Postoperative evaluation of Conservative Surgical Approach on Central Giant Cell Granuloma of the Mandible: A case report
Aggressive form of central giant cell granuloma has always causes challenging problem for oral and maxillofacial surgeons due to their high recurrence rate (55% - 70%). Therefore repetitive and extensive surgical procedures are required to resolve them. That has adverse psychosocial consequences particularly in young age and is prohibitively expensive. On the other hand, non-surgical procedures reported in literature also showed failure of treatment and need for future surgical intervention for aggressive central giant cell granuloma. Nevertheless, combined conservative surgical approach such as surgical curettage + peripheral osteotomy + local application of Carnoy’s solution followed by Iodoform gauze packing till complete soft tissue healing is advantageous for non-perforated large aggressive central giant cell granuloma. The aim of this study was to report the outcome of combined conservative surgical approach for aggressive central giant cell granuloma. The follow-up duration of the cases was 15 months.
Introduction
Central giant cell granuloma (CGCG) is an intraosseous localized benign but sometimes aggressive osteolytic proliferation consisting of cellular fibrous tissue with multiple foci of hemorrhage and haemosiderin deposits along with presence of osteoclast-like giant cells and reactive bone formation [1, 2, 3]. They account only 7% - 10% of all benign lesions of the jaws [4, 5]. Incidence rate of CGCG is twice in females in comparison to males of same high risk age group of under 30 years, with most common mandible localization [4, 5, 6]. Radiographically central giant cell granuloma looks like small unilocular radiolucent lesions to extensive multilocular radiolucent areas with or without well circumscribed margin, displacement of anatomical structures, root resorption, cortical expansion and perforation [2, 4, 6, 7]. Histologically CGCG contain focal arrangements of giant cells within a vascular stroma with thin walled capillaries adjacent to the giant cells [1, 2, 8, 9, 10]. On the above basis CGCG is subdivided into two groups namely non- aggressive or aggressive [2, 4, 6, 7]. Non-aggressive lesion is usually a small, asymptomatic and slow growing and does not show cortical and/or root resorption while aggressive lesion shows pain, expansion of cortex and perforation, mobility, displacement and root resorption of associated teeth [2, 3, 4, 5, 6, 7]. Initially condition was considered to be malignant. Later on in 1940 Jaffe considered it to be a true neoplasm (GCT) and in 1952 suggested the term giant cell reparative granuloma (GCRG). Reparative lesions have capacity to essentially self healing but current consensus reported these are not reparative lesions and if they are not treated, they are progressive. However, at present it is considered as a CGCG [1, 2, 6, 9, 10, 11]. Recent literature reported, choice of treatment for CGCG was mainly based on its non-aggressive or aggressive behavior and available treatment options for CGCG are non-surgical (corticosteroids, calcitonin and α-interferon) and surgical. Surgical management of CGCG was simple curettage with or without adjunct therapy to aggressive resection and appropriate reconstruction. Each treatment modalities have own merits and demerits [2, 3, 5, 10, 11, 12]. In other hand, previous literature reported overall incidence of recurrent were 15% – 20% in the CGCG but it may dramatically increase up to 55%-70% in case of aggressive lesions managed by simple curettage and most of them were encountered after few months of initial treatment [2, 5, 6, 13, 14]. The aim of the present study is to report and evaluate the success of conservative surgical approach to a new case of CGCG involving the right mandibular corpus, ramus and coronoid process managed by surgical curettage with peripheral osteotomy and local application of carnoy’s solution followed by iodoform gauze packing till complete soft tissue healing.
Case Description
A 21-year-old lady reported to our centre, complaining of an occasional pain and swelling in right lower posterior teeth region since last two years. She did not have any history of trauma. Her medical history was unremarkable. On extraoral examination, facial asymmetry was apparent with diffuse swelling involving the right side of face measuring 5.0x4.0 cm. The swelling was bony hard and non-tender on palpation. Intraoral examination revealed carious pulp exposed in relation to 48, grade-II mobility in 47 & 48 and vestibular obliteration was noted in right mandibular corpus and adjacent ramus (Figure 1A). Preoperative panoramic view radiograph shows multilocular well defined heterogeneous lesion extending from the mesial surface of the right mandibular first molar to the adjacent coronoid process and around 1cm of sound residual bone remaining in the lower border with inferior alveolar nerve (IAN) involvement as well as Vijay Kumar. Postoperative evaluation of Conservative Surgical Approach on Central Giant Cell Granuloma of the Mandible: A case report.J Dental Sci 2016, 1(2): 000114.
slight displacement of right mandibular second and third molar (Figure1B). Axial computed tomography revealed expansile lytic lesion involving the right mandibular posterior region shows multilocular trabuculation and heterogeneously enhancing matrix with cortical thinning, non-sclerosed margin and narrow zone of transition (Figure 1C-H).
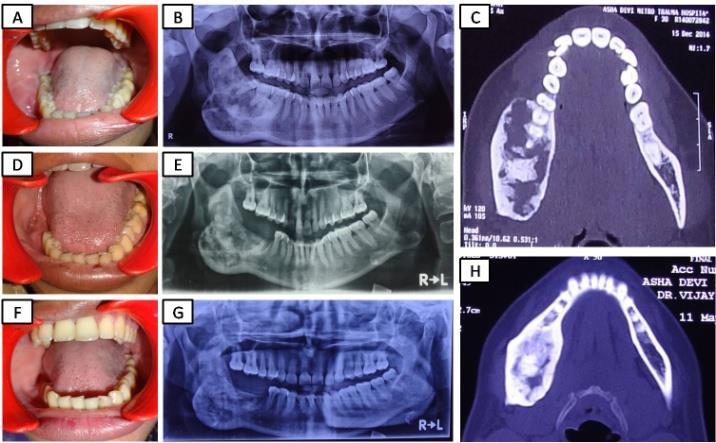
Figure 1: (A) Pre-op intraoral photograph shows vestibular obliteration. (B) Pre-op orthopantomogram shows huge multilocular lesion situated on right mandibular corpus, adjacent ramus and coronoid process. (C) Pre-op axial CT image shows expansile lytic lesion involving the right mandibular posterior region. (D) 4 months post-op intraoral photograph shows completed soft tissue wound healing. (E) 4 months post-op orthopantomogram image shows bone healing is going on and no sign of recurrence. (F) 15 months post-op intraoral photograph shows no sign of any recurrence. (G) 15 months post-op orthopantomogram image shows good bone healing and no sign of recurrence. (H) 15 months Post-op axial CT image shows reduced cortical expansion, uneventful bone regeneration and healing with no sign of recurrence. Incisional histopathologic examination revealed the presence of hypercellular connective tissue stroma, consisting of numerous mature and proliferating fibroblasts with few collagen fiber bundles ramifying in different direction. Few areas having dense collagen fiber bundle and newly formed osteoid along with presence of oval shape giant cells in moderate number. Numerous endothelial lined blood capillaries with areas of hemorrhage are also present with mild chronic inflammatory cell response (Figure 2). Overall clinical, radio-graphical and histopathological features are suggestive of aggressive central giant cell granuloma. Surgery was performed by using a set of standard Copyright© Vijay Kumar
technique with all standard precautions for blood borne pathogens. Under general anesthesia surgical site was exposed using ramus extended lower vestibular incision followed by extraction of all involved teeth and the perioperative findings were recorded. Of note, the lesion looks like deep brown, friable, cluster of abnormal bone, cortical expansion and uneven cortical thickening. After that’s, lesion was curetted carefully to preserve IAN, at that time profuse bleeding was encountered that suddenly stopped after complete removal of the disease tissues then all sharp edges were smoothed with a rotary instrument. Finally Carnoy’s solution was applied for five minutes followed by irrigation, partial primary closer of the wound and packed with iodoform gauze. During follow-up, the wound was evaluated and the packing was changed every 7 days until complete soft tissue healing was achieved. Finally enucleated tissue was sent for histopathologic examination that also conform initial diagnoses.
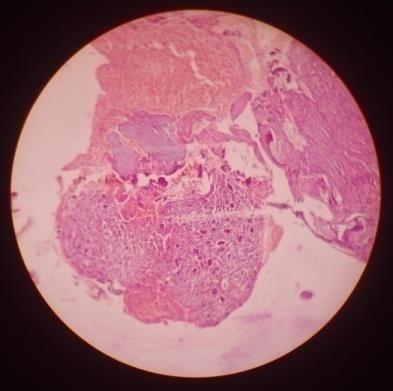
Figure 2: 10X H & E stained section reveals connective tissue stroma that consisting of (a) Fibroblasts & Collagen fiber bundles; (b) Osteoid areas; (c) Multiple giant cells; (d) Hemorrhagic areas. During first four initial clinical follow-up of wound evaluations, slight bleeding and pain was noted, but resolved after repeated wound packing with iodoform gauze. Clinically intraoral complete soft tissue healing was achieved at about 4 months (Figure 1D) and improved facial symmetry with no sign of any soft tissue recurrence noted during 15 months (Figure 1F) follow-up. Panoramic radiographs were taken at 4 months and 15 months that revealed bone regeneration was uneventful (Figure1E&G) and 15 months postoperative axial CT reveals well cortical thickening, resolution of cortical expansion, uneventful bone regeneration and healing (Figure 1H). Few sclerotic areas are also seen but no evidence of abnormal enhancement seen after IV contrast and extra osseous soft tissue component. In addition, there was Vijay Kumar. Postoperative evaluation of Conservative Surgical Approach on Central Giant Cell Granuloma of the Mandible: A case report.J Dental Sci 2016, 1(2): 000114.
uneventful secondary healing and bone regeneration with adequate facial symmetry and no evidence of recurrence recorded during 15 months postoperative follow-up of large aggressive CGCG.
Discussion
Management of large and aggressive forms of CGCG has always been a challenging problem for oral and maxillofacial surgeons due to their high recurrence rate (55% - 70%) [11, 14]. Therefore repetitive and extensive surgical procedures are required to resolve them. Resection alone may create severe postoperative functional and esthetic impairment that have adverse psychosocial consequences, particularly in young patients; while resection with reconstruction may prevent such adverse psychosocial consequences, it entails additional surgery and is prohibitively expensive [14, 15]. On other hand, recent advancement in the molecular biology in this form of lesion may provide evidence of by multi-phenotypic cell population that is in a dynamic state of trans-differentiation. This creates a distinguished phenotypic profile for each lesion at different time points, with changing proportions among the types of the lesional cells. Therefore each of these lesions should be considered individually in terms of biological behavior and treat accordingly [5]. Most authors agreed that large number of cases of aggressive CGCG treated by non surgical procedures (corticosteroids, calcitonin and α- interferon) showed failure of treatment and in future surgery required. Therefore, currently employed non surgical therapies would appear to be inadequate and need of a new therapeutic modality and operative strategies for aggressive CGCG [5, 14, 16, 17, 18, 19]. Molecular biology of aggressive CGCG indicated complete removal of disease tissue for uneventful postoperative soft and hard tissues healing because in the presence of multi-phenotypic cell population in its dynamic state of trans-differentiation [5]. Other studies conducted by Miloro, et al. [10], Vasconcelos, et al. [20] & Loyola, et al. [21] and reported seeding and incomplete surgical excision; more invasive nature and low osseous density respectively are the main reasons for rapid growth and high recurrence (72%) noted in aggressive CGCG after surgical curettage [3, 10, 20, 21, 22]. Therefore our aim is to manage the aggressive CGCG as quickly as possible with complete removal of disease tissues are the key for successful surgical management and uneventful long prognosis. In case of large aggressive CGCG, complete removal of disease tissues may created large surgical Copyright© Vijay Kumar
cavity that should undergo secondary wound healing rather than primary wound closer to reduce the risk of postoperative infection secondary to dead space [5, 15]. In sight of above things as well as my previous encouraging results for aggressive odontogenic cysts and tumour management by conservative surgical approach. Present case was also treated by conservative surgical approach such as surgical curettage, peripheral osteotomy, local application of carnoy’s solution followed by iodoform gauze packing till complete soft tissue healing and reported a fair degree of clinical and radio-graphical success in 15 months follow-up. Almost similar study was performed by Coskunses et al. [23] reported clinically and radiographically no recurrence after 7years of initial treatment [23]. In first four initial follow-up of wound evaluations, slight bleeding and pain was noted, but resolved after repeated wound packing with iodoform gauze and complete soft tissue healing was achieved at 4 months, the result was similar to my previous study [15]. On the other hand, Yildirim et al. [24] Hadziabdic et al. [25] & Kumar V [15] reported that radiographically complete bone healing was achieved in about 12 months, 16 months and 12 months in their respective studies. Similar result was achieved in this aggressive case of CGCG [15, 23, 24, 25]. On the other hand most authors agreed that recurrence in large aggressive CGCG after treatment were encountered within few months of initial treatment and minor recurrences were also manifested after 2 and more years of initial treatment. Shaminey SA et al. also reported recurrence after 23 years of initial treatment but site of recurrence was other than primary site [2, 5, 6, 9, 13, 14, 16, 21]. In addition, there was uneventful secondary healing and bone regeneration with adequate facial symmetry and no evidence of recurrence noted in present case treated by combined conservative surgical approach.
Study Design
Patients with non-perforated central giant cell granuloma, free of any serious systemic illness and patients interested to participate in the study are included.
Conclusion
The finding of this case report indicated that combined conservative surgical approach is effective for management of non-perforated large aggressive central giant cell granuloma of the mandible. In other hand we also noticed patient must retained its normal structural Vijay Kumar. Postoperative evaluation of Conservative Surgical Approach on Central Giant Cell Granuloma of the Mandible: A case report.J Dental Sci 2016, 1(2): 000114.
and functional integrity, less duration of hospital stay and antibiotic usage as well as good patient tolerence to this procedure. Thus, we conclude that above surgical procedure is a good conservative treatment option in future that has uneventful secondary healing with no recurrence during 15 months clinical and radio-graphical follow-up for management of non-perforated large aggressive central giant cell granuloma of the mandible.
References
-
Barnes L, Eveson JW, Reichart P, Sidransky D (2005) World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours. IARC Press Lyon 324.
-
Miloro M, Ghali GE, Larsen PE, Waite PD (2004) Peterson’s Principles of Oral and Maxillofacial Surgery. (2nd edn), BC Decker Inc. Hamilton London pp. 603:604.
-
Shaminey SA, Manoharan GVMG (2015) Central giant cell granuloma presenting as unilocular radiolucency in posterior mandible – A case report. Int J Cur Res Rev 7(21): 8-12.
-
Stavropoulos F, Katz J (2002) Central giant cell granulomas: A systemic review of the radiographic characteristics with the addition of 20 new cases. Dentomaxillofacial Radiology 31: 213-217.
-
Vered M, Buchner A, Dayan D (2008) Central giant cell granuloma of the jawbones – new insights into molecular biology with clinical implications on treatment approaches. Histol Histopathol 23(9): 1151-1160.
-
Bilodeau E, Chowdhury K, Collins B (2009) A case of recurrent multifocal central giant cell granulomas. Head and Neck Pathol 3(2): 174-178.
-
Noleto JW, Marchiori E, Sampaio RK, Irion KL, Collares FB (2007) Radiological and epidemiological aspects of central giant cell granuloma. Radiol Bras 40(3): 167-171.
-
Valentine JC, Nelson BL (2011) Central giant cell lesion. Head and Neck Pathol 5(4): 385-388.
-
Cossio PI, De-Fuentes RM, Carranza AC, Lagares DT, Perez JLG (2007) Recurrent central giant cell granuloma in the mandible: Surgical treatment and Copyright© Vijay Kumar dental implant restoration. Med Oral Patol Oral Cir Bucal 12(3): E229-E232.
-
Miloro M, Quinn PD (1995) Synchronous central giant cell lesions of the jaws: Report of a case and review of the literature. J Oral Maxillofac Surg 53(11): 1350- 1355.
-
Hongal BP, Joshi P, Kulkarni V, Baldawa P (2015) Central giant cell granulomas of the jaws: A review of the literature with its emphasis on differential diagnosis on related lesions. Int J Contem Dent Med Rev Article ID 010115:1-4.
-
Bojan A, Christy W, Chanmougananda S, Ashokan K (2012) Central giant cell granuloma of the jaw in early childhood: Surgical and non-surgical management. Journal of Advanced Oral Research 3(2): 37-42.
-
Melrose RJ Central giant cell granuloma. Oral Pathology associates, INC. Tissue Diagnosis and consultation for the health care professional.
-
Al-Jandan B (2015) Combined management of large aggressive central giant cell granuloma of the mandible: A case report. The Saudi Journal for Dental Research 6(2): 157-160.
-
Kumar V (2015) Conservative surgical approach to aggressive benign odontogenic neoplasm: A report of three cases. J Korean Assoc Oral Maxillofac Surg 41(1): 37-42.
-
Gerzanic L, Schultes G, Karcher H, Zebedin D (2013) Central giant cell granuloma resistant to calcitonin nasal spray: A case Report. Anaplastology 2(5): 119.
-
Graham RM, Foster MF, Richardson D (2008) An unusual presentation of a central giant cell granuloma and initial treatment with intralesional steroids: A Vijay Kumar. Postoperative evaluation of Conservative Surgical Approach on Central Giant Cell Granuloma of the Mandible: A case report.J Dental Sci 2016, 1(2): 000114. case report and review of the literature. JOHCD 2(3): 65-69.
-
Yazici N, Yalcin B, Yilmaz T, Akyuz C, Oguz KK, et al. (2006) Surgery and calciton in therapy in childhood central giant cell granuloma. International Journal of Pediatric Otorhinolaryngology Extra1: 297-300.
-
Sezer B, Koyuncu B, Gomel M, Gunbay T (2005) Intralesional corticosteroid injection for central giant cell granuloma: A case report and review of literature. The Turkish Journal of Pediatrics 47(1): 75-81.
-
Vasconcelos RG, Vasconcelos MG, Queiroz LMG (2013) Peripheral and central giant cell lesions: etiology, origin of giant cells, diagnosis and treatment. J Bras Patol Med Lab 49(6): 446-452.
-
Loyola AM, Fernandes AV, Magalhaes AO, Moreira MR (2005) The central giant cell granuloma in childhood: clinical case report. The Journal of Clinical Pediatric Dentistry 29(3): 259-262.
-
Kalsi HS, Thakkar V, Kharkar V (2014) Surgical treatment and reconstruction for central giant cell granuloma of mandible- Case report and literature review. IOSR-JDMS 13(8): 23-27.
-
Coskunses FM, Suer BT, Ozgul O, Kocyigit ID, Kartal Y (2014) preserving of a tooth related with central giant cell granuloma with non-invasive curettage: 7 years follow-up case report. OHDM 13(3): 634-637.
-
Yildirim G, Ataoglu H, Kalayci A, Ozkan BT, Kucuk K, et al. (2010) Conservative treatment protocol for Keratocystic odontogenic tumour: a follow-up study of 3 cases. J Oral Maxillofac Res 1(3): e7.
-
Hadziabdic N, Sulejmanagic H, Selimovic E, Sulejmanagic N (2011) Therapeutic approach to large jaw cysts. Health Med 5: 1793-1799. Copyright© Vijay Kumar
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells