Salvaging Compromised Natural Teeth with Tooth Supported Telescopic Over Denture: A Case Report
Background: Telescopic dentures gained popularity in late 1980’s as an alternative to conventional complete dentures as well as conventional over dentures, due to the preservation of periodontium as well as the residual bone. A significant advantage of better retention, stability and support can be obtained with the remaining natural teeth. The residual ridge resorption is decreased significantly as a result of conversion of compressive forces into tensile forces through periodontal ligament, distributing even stresses. Materials and Methods: After the preparation of the abutments, a polyvinyl siloxane elastomer impression was made and the primary copings were fabricated on the subsequent cast obtained. After evaluating the fit of the primary copings on the abutments, they were cemented and an impression of the cemented primary copings was made for the fabrication of metal framework along with secondary copings which was included in the prosthesis. Conclusion: Tooth-supported, removable over dentures with telescopic crowns along with metal framework are a good alternative to the conventional removable dentures. These provide better occlusion, retention, stability, support, decrease in the forward sliding of the prosthesis and better control of the mandibular movements because of the proprioception feedback which increases the chewing efficiency and phonetics, as compared to the conventional complete dentures and over dentures.
Introduction
Natural teeth should be saved only if they can be made comfortably functional or if they can, in a modified state, contribute to the function of the masticatory system. In the latter instance, natural teeth may be useful in support of complete dentures since many residual ridges are poor recipients for either complete or implant dentures. In these instances, the use of the telescopic denture may be indicated [1]. According to GPT 8, a telescopic over denture is a removable partial denture or complete denture that covers and rests on one or more remaining natural teeth, the roots of natural teeth, and/or dental implants; a prosthesis that covers and is partially supported by natural teeth, natural tooth roots, and/or dental implants-also called overlay denture, overlay prosthesis, superimposed prosthesis. Telescopic dentures consist of an inner or primary telescopic coping which is permanently cemented to an abutment and an outer or secondary telescopic coping which is attached to the prosthesis. These copings protect the abutment from dental caries and thermal irritations and also provide retention and stabilization of the secondary coping. The secondary coping engages the primary copings to form a telescopic unit and it provides retention and stability to the prosthesis [2, 3]. Telescopic dentures do not preclude the use of removable partial dentures where indicated. Selection is based on the nature of the support of denture-bearing areas and stability of remaining teeth. Through a combination of passive ridge support and full-coverage retainers placed on the remaining natural teeth, the telescopic denture is constructed [4, 5, 6, 7]. The teeth act as stabilizers and do not provide retention for the denture. The teeth prevent lateral displacement of the denture. On the other hand, the passive relationship of the denture to the teeth may provide an increase in the longevity of the abutment teeth. The principles of vertical loading of teeth and resistance of denture bases to rotation have been described in other articles [6, 7, 8]. Proper periodontal therapy must be instituted to establish a sound soft tissue environment for the abutment teeth for telescopic dentures. The patient must be instructed in oral hygiene specifically oriented to the remaining teeth. Proper care is facilitated by judicious cleansing and massaging of the marginal surfaces with pipe cleaners upon removal of the dentures.
Clinical Case Report
A 62-years old male reported the Department of Prosthodontics and Crown and Bridge with a chief complaint of difficulty in mastication due to loss of mandibular teeth in the lower left and right back region. The patient had major complaints of difficulty in chewing due to the missing posterior teeth and poor aesthetics due to the loss of teeth. On intra-oral examination it was observed that teeth remaining in the mandibular arch were 33,34,37,43 and 44 (Figure 1A). Out of the remaining teeth, 44 was grade II mobile and had a poor prognosis. The radiographic examination revealed that there was no periapical pathology. The rest of the teeth were periodontally sound, with a grade II mobility w.r.t 44 only. It was decided to fabricate a mandibular tooth- supported telescopic over denture after extraction of 44. After the intentional root canal treatment of the abutments (Figure 1B), they were prepared with a tapered round end diamond rotary bur with a chamfer finish line for the primary coping. The finish line had to be prepared subgingivally. The long abutments had to be prepared with tapered walls (2-5º) and the short abutments had to be prepared with parallel walls. After the preparation of the abutments, the impression was made by using a polyvinyl siloxane elastomeric impression material (monophase) by a single mix single step technique. The impression was poured into a die material to obtain the cast, on which the primary copings were fabricated. The fit of the primary coping was evaluated in the patient’s mouth, after which they were cemented on the abutments with glass ionomer cement (Figure 2). Another impression was made by a single mix single step technique (monophase) after the cementation of the primary copings, (Figure 3) by using a custom acrylic resin tray to obtain a cast on which a metal framework along with secondary copings was fabricated (Figures 4-8). The fit of the metal framework along with secondary copings over the primary copings was evaluated in the patient’s mouth. The frictional contact between the primary and secondary copings helped in the retention of the prosthesis.

Figure 1A: Pre-op intra-oral view- abutments.
Figure 1B: Radiographs showing intentional root canal treatment w.r.t. 33, 34 and 44.




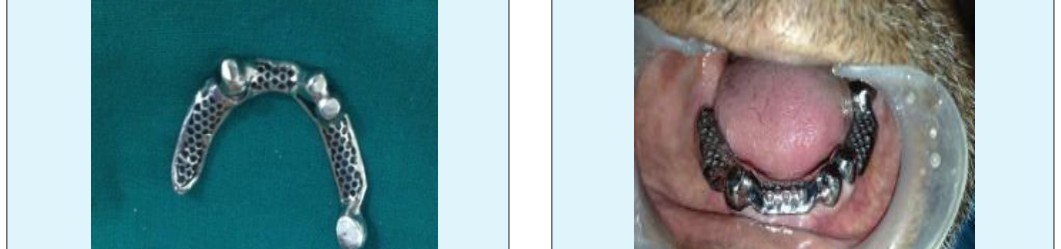

Figure 8: Intra-oral Trial of Metal Framework. The metal framework along with secondary copings had to be placed on the master cast, it had to be covered with wax and the trial denture base had to be fabricated with chemically cured acrylic resins after applying separating media over the master cast. The placement of the wax over the secondary copings helped in the easy separation of the abutment copings from the trial denture base at the time of the dewaxing. Occlusion rims were also fabricated over the trial denture base. The artificial teeth were selected and arranged on the record bases for a trial denture arrangement and they were evaluated intraorally for phonetics, aesthetics, occlusal vertical dimension and centric relation. After the wax up, the dentures were processed, finished, polished and delivered to the patient (Figures 9-11). The patient was scheduled for follow-up visits every 3 months and he reported no complaints during the 2 years of follow-up.



Discussion
It is a documented fact that after the loss of the teeth, the residual alveolar ridge undergoes rapid loss in all dimensions. The residual ridge resorption (RRR) is stated to be rapid, progressive, irreversible and inevitable, and has been well observed and documented in the literature. It is equally well observed that bone is maintained around long-standing teeth and implants. Retaining teeth as over denture abutments seems to slow the rate of alveolar resorption. The physiologic objective is to provide for the tensile stimulation of as many of the oblique periodontal fibers as possible and the end result is the deposition of more bundle bone followed by concomitant decrease in abutment mobility [1]. The telescopic over denture system used in this case in mandibular arch revealed a long-lasting usefulness in the prosthetic treatment of the patient with reduced dentition. Many authors have also observed positive results of prosthetic treatment with telescopic dentures in patients with reduced dentition. There are many advantages of telescopic crowns, like axial load of the tooth and full covering of the abutment (on the contrary to clasps), which may reduce the tilting forces with their negative influence on the abutment supporting tissues. The axial forces stimulate periodontal tissues and alveolar bone. They also provide indirect splinting influence, easy oral hygiene maintenance and easy ways of repair [2]. The metal framework incorporated into the final prosthesis served major beneficial advantage of providing fracture toughness to the prosthesis, better coverage and stability of the prosthesis. Interarch space plays a vital role in determining the success of a telescopic prosthesis and may as well require an intentional endodontic therapy for the abutments. This space requirement however varies according to the primary and secondary copings, denture base thickness, the arrangement of the teeth and interocclusal gap. An even number of the abutments in each quadrant is pre-requisite for stress distribution and for increased retention and stability of the prosthesis. The interocclusal gap/ interarch distance should be ≥ 10 mm, in order to have sufficient space for the copings, denture base, teeth placement and adequate closest speaking space [9]. The contours and the degree of taper of the outer aspect of the primary coping determine the path of insertion and the amount of retention of the prosthesis. The retention varies inversely with the taper of the coping. Even copings of minimal taper (approximately 5 degrees) require a height of about 4mm to achieve a significant retention [3, 6]. The height and size of the inner coping also influence the retention. The essential requirements for the long service of the telescopic prosthesis are, to provide adequate height of the vertical walls (at least 4mm), sufficient thickness of the copings (never less than 0.7mm for each casting) and a taper of around 6 degree. Adaptation to the conventional removable complete dentures is a complex learning process. Patients who have originally adapted to wearing complete dentures may become maladaptive with time, due to the continual residual ridge resorption, intra oral physiological changes and the development of an altered muscle pattern. It has been found that the telescopic dentures which are supported by the roots of natural teeth have more predictable prosthodontic outcomes because of increased support, stability and retention and decrease in rate of the residual ridge resorption. Complete denture fabrication for maladaptive elderly patients becomes difficult. Therefore, they are the group of patients who will benefit most with telescopic dentures. Overdentures which are supported and/or retained with a few remaining teeth or implants can be a predictable treatment that will fulfill most of the demands of the elderly denture patients [10].
Conclusion
In the above stated case, there were many other options which could have been used as a way of alternative prosthodontic rehabilitation. As Tooth- supported over dentures present with an advantage of improved proprioception along with an increased stability and retention, it proved to be beneficial for the patient as well. Inclusion of telescopic crowns along with metal framework provided exclusive coverage for the abutments and thereby increasing the longevity of both abutments as well as the prosthesis. Thus, it can be stated with confidence that keeping in mind all the regressive changes that the body undergoes after loss of teeth and supporting structures, telescopic prostheses are a good alternative to the conventional removable dentures. These provide better occlusion, retention, stability, support, decrease in the forward sliding of the prosthesis and better control of the mandibular movements because of the proprioception feedback which increases the chewing efficiency and phonetics, as compared to the conventional complete dentures and over dentures.
References
-
Morton LP (1973) Telescope Dentures. J Prosthet Dent 29(2): 151-156.
-
Langer Y, Langer A (2000) Tooth-supported telescopic prostheses in compromised dentitions: A clinical report. J Prosthetic Dent 84 (2): 129-132.
-
Wenz HJ, Lehmann KM (1998) A telescopic crown concept for the restoration of the partially endentulous arch: the Marburg double crown system. Int J Prosthodont 11(6): 541-550.
-
Langer A (1981) Telescope retainers for removable partial dentures. J Prosthet Dent 45(1): 37-43.
-
Laufer BZ, Gross M (1998) Splinting osseointegrated implants and natural teeth in the rehabilitation of partially edentulous patients. Part II: principles and applications. J Oral Rehabil 25(1): 69-80.
-
Besimo C, Graber G (1994) A new concept of over dentures with telescope crowns on osseointegrated implants. Int J Periodontics Restorative Dent 14(6): 486-495.
-
Langer A (1980) Telescope retainers and their clinical application. J Prosthet Dent 44(5): 516-522.
-
Preiskel HW (1996) Over denture made easy-a guide to implant and root supported prostheses 61.
-
Bergman B, Ericson Á, Molin M (1996) Long-term clinical results after treatment with conical crown- retained dentures. Int J Prosthodont 9(6): 533-538.
-
Kunwarjeet S, Nidhi G (2012) Telescopic Denture-A Treatment Modality for Minimizing the Conventional Removable Complete Denture Problems: A Case Report. J Clinical Diagnostic Research 6(6): 1112- 1116.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells