Applications of Nanomaterials in Dental Appliances
Introduction: The evolutionary microbes develop resistance against the prior encountered less-effective antimicrobial agents. Most of the conventional materials used in dental appliances, fail to achieve the efficacy to inhibit the biofilm accumulation and replication. The objective of this review article is to provide an update on applications of metal nanoparticles and metal oxide nanoparticles in the development of modern nanocomposites, nano-sealers, ionomeric cements, dental implants, and prosthetics of superior quality. Data Source: Electronic databases like PubMed/Medline, google scholar, and Scopus were searched with proper keywords. The final study was performed using 164 articles short-listed out of 349 total documents found. Conclusion: Nanotechnology can rightly be called the “disruptive technology” in dental science. It is successfully replacing the old technology along with its existing market and value network. Moreover, the development of stimuli-responsive selfrepairing materials and dental hard tissue regenerative materials are in demand. Nanotechnology is definitely the solution. Though different dental nanoceramics have enhanced structural integrity through defect control and damage tolerance, more extensive investigation is required for the successful clinical use of those products. Nano-biosensing is at an early stage in dental science, it will definitely play a critical role in the future development of dental materials.
Introduction
The innovations in the field of nanoscience and nanotechnology helped in overcoming many problems associated with the evolutionary growth of bacterial resistance towards the present interventions in the field of dental diagnosis [1]. The human oral microbiota consists of several bacteria and other microorganisms that are genuinely helpful for digestion and metabolism. But sometimes they affect their own surrounding and give rise to acute and chronic infections in the oral cavity. The dental science believes in the complete elimination of the infection from the human system. The acute stage is treated with antibiotics and further severity leads to application of restorative dentistry and endodontics. Whereas, in extreme cases of infection, dental surgery and dental prosthetics are suggested [2].
The emergence of nanotechnology in dentistry has led to the modification of the dental materials with nanoparticles. The nanoparticles are advantageous due to their smaller size and high drug loading capacity, rather they can also be specially functionalized to any predetermined target tissues and organs. But, cytotoxicity of nanomaterials is a major issue of concern. Keeping these facts in mind, the nanoparticles are incorporated with various dental materials like dental implants, polishing agent, caries prevention agent, teeth whitening agent, anti-sensitivity agent and dental fillings materials [3].
Materials and Methods
The electronic databases PubMed/Medline, Google Scholars, and Scopus have been searched with the phrases like “Metal nanoparticles in oral infection”, “Antimicrobial activity of nanoparticles”, “Application of nanoparticles in dentistry”, “Pharmacodynamics of metal nanoparticles”, “Interpretation of metal nanoparticles in dental science”, “Implication of metal nanoparticles in dental implants”, “Silver nanoparticles in dental materials”, and “Copper nanoparticles in dental materials”, Initially, the title, keywords, and abstract of individual manuscript was checked. The search result contained a total of 349 articles (review and research) published between 2011 to 2022. Out of them, 164 documents were selected for study. 93 documents have been cited in this review work. The main study was performed on: (1) the present interventions that are used for the treatment of oral infections; (2) reasons for selecting nanoparticles as complementary to antibiotics; (3) application of different nanoparticles in various dental materials; and (4) toxicity effect of nanoparticles.
Etiology of Oral Infections
The human oral microbiota consists of various bacteria, fungi (Candida, Cladosporium, Aureobasidium, Aspergillus, Fusarium, and Cryptococcus), and viruses. It has mostly similar composition in all healthy humans [4]. The most common oral bacteria include Streptococcus mutans [5] (main component of the oral microbiota and one of the main components of dental plague), Porphyromonas gingivalis [6] (Gram-negative anaerobic bacterium), Staphylococcus and Lactobacillus [4] Another important microorganism is Candida, that remains neutral in normal oral microbiota, but when the oral microbiota balance is broken, they form biofilms with Streptococcus to play a pathogenic role [7]. These accumulation of bacteria in dental cavities of molars and premolars results in spread-out of infection to adjacent structures. Some common oral infections have been discussed below.
Dental Caries or Cavities
Dental cavities are holes in the teeth that cause decaying of tooth. They are the most common oral infections; besides, it also provides shelter to most of the bacteria [8]. The bacteria present in oral cavities are also responsible for food digestion. The decaying of tooth is generally caused by the bacteria Streptococcus mutans (mostly in children) [4]. S. mutans are feed on sugary substances from foods and beverages. The consumed carbohydrates are also broken-down into glucose inside oral cavity. This initiates the bacteria to produce acid causing erosion of tooth [9]. Normally, the teeth are replenished by the saliva between meals [8]. However, when a person consumes fermented food frequently, more acid is produced by the bacteria that cause a sustained acidic pH at the site of erosion leading to decaying of tooth.
Gingivitis
The word ‘Gingivitis’ has been derived from the word “gingiva” which means “gums”. It’s generally referred as the development of bacterial settlement in the gumline. The bacteria produces toxin, which causes swelling and inflammation of gingiva (gums) [8]. Gingivitis is considered as the primary stage of infection, because the severity in this condition may lead to chronic periodontitis. The common symptoms of gingivitis are bleeding gums, sensitive gums, and swelling gums. The onset of gingivitis can be reversible and treatment at this stage is effective [10].
Periodontal Disease
Periodontitis is the secondary stage of gingivitis. The bacteria penetrate deep into the periodontium tissue and cause severe infection. With chronic effect it may lead to permanent loss of teeth [11]. Periodontal disease is a local infection with bacterial growth in the gingival cervices. It affects the structural organs surrounding the teeth such as periodontal ligament, connective tissue, and bone [12]. The warm and moist pocket environment of the cavity fasters the growth rate of Gram-negative, anaerobic bacteria that proliferate in the sub gingival space [13].
Dental Abscess
It is the formation of pus inside the soft pulp of the tooth and gum due to bacterial infection. It is also called periapical infection that arises typically at the secondary stage of dental caries [13]. Breakdown of the protective enamel layer due to poor dental hygiene causes invasion of oropharyngeal bacteria in the dental cavity leading to local infection [13].
Biofilms: A dental threat
Both the micro-organisms of endogenous source (i.e., microorganisms that are normally found in mouth like bacteria causing periodontal disease and dental caries) and exogenous source (i.e., microorganisms not normally present in oral microbiota) are responsible for oral infection. They give rise to the formation of biofilms [14] that are the multi- cellular colonies of bacteria adhering to the substratum and providing advanced protection against antibiotics and host defence mechanism [14]. Initially, the bacteria adhere reversibly to a substrate where it secrete binding molecules (like adhesion protein) that leads to irreversible attachment of the biofilms [15]. After settling at the site, the bacteria multiply to form colonies inside the peptidoglycan envelop resulting in the formation of mature biofilms. Hence, biofilm provides a reservoir of bacteria that leads to chronic infection [16]. Moreover, biofilm is poorly responsive towards conventional antibiotics and may develop resistance to antibiotics [17].
Antimicrobial Resistance of Biofilms
All the bacteria growing in biofilms are recognised to be more resistant to antibiotics as compared to the same microbe growing in planktonic state [18]. There are several factors related to the development of antibiotic resistance (against Penicillin, Sulphonamide, Ampicillin, Vancomycin, Erythromycin, Methicillin, Ciprofloxacin, Linezolid, and Ceftaroline) over a long period of time [19]. The most important factor is the slower growth rate of the bacteria in biofilms that makes them less available for most of the antibiotics, but not for all (like metronidazole, amoxicillin, and tetracycline) [14]. In many studies it is mentioned that, the response of the bacteria against antibiotics and biocides depends upon the growth rate, nutritional status, pH, temperature, or any kind of prior exposure to antimicrobial agents [20]. Changes in any of these parameters results in varied response to antibiotics within a biofilm. When the bacterial cell experiences environmental stress it secretes stress protein (also called as “Heat-shock proteins”) that protects the cell from the external damages [14]. The exopolymer matrix of the bacterial cell has the ability to retard the diffusion of antibiotics through it, and the antibiotic get trapped, concentrated in the polymer matrix, and subsequently get inactivated. Moreover, the bacterial cells within biofilms have expressed gene that is dormant in the same organism within planktonic system. Hence, the memory of the prior encounters promotes the resistivity of the cells against antibiotics [14].
Antibiofilm Activity of Nanoparticles
On the basis of bacterial cell wall formation, bacteria are classified as Gram-positive and Gram-negative bacteria. The gram-positive bacteria have a thicker layer of peptidoglycan cell wall in comparison to gram-negative bacteria, that composed of alternating linear chain formed by residues of N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) arranged in a sequence of 3 to 5 amino acid that are cross linked to each other, results in a mess like structure [21]. Additionally, the presence of teichoic acid (with high level of phosphate group) starting from the cell wall to the surface of gram-positive bacteria makes them negatively charged [21]. Whereas, the gram-negative bacteria have a slight complex outer cell structure than gram-positive bacteria due to the presence lipopolysaccharide outer membrane covering the peptidoglycan cell wall [19]. The lipopolysaccharide (LPS) is composed of inner phospholipid layer and outer glycolipid layer that impart a strong negative charge on the cell surface. LPS is the major molecule responsible for the endotoxic shock associated with the septicaemia (blood poisoning) caused by gram-negative bacteria [22].
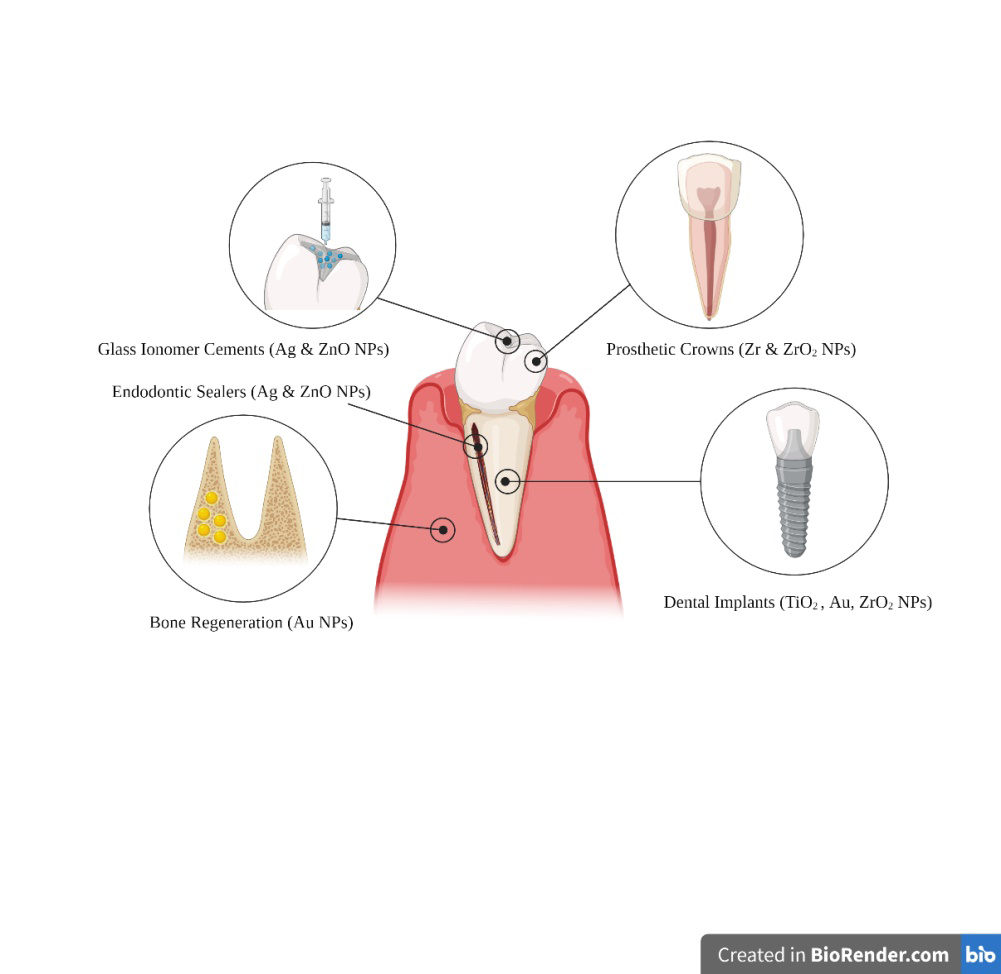
The metal and metal oxide nanoparticles are administered according to various strategies to combat with the microbial resistance by penetrating the bacterial cell wall, which further leads to destruction of bacterial cell due to oxidative stress [23]. Some nanoparticles are exclusively fabricated as the antibacterial agents, and they are quite effective as compare to other antimicrobial agents and antibiotics. Nanoparticles like nitric-oxide releasing nanoparticle (NO NPs), chitosan-containing nanoparticles (chitosan NPs), and metal nanoparticles (metal NPs) are widely used as the active antimicrobial agents [24]. Whereas, in some cases nanoparticles are also used as the carrier for several antibacterial agents. In this way nanoparticles are effectively overcome the problems of existing microbial resistance mechanisms like decreased uptake and increased efflux of drug from the bacterial cell (like liposomes and dendrimers) [25], formation of biofilms (like NO nanoparticles) [26], and intercellular bacterial growth (like liposomes) [27]. Application of Nanoparticles in Dental Materials The applications of nanotechnology in dentistry have been summarized in (Table 1). The nanotechnology is adapted in dentistry for maintenance of comprehensive oral health. Nanomaterials are the major part of nanodentistry as they act as the structural element for many dental restoratives and implants. The nanoparticles are used in dentistry as (1) drug carriers (Solid lipid nanoparticle, hydrogel and dendrimers) [28]; (2) antimicrobial therapeutics (chitosan nanoparticle, metal and metal oxide nanoparticles of Cu, Zn, Ag, Cr, and Ti) [29]; (3) Reinforcement nanoparticles (hydroxyapatite, nano-silica, nano-zirconia, nano-carbon) [30] (as shown in Figure 1). Nanomaterials are also find applications in the production of periodontic, endodontic, orthodontic, and prosthodontic materials.
Restorative Dentistry (Periodontic Treatments)
The patients with dental caries are usually treated with materials those are morphologically similar to human teeth. These materials are called dental restoratives as they assist to repair or replace the infected part. But the failure in restoration process may occurs due to lack of antimicrobial properties which leads to demineralization of tooth by microbial acid production [31]. The emergence of nanoparticles (including Ag NPs, ZnO NPs, and quaternary ammonium polyethyleneimine NPs) as dental restoratives and remineralizing substances (includes calcium phosphate nanoparticles, calcium fluoride nanoparticles, nanohydroxyapatite, and nanofluorohydroxyapatite ) [32], are introduced in the form of nanocomposites, glass ionomer cement, endodontic sealers (endodontics), and tooth regeneration.
Nanocomposites
The introduction of nanocomposites have solved the issues regarding strength, polymerization shrinkage, and wear resistance [33]. Incorporation of nanoparticles in resin composites are the primary approach to treat microorganism biofilm with direct contact [31]. Some studies involve the incorporation of 1% silver nanoparticle and zinc Oxide (ZnO) for effective antibacterial activity with direct contact. It was noted from the outcomes that the antibacterial effect of nanocomposite containing ZnO NPs on S. mutans was significantly higher than composite containing AgNPs [34, 35]. Whereas, the AgNPs containing resin composites shows significant inhibition of S. mutans when they were synthesized in-situ using photoreduction mechanism accompanied by polymerization reaction [36].
Nanoparticles are also incorporated in restorative dentistry as nanofiller and nanohybrids because they increase the surface tension of adhesives [37]. Silver and amorphous calcium phosphate nanoparticles have widely been used as adhesives because they enhance the band strength with effective antibacterial effect [38]. The magnetic nanoparticles (containing an iron core and silica coating shell, silanized with vinyl groups on the surface to covalently bond to the resin matrix) loaded adhesives have better penetration ability in dentin due to better microshear bond strength [39].
Glass Ionomer Cements
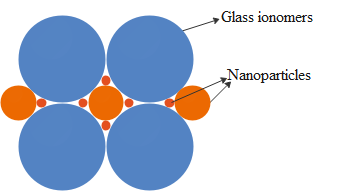
The nanoparticles are also administered in the form of nanoionomers for the preparation of nano glass ionomers. The nano glass (made up of fluoroaluminosilicate glass) ionomers are more efficient as compare to conventional glass ionomers because the addition of nanomers in the cement reduces the porosity by filling the pockets between the glass particles present in the cement [40, 41] (as shown in Figure 2). The nanoparticles like copper, titanium dioxide, hexametaphosphate, and zinc oxide are widely used in glass ionomer cements (GICs) that includes bioactive glass, CPP- ACP (Casein phosphopeptide amorphous calcium phosphate complex), reinforced GIC, zirconomer, chlorhexidine GIC, nano bioceramic impregnated GIC, ceramirand giomer [42] for better antibacterial efficacy, improved mechanical strength, and reduced collagen degradation [43].
There is another development called “equia system”, which is a resin coated high viscosity GIC of 40nm size. Considering the evolution of GICs this glass ionomer filling technology focused on the limit of hardness and resistance to strength through a novel high-viscosity GICs. It provides better resistance to dissolution, disintegration, and wear. They able to maintain a polished effect over the surface of restorative material for a longer period of time [44]. The smaller particle size of the nanomaterials present in equia system enhances the optical appearance and translucency as compared to conventional GICs. In a study performed by Friedl, et al. [45] on the performance of this new glass ionomer cements and concluded equia system as the better intervention for posterior filling material. There is also a secondary approach by organic nanoparticles to reduce demineralization of oral structures and results in remineralization by using the nanoparticles of amorphous calcium phosphate (NACP) combinedly with polymerizable quaternary ammonium methacrylates (QAMs). These modified composites have effective antibacterial action for long-term durability [46] and are applicable to various dental composites, adhesives and cements to reduce the chances of plaque biofilm formation due to restorative dentistry.
Root Canal Therapy (Endodontic Treatments)
The onset of secondary dental caries results in pulpitis and apical periodontitis, and the application of nanoparticles increases due to their benefits over conventional materials. These nanoparticles are incorporated in the form of sealer, obturating material, intracanal medicament, and irrigating solution to provide better results.
Root Canal Irrigation
It is a process of washing the root canal with a stream of fluid. Whereas, intracanal irrigation represents physically removal of materials from the canal and filling with chemical for antimicrobial activity, demineralization, tissue dissolution, bleaching, deodorizing, and haemorrhage controls. Some commonly used irrigants are chlorhexidine (CHX), ethylenediaminetetraacetic acid (EDTA) and sodium hypochlorite (NaOCl).
Sodium hypochlorite is an ideal irrigant used regularly. It can dissolve organic and inorganic tissues and also caused oxidation and hydrolysis of cellular protein. But, their accidental administration beyond apical foreman of the tooth having serious concerns of cytotoxicity [47]. Chlorhexidine is biologically safer than NaOCl but they have less ability to eliminate biofilm layer from the root canal. Introduction of chitosan nanoparticles on behalf of conventional irrigants have effective antibiofilm properties and ability to inhibit bacterial endotoxin. Hence, they are suggested to use as the finishing rinse in root canal irrigation and they are non-toxic to animal cells [48].
Bulk Fillers (Obturation)
Commonly used bulk fillers during obturations are Gutta percha (GP), silver points, and resilon. They are biocompatible, inert, and structurally stable. Lee, et al. [49] reported in a study that the incorporation of nano-diamond GP (NDGP) composite with amoxicillin results in enhanced mechanical properties like elastic modulus and strength, over other conventional GP.
Sealers
The developing technology combines the endodontic sealants with obturating materials to achieve a three- dimensional packing material for root canal. The endodontic sealers help to fill the gap between obturating materials and root dentin and to achieve a fluid-snug seal. Zinc oxide is used as nanoparticles in sealing agents and is commercially available as NanoSeal-S (Prevest DenPro) [50]. In a study performed by Del Carpio-Perochena, et al. [51] on addition of chitosan in endodontic sealers, results in enhanced antibacterial activity for longer period of time.
Zoufan, et al. [52], in a study discuss about a bioceramic based nanomaterial is prepared using calcium silicate, calcium phosphate, calcium hydroxide, zirconia and a thickening agent. Their nano-sized particles allowed the delivery of sealing material through 0.012 capillary needle and adapt the irregular dentin surface. It sets hard with few hours and upon setting hard they form hydroxyapatite provides biocompatibility. They also have effective antimicrobial activity due to their high alkaline pH 12.8 [52]. Another development is a silicon-based sealer (Gutta-Flow sealer) which comprised with powder of gutta percha and silver nanoparticles. It’s found in the form of uni-dose capsule that are easy to mix and injected [52], they also have better sealing ability and prevention against bacterial invasion in root canal. Researchers also developed quaternary ammonium polyethyleneimine (QPEI) nanoparticles for addition into existing sealers like AH plus, Epiphany, and Guttaflow. The addition of QPEI up to 2 % (w/w) does not compromise with the biocompatibility or the mechanical properties of the sealers, but provides prolonged antibacterial activity [53].
Orthodontic Treatments
The orthodontics is the part of dental science that deals with the problem of malocclusion or misalignment of teeth. The orthodontists are the specialist that focuses on correcting bite, occlusion, and the straightness of teeth to provide better oral health. But the fixed orthodontic appliances create areas inside the mouth that are difficult to keep clean. So, they are also one of the reasons for the biofilm accumulation in the oral cavity and increasing the chances of enamel demineralization in the patient. There is formation of “white spot lesions” or WSLs as a consequences of dental caries due to the production of organic acid by the microorganisms present in the biofilm [54]. So modern nanotechnology develops several other interventions to successfully inhibit the biofilm accumulation.
Orthodontic ligatures
The orthodontic elastomeric ligature (OEL) are synthetic elastic modules made up of polyurethane material, that makes their application towards patient compliance. Whereas, they are also used most as they’re inexpensive. Some studies shows the long term ineffectiveness of conventional elastic ligatures and also their ineffectiveness over decalcification [55, 56, 57]. So, the proposal of administering the conventional elastomeric ligatures as the transporter of nanoparticles, which may include molecules with anticarcinogenic properties or anti-inflammatory activity, and also antibiotics with elastomeric matrix. The application of medicated wax in orthodontic brackets successfully reduce the mucosal irritation cause due to brackets with a continuous release of benzocaine shown more effective results [58]. Hernández- Gómora, et al. [57], in a study stated that the incorporation of silver nanoparticles in orthodontic elastomeric ligatures is convenient due to the strong antibacterial mechanism of silver nanoparticles and also the silver is not much toxic for human cells (Table 1).
| SL. NO. | Nanoparticle | Use in dentistry |
|---|---|---|
| Antimicrobial nanoparticles | ||
| 1 | Chitosan | • Restorative composites |
| • Adhesive dentistry | ||
| • Periodontology | ||
| • Implant odontology | ||
| 2 | Quaternary ammonium compound | • Restorative composites |
| • Adhesive dentistry | ||
| • Periodontology | ||
| • Endodontics | ||
| 3 | Polymeric triclosan | • Periodontology |
| 4 | Copper-based nanomaterials | • Implant odontology |
| 5 | Zinc-based nanomaterials | • Temporary materials |
| • Endodontics | ||
| • Adhesive dentistry | ||
| 6 | Amorphous calcium phosphate | • Periodontology |
| • Endodontics | ||
| 7 | Titanium dioxide | • Implant odontology |
| • Restorative composites | ||
| 8 | Nanosilver | • Temporary materials |
| Therapeutic nanomaterials | ||
| 1 | Cisplatin PEG-PolyGA | • Oral cancer |
| 2 | Solid lipid nanoparticles | • Oral cancer |
| • Periodontology | ||
| 3 | Hydrogels | • Periodontology |
| 4 | Gold nanoparticles | • Oral cancer management |
| 5 | Quantum dots | |
| 6 | Dendrimers | • Biomineralization |
| • Adhesive dentistry | ||
| Reinforcement nanostructures | ||
| 1 | Nanocarbon | • Biomineralization |
| • Adhesive dentistry | ||
| • Prosthodontics (acrylic resins) | ||
| • Restorative dentistry | ||
| 2 | Nanosilica | • Endodontics |
| • Biomineralization | ||
| • Restorative composites | ||
| 3 | Nanozirconia | • Endodontics |
| • Biomineralization | ||
| • Restorative composites | ||
| • mplant odontology | ||
| • Bioceramics | ||
| 4 | Polymeric nanogel | • Restorative composites |
| • Adhesive dentistry | ||
| 5 | Nanohydroxyapatite | • Implant odontology |
| • Biomineralization | ||
| • Adhesive dentistry |
Table 1: Application of nanotechnology in Dentistry.
Orthodontic Power Chains
Orthodontic power chains are regularly used intervention that composed of polymeric material like polyester and polyether, formed through the process of polymerization. They provide light mechanical force continuously and are highly flexible to get fit in any patient. But their mechanical effectiveness is for a limited time, and needed to replace periodically. On the other hand, their effectiveness got affected due to both intrinsic (material composition, production method, and external morphology) and extrinsic factors (oral cavity temperature, pH and moisture absorption). Their hydrophilic (absorb fluid from oral cavity) characteristics leads to discoloration of material over time.
In a study performed by Cheng, et al. [59] in Taiwan, they conduct an experiment on conventional orthodontic power chains and develop their physical characteristics by using a surface treatment called ‘nanoimprinting’. In this treatment process nanostructures are developed on the surface of the power chains and stated as ‘nanopillars’ that transforms them from hydrophilic to hydrophobic materials.
Orthodontic Mini-Screws
The basic principle of orthodontic treatment is to develop a material with control anchorage at their site of application, along with a force system that apply desirable effect and avoid undesirable movements. They are inserted in bone and provide anchorage to the dental structures directly or indirectly to support the anchoring teeth. From past few years a lot of temporary anchorage devices (TADs) develop with orthodontic properties like mini-screws, miniplates, and implants [59]. Generally, TADs achieve their stability mechanically (cortical or bicortical stabilization) and do not require biomechanical osseointegration [60]. Mini-screws are commonly used due to their versatile nature (available in favourable size, simple to insert and remove, inexpensive, and easy to perform application by any skilled practitioner.
Two studies were performed [61, 62], to evaluate the stability and osseointegration of mini-screws having modified surface due to nanoparticles. The surface study was characterised by titanium oxide nanotube array loaded with RhBMP-2 (recombinant human bone morphogenicprotein-2) and ibuprofen were evaluated against standard mini-screws [61]. They concluded better effectiveness of the drug loaded mini- screws and their positive impact on the tissue health. Prosthodontic Treatments Dental prosthetics deals with complex dental cases including jaw surgery, dentures, and implants. Prosthodontic treatments are associated with missing or defect teeth and oral or maxillofacial tissues. They are generally categorized in four types: (i) Fixed prosthodontics [63] (includes crown and bridge); (ii) Removable prosthodontics [64] (includes complete dentures and partial dentures); (iii) Maxillofacial prosthodontics [65] (includes obturators, speech bulb, palatal lifts, palatal augmentation); (iv) Dental implants. In prosthodontics, polymethyl methacrylate (PMMA) is the most commonly used biomaterial for the removal of partial or complete dentures, but it does not have antibacterial property [66]. The biomaterials are modified with nanofillers to improve antimicrobial efficacy without affecting the mechanical properties of the appliances. The nanoparticles used in this case are of silver (Ag) [67], platinum (Pt) [68], zinc or zinc oxide (Zn/ZnO) [69], titanium or titanium dioxide (Ti/TiO2) [70], and zirconium oxide (ZrO2) [71]. Out of these, titanium dioxide exhibits better extent of activity against both Gram-positive and Gram-negative bacteria. In a study [70], four inorganic antibacterial material with nanofillers (like Ag-supported Zr phosphate (Navaron), tetrapod like Zn-oxide whiskers (T-ZnOw), TiO2NPs, AgNPs) are compared along with PMMA composites. The results indicated that the nanofiller like Navaron and T-ZnOw shows significantly better antibacterial activity and exhibits no cytotoxicity, whereas, the TiO2 and Ag-based nanoparticles have minimal cytotoxicity [70]. Toxicity The toxicity of the nanoparticles may be due to many factors like size, shape, surface area, surface charge, chemical composition, chemical stability, as well as route of exposure. Some studies reported no significant toxic effects of nanoparticles[1, 72, 73, 74, 75, 76], while other studies found better antibacterial activity with no cytotoxic effect within a certain range of concentration administered [70, 77, 82]. The studies revealed that administration of nanoparticles exceeding a certain level of concentration causes accumulation of NPs in different organs leading to oxidative stress and toxicity. However, in a study it was explained that the toxicity of nanoparticles are time dependent rather than their concentration [35].
There are several techniques to reduce the toxicity of the metal nanoparticles in dental treatments. Some researchers have proven that variations in the methods to develop surface properties of the individual nanoparticles, lead to production of better non-toxic nanoparticles with desirable properties [83]. The above mentioned factors affects one or more of the following mechanisms to manifest the toxicity (i) direct association of nanoparticles with the organisms’ cell surface, (ii) dissolution of the nanomaterial through various delivery systems leads to release of toxic metal ions that impact the organisms, and (iii) generation of ROS and oxidative stress, that leads to the damage of the cells [84]. So, to overcome these limitations of nanoparticles in dentistry, several redesign strategies are evolving day-by-day.
Like, the researchers develop toxicity study of several nanoparticles having variable surface charges. In a study, they used negatively charged ligands having PEG coating, and the PEG helps to reduce toxicity by reducing the binding affinity of the nanoparticles with the eukaryotic cells [85]. The PEG coating improves the nanoparticles’ stability that also elevate the bioavailability time and environmental persistence of the nanoparticles in the physiological medium [86]. Besides this, in an experimental study [87], associating NMC (Nickel, Manganese, Cobalt) demonstrate the release of nickel and cobalt ions dominates the toxicity to S. oneidensis for a study on Lithium-ion battery. This experiment aims to reduce the Ni and Co concentration and increasing the Mn. After performing respirometry to monitor the bacterial growth in both the cases with excess Mn and normal formulation. And that results in reduced overall toxicity of the nanomaterial, but reduced efficacy of the nanomaterial on the bacterial growth are also observed. On the other hand, the application of ZnS coating on the cadmium selenide quantum dots as high energy band gap material is done to maintain the core integrity and to improve the quantum yield of the nanoparticle, but the coating also reduce the material’s ability to produce ROS, hence reduce toxicity [88].
Conclusion and Future Prospects
The readers of this article are nurtured with the facts behind encouraging the application and bio-safety of nanoparticles in dental appliances. The work represented here contains the wide range of applications of antimicrobial nanoparticles in restorative dentistry, endodontics, dental implants, orthodontics, and dental prostheses. Besides, having significant antibacterial properties, the nanoparticles also exhibit toxicological effect depending on factors like concentration, time, size, shape, route of exposure, surface charge, chemical composition, and chemical stability. The modern dental science takes initiatives to overcome the limitations but several studies are required in future to establish successful strategies for development of non-cytotoxic antibacterial nanoparticles loaded dental accessories. Hence, nanotechnology in dental materials can be called as “disruptive technology”, which means a new technology that can successfully replace the old technology along with its existing market and value network. The development of stimuli responsive self-repairing materials, and dental hard tissue regenerative material are in demand. The nanotechnology is definitely the solution. Though different dental nanoceramics have enhanced the structural integrity through defect control and damage tolerance [89], more extensive investigation is required for successful clinical use of those products. Nano-biosensing is at early stage in dental science [90], it will definitely play a critical role in the future development of dental materials [91].
Conflict of Interest
The authors declare NO conflict of interest.
References
-
Agnihotri R, Gaur S, Albin S (2020) Nanometals in Dentistry: Applications and Toxicological Implications-a Systematic Review. Biol Trace Elem Res 197(1): 70-88.
-
Lubojanski A, Dobrzynski M, Nowak N, Soroczynska JR, Sztyler K, et al. (2021 ) Application of Selected Nanomaterials and Ozone in Modern Clinical Dentistry. Nanomaterials 11(2): 259.
-
Priyadarsini S, Mukherjee S, Mishra M (2018) Nanoparticles used in dentistry: A review. J Oral Biol Craniofacial Res 8(1): 58-67.
-
Lu M, Xuan S, Wang (2019) Oral microbiota: A new view of body health. Food Science and Human Wellnes 8(1): 8-15.
-
Loesche WJ (1986) Role of Streptococcus mutans in human dental decay. Microbiol Rev 50(4): 353-380.
-
How KY, Song KP, Chan KG (2016) Porphyromonas gingivalis: An overview of periodontopathic pathogen below the gum line. Front Microbiol 7: 1-14.
-
Baker JL, Bor B, Agnello M, Shi W, He X (2017) Ecology of the Oral Microbiome: Beyond Bacteria. Trends Microbiol 25(5): 362-374.
-
Bmedsc GR (2017) Bacteria Infections Oral cavity Microbiology Microbiome. Dent Clin NA 61(2): 305-318.
-
Belibasakis GN, Mylonakis E (2015) Oral infections : clinical and biological perspectives. Virulence 6(3): 173- 176
-
Gasner NS, Schure RS (2020) Periodontal Disease, StatPearls, Treasure Island, Florida, USA.
-
Victor M (2019) Periodontal film for the treatment of periodontal disease. Journal of Pharmaceutical Sciences and research 11(7): 2579-2584.
-
Kinane DF, Stathopoulou PG, Papapanou PN (2017) Periodontal diseases. Nat Rev Dis Primers 3.
-
Shweta, Prakash SK (2013) Dental abscess: A microbiological review. Dent Res J (Isfahan) 10(5): 585- 591.
-
Saini R, Saini S, Sharma S (2011) Biofilm: A dental microbial infection. J Nat Sci Biol Med 2(1): 71-75.
-
Beyth N, Houri-Haddad Y, Domb A, Khan W, Hazan R (2015) Alternative antimicrobial approach: Nano- antimicrobial materials. Evidence-based Complement. Altern Med pp: 1-16
-
Watnick P, Kolter R (2000) Biofilm, City of Microbes. American Society for microbiology 182(10): 2675-2679.
-
Haque M, Sartelli M, Haque SZ (2019) Dental infection and resistance-global health consequences. Dent J 7(1): 22.
-
Lindhe J, lang NP (2013) Clinical Periodontology and Implant Dentistry In: (Sixth edition), J Chem Inf Model 53(9): 1689-1699.
-
Sánchez-López E, Gomes D, Esteruelas G, Bonilla L, Lopez- Machado AL, et al. (2020) Metal-based nanoparticles as antimicrobial agents: An overview. Nanomaterials 10(2): 292.
-
Socransky SS, Haffajee AD (2002) Dental biofilms: Difficult therapeutic targets. Periodontol 2000 28(1): 12-55.
-
Slavin AN, Asnis J, Häfeli UO, Bach H (2017) Metal nanoparticles: understanding the mechanisms behind antibacterial activity. Journal of Nanobiotechnology 15(1): 1-20.
-
Silhavy TJ, Kahne D, Walker S (2010) The Bacterial Cell Envelope. Cold Spring Harb Perspect Biol 2(5).
-
Yin IX, Zhang J, Li Q, Zhao IS, Mei ML, et al. (2020) The Antibacterial Mechanism of Silver Nanoparticles and Its Application in Dentistry. International Journal of Nanomedicine 2020(15): 2555-2562.
-
Pelgrift RY, Friedman AJ (2013) Nanotechnology as a therapeutic tool to combat microbial resistance. Adv Drug Deliv Rev 65(13-14): 1803-1815.
-
Gao W, Chen Y, Zhang Y, Zhang Q, Zhang L (2018) Nanoparticle-based local antimicrobial drug delivery. Adv Drug Deliv Rev 127: 46-57.
-
Hetrick EM, Shin JH, Paul HS, Schoenfisch MH (2009) Anti-biofilm efficacy of nitric oxide-releasing silica nanoparticles. Biomaterials 30(14): 2782-2789.
-
Huh AJ, Kwon YJ (2011) Nanoantibiotics: A new paradigm for treating infectious diseases using nanomaterials in the antibiotics resistant era. J Control Release 156(2): 128-145.
-
Elkassas D, Arafa A (2017) The innovative applications of therapeutic nanostructures in dentistry. Nanomedicine Nanotechnology Biol Med 13(4): 1543-1562.
-
Gordon SB, Shaddox LM (2020) Nanoparticles in Dentistry: Evidence and Future. American Journal of Biomedical Science and Research 8(4): 321-323.
-
Xia Y, Zhang F, Xie H, Gu N (2008) Nanoparticle-reinforced resin-based dental composites. J Dent 36(6): 450-455.
-
Kasraei S, Sami L, Hendi S, AliKhani MY, Rezaei-Soufi L, et al. (2014) Antibacterial properties of composite resins incorporating silver and zinc oxide nanoparticles on Streptococcus mutans and Lactobacillus. Restor Dent Endod 39(2): 109-114.
-
Melo MAS, Guedes SFF, Xu HHK, Rodrigues LKA (2013) Nanotechnology-based restorative materials for dental caries management. Trends Biotechnol 31(8): 459-467.
-
Ozak ST, Ozkan P (2013) Nanotechnology and dentistry. European Journal of Dentistry 7(1): 145-151.
-
Andrade V, Martínez DDS A, Rojas N, Bello Toledo H, Flores P, et al. (2018) Antibacterial activity against Streptococcus mutans and diametrical tensile strength of an interim cement modified with zinc oxide nanoparticles and terpenes: An in vitro study. The Journal of Prosthetic Dentistry 119(5): 862e1-862e7.
-
Dutra Correa M, Leite A, PHM de Cara S, MA Diniz I, Marques MM, et al. (2018) Antibacterial effects and cytotoxicity of an adhesive containing low concentration of silver nanoparticles. Journal of Dentistry 77: 66-71.
-
Saafan A, Zaazou MH, Sallam MK, Mosallam O, El Danaf HA (2018) Assessment of Photodynamic Therapy and Nanoparticles Effects on Caries Models. Open Access Maced J Med Sci 6(7): 1289-1295.
-
Zhang M, Liu M, Bewick S, Suo Z (2009) Nanoparticles to Increase Adhesive Properties of Biologically Secreted Materials for Surface Affixing. J Biomed. Nanotechnol 5(3): 294-299.
-
Eanes ED (2001) Amorphous Calcium Phosphate Monogr Oral Sci 18: 130-147.
-
Li Y, Hu X, Xia Y, Ji Y, Ruan J, et al. (2018) Novel magnetic nanoparticle-containing adhesive with greater dentin bond strength and antibacterial and remineralizing capabilities. Dent Mater 34(9): 1310-1322.
-
Gjorgievska E, Tendeloo GV, Nicholson JW, Coleman NJ, Slipper IJ, et al. (2015) The Incorporation of Nanoparticles into Conventional Glass-Ionomer Dental Restorative Cements. Microsc. Microanal 21(2): 392- 406.
-
Jandt KD, Watts DC (2020) Nanotechnology in dentistry: Present and future perspectives on dental nanomaterials. Dental Materials 36(11): 1365-1378.
-
Singh S (2019) Advances in Glass Ionomer Cement: A Review. Indian Journal of Contemporary Dentistry 7(2): 1-32.
-
Renné WG, Lindner A, Mennito AS, Agee KA, Pashley DH, et al. (2017) Antibacterial properties of copper iodide-doped glass ionomer-based materials and effect of copper iodide nanoparticles on collagen degradation. Clinical Oral Investigations 21(1): 369-379.
-
Basso M, Brambilla E, Benites MG, Marta G, Lonescu AC (2015) Glassionomer Cement for Permanent Dental Restorations : A 48-Months. Stoma Edu J 2: 10-20.
-
Friedl K, Hiller KA, Friedl KH (2011) Clinical performance of a new glass ionomer based restoration system: A retrospective cohort study. Dental Materials 27(10): 1031-1037.
-
Pietrokovski Y, Nisimov I, Kesler-Shvero D, Zaltsman N, Beyth N (2016) Antibacterial effect of composite resin foundation material incorporating quaternary ammonium polyethyleneimine nanoparticles. J Prosthet Dent 116(4): 603-609.
-
Cárdenas-Bahena A, Sánchez-García S, Tinajero- Morales C, González-Rodríguez VM, Baires-Várguez L (2012) Revista Odontológica Mexicana Use of sodium hypochlorite in root canal irrigation. Opinion survey and concentration in commercial products 16(4): 252-258.
-
Shrestha A, Kishen A (2014) Antibiofilm Efficacy of Photosensitizer-functionalized Bioactive Nanoparticles on Multispecies Biofilm. J Endod 40(10): 1604-1610.
-
Lee DK, Kim SV, Limansubroto AN, Yen A, Soundia A, et al. (2015) Nanodiamond–Gutta Percha Composite Biomaterials for Root Canal Therapy. ACS Nano 9(11): 11490-11501.
-
VPS root canal sealer.
-
Carpio-Perochena AD, Kishen A, Shrestha A, Bramante CM (2015) Antibacterial Properties Associated with Chitosan Nanoparticle Treatment on Root Dentin and 2 Types of Endodontic Sealers. J Endod 41(8): 1353-1358.
-
Zoufan K, Jiang J, Komabayashi T, Wang YH, Safavi KE, et al. (2011) Cytotoxicity evaluation of Gutta Flow and Endo Sequence BC sealers. Oral Surgery Oral Med Oral Pathol Oral Radiol Endodontology 112(5): 657-661.
-
Abramovitz I, Beyth N, Weinberg G, Borenstein A, David P, et al. (2012) In Vitro Biocompatibility of Endodontic Sealers Incorporating Antibacterial Nanoparticles. Journal of Nanomater 2012: 1-9.
-
Srivastava K, Tikku T, Khanna R, Sachan K (2013) Risk factors and management of white spot lesions in orthodontics. J Orthod Sci 2(2): 43-49.
-
Sharma R, Sharma K, Sawhney R (2018) Evidence of variable bacterial colonization on coloured elastomeric ligatures during orthodontic treatment: An intermodular comparative study. J Clin Exp Dent 10(3): e271-e278.
-
Sawhney R, Sharma R, Sharma K (2018) Microbial Colonization on Elastomeric Ligatures during Orthodontic Therapeutics: An Overview. Turkish J Orthod 31(1): 21-25.
-
Hernández-Gómora AE, Lara-Carrillo E, Robles-Navarro JB, Scougall-Vilchis RJ, Hernández-López S, et al. (2017) Biosynthesis of Silver Nanoparticles on Orthodontic Elastomeric Modules: Evaluation of Mechanical and Antibacterial Properties. Molecules 22(9): 1407.
-
Sharan J, Singh S, Lale SV, Mishra M, Koul V, et al. (2017) Applications of nanomaterials in dental science: A review. J Nanosci Nanotechnol 17(4): 2235-2255.
-
Cheng HC, Chen MS, Peng BY, Lin WT, Shen YK, et al. (2017) Surface Treatment on Physical Properties and Biocompatibility of Orthodontic Power Chains. Biomed Res Int 2017: 1-9.
-
Tsui WK, Chua HDP, Cheung LK (2012) Bone anchor systems for orthodontic application: a systematic review. Int J Oral Maxillofac Surg 41(11): 1427-1438.
-
Jang I, Choi DS, Lee JK, Kim WT, Cha BK, et al. (2017) Effect of drug-loaded TiO2 nanotube arrays on osseointegration in an orthodontic miniscrew: an in- vivo pilot study. Biomed Microdevices 19(4): 94.
-
Jang I, Shim SC, Choi DS, Cha BK, Lee JK, et al. (2015) Effect of TiO2 nanotubes arrays on osseointegration of orthodontic miniscrew. Biomed Microdevices 17(4): 76.
-
Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY (2003) Clinical complications in fixed prosthodontics. J Prosthet. Dent 90(1): 31-41.
-
Rao J, Singh GK, Alvi HA, Kumar L, Agrawal KK, et al. (2013) Removable partial denture with molar uprighting spring: An innovative hybrid appliance. J Prosthodont Res 57(1): 57-61.
-
Hanawa S, Kitaoka A, Koyama S, Sasaki K (2015) Influence of maxillary obturator prostheses on facial morphology in patients with unilateral maxillary defects. J Prosthet Dent 113(1): 62-70.
-
Yamada R, Nozaki K, Horiuchi N, Yamashita K, Nemoto R, et al. (2017) Ag nanoparticle–coated zirconia for antibacterial prosthesis. Mater Sci Eng C mater boil appl 78: 1054-1060.
-
Jo JK, El-Fiqi A, Lee JH, Kim DA, Kim HW, et al. (2017) Rechargeable microbial anti-adhesive polymethyl methacrylate incorporating silver sulfadiazine-loaded mesoporous silica nanocarriers. Dent Mater 33(10): e361-e372.
-
Nam KY (2014) Characterization and bacterial anti- adherent effect on modified PMMA denture acrylic resin containing platinum nanoparticles. J Adv Prosthodont 6(3): 207-214.
-
Kamonkhantikul K, Arksornnukit M, Takahashi H (2017) Antifungal, optical, and mechanical properties of polymethylmethacrylate material incorporated with silanized zinc oxide nanoparticles. Int J Nanomedicine 12: 2353-2360.
-
Chen R, Han Z, Huang Z, Karki J, Wang C, et al. (2017) Antibacterial activity, cytotoxicity and mechanical behavior of nano-enhanced denture base resin with different kinds of inorganic antibacterial agents. Dent Mater J 36(6): 693-699.
-
Sadowsky SJ (2020) Has zirconia made a material difference in implant prosthodontics? A review. Dent Mater 36(1): 1-8.
-
Kittler S, Greulich C, Diendorf J, Köller M, Epple M, et al. (2010) Toxicity of silver nanoparticles increases during storage because of slow dissolution under release of silver ions. Chem Mater 22(16): 4548-4554.
-
Madl AK, Plummer LE, Carosino C, Pinkerton KE (2014) Nanoparticles, Lung Injury, and the Role of Oxidant Stress. Annu Rev Physiol 76(1): 447-465.
-
Sukhanova A, Bozrova S, Sokolov P, Berestovoy M, Karaulov A, et al. (2018) Dependence of Nanoparticle Toxicity on Their Physical and Chemical Properties. Nanoscale Res Lett 13: 44.
-
Wang Y, Chen Z, Ba T, Pu J, Chen T, et al. (2013) Susceptibility of young and adult rats to the oral toxicity of titanium dioxide nanoparticles. Small 9(9-10): 1742- 1752.
-
Solla DF, Paiva TS, André M, Paiva WS (2015) Potential toxicity of dental nanomaterials to the central nervous system. Int J Nanomedicine 10: 5593-5594.
-
Woźniak A, Malankowska A, Nowaczyk G, Grześkowiak BF, Tuśnio K, et al. (2017) Size and shape-dependent cytotoxicity profile of gold nanoparticles for biomedical applications. J Mater Sci Mater Med 28(6): 92.
-
Akay C, Cevik P, Karakis D, Sevim H (2018) In Vitro Cytotoxicity of Maxillofacial Silicone Elastomers: Effect of Nano-particles. J Prosthodont 27(6): 584-587.
-
Zhang T, Wang L, Chen Q, Chen C (2014) Cytotoxic potential of silver nanoparticles. Yonsei Med J 55(2): 283-291.
-
Chan EL, Zhang C, Cheung GS (2015) Cytotoxicity of a novel nano-silver particle endodontic irrigant. Clin Cosmet Investig Dent 7: 65-74.
-
Lee YJ, Ahn EY, Park Y (2019) Shape-dependent cytotoxicity and cellular uptake of gold nanoparticles synthesized using green tea extract. Nanoscale Res Lett 14: 1-14.
-
Heravi F, Ramezani M, Poosti M, Hosseini M, Shajiei A, et al. (2013) In Vitro Cytotoxicity Assessment of an Orthodontic Composite Containing Titanium-dioxide Nano-particles. J Dent Res Dent Clin Dent Prospects 7(4): 192-198.
-
Ungor D, Dékány I, Csapó E (2019) Reduction of Tetrachloroaurate(III) Ions With Bioligands: Role of the Thiol and Amine Functional Groups on the Structure and Optical Features of Gold Nanohybrid Systems. Nanomaterials 9(9): 1229.
-
Buchman JT, Hudson-Smith NV, Landy KM, Haynes CL (2019) Understanding Nanoparticle Toxicity Mechanisms To Inform Redesign Strategies To Reduce Environmental Impact. Acc Chem Res 52(6): 1632-1642.
-
Xu L, Yang J, Xue B, Zhang C, Shi L, et al. (2017) Molecular insights for the biological interactions between polyethylene glycol and cells. Biomaterials 147: 1-13.
-
Tejamaya M, Römer I, Merrifield RC, Lead JR (2012) Stability of Citrate, PVP, and PEG Coated Silver Nanoparticles in Ecotoxicology Media. Environ Sci Technol 46(13): 7011-7017.
-
Manthiram A (2017) An Outlook on Lithium Ion Battery Technology. ACS Cent Sci 3(10): 1063-1069.
-
Derfus AM, Chan WCW, Bhatia SN (2004) Probing the Cytotoxicity of Semiconductor Quantum Dots. Nano Lett 4(1): 11-18.
-
Warreth A, Elkareimi Y (2020) All-ceramic restorations: A review of the literature. Saudi Dent J 32(8): 365-372.
-
Sagadevan S, Periasamy M (2014) Recent trends in nanobiosensors and their applications -A review Rev Adv Mater Sci 36(1): 62-69.
-
Priyadarsini S, Mukherjee S, Bag J, Nayak N, Mishra M (2020) Application of Nanoparticles in Dentistry: Current Trends. In: Shukla A (Eds.), Nanoparticles in Medicine. Springer, Singapore, pp: 55-98.
- Solution-Processed Chiral Perovskites for Biomedical Applications
- Nanotechnology in Health Chemistry and Medicine: Current Challenges and Future Directions
- Human Exposure to Micro- and Nanoplastics: Pathways, Toxicity, and Intervention Strategies
- Exosome Nanomedicine for Cancer Therapy
- Micro and Nanoplastics–Plastisphere, Biotoxicity, Impact on Human Health, and Mitigation Strategies
- Process Validation of Cefixime Powder for Suspension Dosage Form, 50 mL