who underwent CECT chest and subsequent biopsy revealed a male predominance. Among these patients, 60 were histopathologically proven cases of bronchogenic carcinoma. Within this group, 65% were male, and 35% were female. The age distribution of patients with bronchogenic carcinoma ranged from 36 to 85 years, with a mean age of 61.5 years. The highest number of cases was observed in the age group of 61 to 70 years (27%) (Table 1).
| Characteristics | Number (%) | |
|---|---|---|
| Sex | Male | 41(59%) |
| Sex | Female | 29(41%) |
| Age | 31-40year | 2(3%) |
| Age | 41-50year | 12(20%) |
| Age | 51-60year | 13(22%) |
| Age | 61-70year | 16(27%) |
| Age | 71-80year | 10(17%) |
| Age | >81 | 7(11%) |
Table 1: Clinico-Demographic Profile of Patient of Bronchogenic carcinoma referred to Radiology Department.
In this study cough, and weight loss were the most common symptoms, while loss of appetite and dyspnea were the least common. Among 60 patients with bronchogenic carcinoma, 41 (68%) were smokers and 19 (32%) were non- smokers of the 23 adenocarcinomas, 56.5% were smokers, while 84.6% were smokers in 25 squamous cell carcinomas. Bronchogenic carcinoma was more common among smokers (p = 0.03).
All the cases of bronchogenic carcinoma showed significant (>20 HU) enhancement in post-contrast images. The study found that 57% of lesions were peripheral in location, while 43% were central in location. Central lesions included 58% adenocarcinomas, 31% squamous cell carcinomas, 8% small cell carcinomas, and 4% not categorizable malignancy. Periphery-situated lesions included 24% adenocarcinomas, 53% squamous cell carcinomas, 15% small cell carcinomas, 6% not fully categorized NSCLC, and 2% not categorizable malignancy. Out of 23 adenocarcinoma cases, 34.8% were peripheral, while 69% of 26 squamous cell carcinoma cases were peripheral. The percentage of peripheral location was significantly different in different carcinoma subtypes (p = 0.016).
Mediastinal and hilar lymphadenopathy was seen in 83 % of patients (n = 50) each, 48 % had supraclavicular lymph nodes (n = 29) and 2 % had peri bronchial lymph nodes (n = 1).Out of a total of 70 patients studied 60 patients had histologically proven bronchogenic carcinoma. Among 60 HPE-proven cases of bronchogenic carcinoma, the most common histological type was squamous cell carcinoma 44 % (n = 26), followed by adenocarcinoma 38% (n = 23). The least common histological subtype was not fully categorized NSCLC 3 % (n = 2). The remaining nine cases were inflammatory infiltrate or negative for malignancy.
The distribution of histopathological diagnoses based on gender demonstrated statistical significance (p=0.006) among various carcinoma subtypes. Adenocarcinoma exhibited a higher prevalence in males, while squamous cell carcinoma showed an equal prevalence in both males and females (Table 2).
| Adenocarcinoma (n=23) | % | Squamous cell carcinoma (n=26) | % | p | |
|---|---|---|---|---|---|
| Female | 3 | 13 | 13 | 50 | 0.006 |
| Male | 20 | 87 | 13 | 50 | 0.006 |
Table 2: Table Depicting Correlation between Gender distribution of Bronchogenic Carcinoma.
MDCT showed a positive predictive value of 86% in evaluating suspected cases of bronchogenic carcinoma, with a negative rate of 14% with histopathological correlation. The study of 60 HPE-proven bronchogenic carcinoma patients revealed that 10% had cavitating lesions, 37% had non-enhancing areas, and 42% had calcification in the CECT chest. Distant metastasis was present in 30% of cases, and satellite nodules were present in 32%. In our study, most of the malignancies had lobulated margins in 42 % (n = 25) of cases while spiculated margin was least commonly seen in 18% (n = 11) of cases. No adverse events were observed during the MDCT examination, as well as during the FNAC or biopsy procedures for mass assessment.
Discussion
Bronchogenic carcinoma is a major global cancer cause, with smoking being the most significant risk factor. It has a poor prognosis with a 5-year survival rate of 10-15% [11]. The incidence of lung cancer has increased, particularly in developing countries like Nepal. This study assessed demographic characteristics, clinical presentations, MDCT characteristics, and histological types of bronchogenic carcinoma.
Bronchogenic carcinoma is more common in individuals aged 61-70, with a slightly older age group compared to Rawat et al.’s 40-60 age groups [12]. The mean age of bronchogenic carcinoma in our study was 61.5-14.07 years, similar to Krishnamurthy A, et al. [13] 56-year mean age.
In this study, the prevalence of lung cancer was higher in males as compared to females with a ratio of M: F of 1.85:1. Higher prevalence among males was also seen in most of the other studies [13, 14], however, in our study percentage involvement of females was higher. In a study done by Al- Rahim YA [15] male: female ratio was 2.5: 1, which is similar to our study. In the study by Shetty CM, et al. [14], there was a very high male-to-female ratio of 12.5:1 (Table 3).
| Present study | Rawat J, et al. [12] | Krishnamurthy A, et al. [13] | Al-Rahim YA [15] | Shetty CM, et al. [14] | |
|---|---|---|---|---|---|
| Male | 65% | 89.20% | 77.50% | 71.80% | 92.50% |
| Female | 35% | 10.80% | 22.50% | 28.2% | 7.50% |
| M: F | 1.85:1 | 8.2:1 | 3.5:1 | 2.5:1 | 12.5:1 |
Table 3: Comparison of gender distribution between present study and other studies.
Smoking, the predominant etiological factor, likely contributed to the elevated occurrence of bronchogenic carcinoma. Notably, the incidence of lung cancer is on the rise among non-smokers too [13]. In our study, 32% of non-smokers were found to have bronchogenic carcinoma, aligning with Krishnamurthy A, et al. [13] findings where 52.7% of cancer cases occurred among non-smokers.
Several imaging modalities, including chest radiography, CT scan, positron emission tomography (PET) scan, and Magnetic Resonance Imaging (MRI), are used for staging various histological subtypes. Among these, radiography offers limited utility, while CT scan is the most widely employed imaging modality [16].
In our study, most malignancies were located peripherally (57%), while the remaining was in central locations (43%). Among the central lesions, 58% were adenocarcinomas, and
31% were squamous cell carcinomas. For the peripherally situated lesions, 53% were squamous cell carcinomas, and 24% were adenocarcinomas. These findings align with a study by Shetty CM, et el. [14], which showed adenocarcinoma as the central tumor in 70.5% and squamous cell carcinoma as the peripheral tumor in 52.7%. However, some studies indicate a higher prevalence of squamous cell carcinoma centrally.
In our study, 42 % of carcinomas showed lobulated contour which is contrary to the study done by Shetty CM, et al. [14] where 85 % of the malignancies had speculated margins and 70 % had lobulated margins. In our study calcification was found in 42% of the tumors which was seen predominantly in squamous cell carcinoma. This is in agreement with the study by Shetty CM, et al. [14] where calcifications were seen predominantly in squamous cell carcinoma in 46%.
| Present study | Kayastha P | Rawat J, et al. [12] | Krishnamurthy A, et al. [13] | Shetty CM, et al. [14] | |
|---|---|---|---|---|---|
| Squamous cell carcinoma | 43% | 20% | 44.80% | 15.60% | 44.40% |
| Adenocarcinoma | 38% | 42.50% | 19.70% | 42.60% | 18.50% |
| Small cell carcinoma | 12% | 10% | 16.75% | 13.20% | 17.20% |
| Large cell carcinoma | - | - | 8.30% | 2.30% | 9.80% |
| Not fully categorized NSCLC | 3% | 2.50% | - | - | - |
| Not categorizable malignancy | 3% | - | - | - | - |
Table 4: Comparison of various histopathological types of Bronchogenic carcinoma between present study and other studies.
All of our cases showed significant enhancement in post- contrast imaging which is concordant with the findings in the study by Shetty CM, et el. [14]. In our study, squamous cell carcinoma emerged as the predominant histological subtype, constituting approximately 43% of cases, followed by adenocarcinoma as the second most common subtype. These findings align with similar research by Rawat J, et al. [12], reporting squamous cell carcinoma in 44.8% of cases, and Shetty CM, et al. [14], where it was found in 44.4% of cases. Additionally, our study recorded small cell carcinoma in 12% of cases, with the absence of large cell carcinoma, corroborating findings from Kayastha P, which showed a 10% occurrence of small cell carcinoma and the absence of large cell carcinoma (Table 4).
In our study, the positive predictive value of MDCT for bronchogenic carcinoma diagnosis was 86%, which is notably lower than the findings of Meena DR, et al. [10] and Vinay C et al. [17], where MDCT demonstrated positive predictive values of 98% and 100%, respectively. This discrepancy may be attributed to the presence of 9 inflammatory lesions identified on biopsy in our study, accounting for 14% of cases.
The study had limitations, including the absence of interobserver variation and the potential for MDCT to provide a precise differentiation between reactive hyperplasia and metastatic mediastinal lymphadenopathy. These limitations should be considered when interpreting the findings and applying them in clinical contexts.
In conclusion, our study extensively assessed bronchogenic carcinoma using Multidetector Computed Tomography (MDCT) and correlated it with histopathological findings. Squamous cell carcinoma predominated, followed by adenocarcinoma. Notably, our results differed from similar studies, highlighting a higher occurrence of peripheral squamous carcinoma. Smoking showed a strong association with bronchogenic carcinoma, especially squamous cell carcinoma. MDCT exhibited a notably high positive predictive value, emphasizing its exceptional diagnostic accuracy in evaluating bronchogenic carcinoma. We recommend the routine use of MDCT for the diagnosis and staging of bronchogenic carcinoma.
Ethical Approval
We have conducted an ethical approval base on the Declaration of Helsinki with registration research at the Institutional Review Committee (IRC) of the Institute of Medicine (IOM), Tribhuvan University, Nepal Reference number: 79/ (6-11) E2/077/078.
Acknowledgment
I appreciate biostatisticians for their invaluable support in article submission, their expertise in statistical analysis and interpretation significantly improved research quality.
Author Contributions
Sharma Paudel: Conceptualization, as mentor and reviewer for this original article and for data interpretation, Bibek Nepal: Conceptualization and reviewer for this case, Prakash Kayastha: Reviewer and data interpretation, Sundar Suwal: Contributed in performing literature, Shailendra Katwal: Contributed in performing literature review and editing. All authors have read and approved the manuscript.
Declaration of Competing Interest
All the authors declare that they have no competing interest.
Funding
The authors declare that writing and publishing this manuscript was not funded by any organization.
References
-
Johnson DH (2007) PL3-01: Advances in Management of NSCLC-Advances in Chemotherapy. J Thorac Oncol 2(8): S145-S146.
-
Sung H, Ferlay J, Siegel RL, Laversanne M, Jemal A, et al. (2021) Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71(3): 209- 249.
-
Report P (2018) Population Based Cancer Registry in Nepal Cancer Registry Principal Investigator/ Co- Investigators.
-
Poudel KK, Huang Z, Neupane PR, Steel R, Poudel JK (2017) Hospital-Based Cancer Incidence in Nepal from 2010 to 2013. Nepal J Epidemiol 7(1): 659-665.
-
Didkowska J, Wojciechowska U, Manczuk M, Lobaszewski J (2016) Lung Cancer Epidemiology: Contemporary and Future Challenges Worldwide. Annl Transl Med 4(8): 150.
-
Das CJ, Seith A, Mukhopadhyay S (2007) Thoracic Application of Multi-Detector CT. Indian J Chest Dis Allied Sci 49(1): 29-36.
-
Hafez MR, Sobh ES, Elsawy SB, Abo-Elkheir OI (2017) The Usefulness of Thoracic Ultrasonography in Diagnosis and Staging of Bronchogenic Carcinoma. Ultrasound 25(4): 200-212.
-
Ahmed M, Flannery A, Daneshvar C, Breen D (2018) PET and Neck Ultrasound for the Detection of Cervical Lymphadenopathy in Patients with Lung Cancer and Mediastinal Lymphadenopathy. Respiration 96(2): 138- 143.
-
Cohen JF, Korevaar DA, Altman DG, Bruns DE, Gatsonis CA, et al. (2016) STARD 2015 Guidelines for Reporting Diagnostic Accuracy Studies: Explanation and Elaboration. BMJ Open 6(11): e012799.
-
Meena DR, Godara CS, Saxena S (2019) Role of Multi Detector Computed Tomography in Evaluation and Staging of Bronchogenic Carcinoma. IOSR Journals 18: 27-36.
-
Rosado-de-Christenson ML, Frazier AA, Stocker JT, Templeton PA (1993) From the Archives of the AFIP. Extralobar Sequestration: Radiologic-Pathologic Correlation. Radiographics 13(2): 425-441.
-
Rawat J, Sindhwani G, Gaur D, Dua R, Saini S (2009) Clinico- pathological Profile of Lung Cancer in Uttarakhand. Lung India 26(3): 74-76.
-
Krishnamurthy A, Vijayalakshmi R, Gadigi V, Ranganathan R, Sagar TG (2012) The Relevance of “Nonsmoking- Associated Lung Cancer” in India: A Single-Centre Experience. Indian J Cancer 49(1): 82-88.
-
Shetty CM, Lakhkar BN, Gangadhar VSS, Ramachandran NR (2005) Changing Pattern of Bronchogenic Carcinoma: A Statistical Variation or a Reality? Indian J Radiol Imaging 15(2): 233-238.
-
Al-Rahim YA (2007) Lung Cancer in a Sample of Iraqi Patients. Al-Kindy Col Med J 4(1): 53-59.
-
Purandare NC, Rangarajan V (2015) Imaging of Lung Cancer: Implications on Staging and Management. Indian J Radiol Imaging 25(2): 109-120.
-
Vinay C, Sowmya M (2019) A Study to Evaluate the Imaging Characteristics of Bronchogenic Carcinoma by MDCT with Histopathological Correlation. MedPulse J Radiol 11(2): 82-85.
- Teaching Cognitive Behavioral Therapy to Graduate Psychiatric Mental Health Nurse Practitioner Students: Utilizing A Mixed Methods Course Evaluation
- The Role of Pharmacogenetic Testing in Clinical Practice: A Path toward more Effective, Personalized and Cost-effective Care
- Implementing Screening with the GAD-7 in an Outpatient Mental Health Setting: A Quality Improvement Project
- Social Media and Health Promotion
- Impact of Covid-19 Pandemic on the Academic Performance and Attitude of Nursing Students towards E-Learning
- A Study to Assess the Knowledge Regarding Ill Effects of Tobacco Consumption on Health among Adolescents in Selected Higher Secondary School in Nadiad City