Hemisection in an Era of Implants
Over the last century, the field of dentistry has grown by leaps & bounds. Better and more conservative treatment modalities have led to increased expectations of patients. Mandibular first molars are one of the most commonly extracted teeth due to dental caries & periodontal disease. Hemisection of a mandibular molar can be a suitable treatment option if one of the roots is healthy. This clinical report describes a case wherein hemisection of a decayed mandibular molar followed by prosthetic rehabilitation yielded a satisfactory result.
Munishwar Singh* and Satish Chandar R
*Corresponding author: Lt Col (Dr.) Munishwar Singh, Graded Specialist
(Periodontology), 201 Military Dental Centre, C/o 99 APO, Pin: 981027, India, Email:
msmalhi@yahoo.com molar followed by prosthetic rehabilitation yielded a satisfactory result.
Keywords: Hemisection; Furcation involvement; Prosthetic rehabilitation
Introduction
Advances in dentistry and an increased desire of patients to save teeth have encouraged techniques for conservation of teeth that would have earlier been planned for extraction. The therapeutic procedures for conserving the teeth vary in complexity due to various periodontal, endodontic and restorative factors. The mandibular first molars have a wide pericemental area and are important from the standpoint of occlusion. Despite their importance, they are the most commonly extracted teeth due to dental caries & periodontal disease. Alternatively, if the dental caries is restricted to one root then a hemisection procedure may be possible. Hemisection denotes sectioning of a mandibular molar into two halves followed by the removal or separation of the diseased root with its accompanying crown portion [1]. The retained root is endodontically treated such that the furcation area is made self-cleansable followed by extra coronal restoration. Hemisection is a conservative option with an acceptable prognosis.
A 44-year-old male patient visited the dental OPD with a chief complaint of pain and pus discharge from his right lower back tooth region from the last ten days. Pain was dull aching and intermittent in nature that aggravated on chewing. On examination, patient had a fair oral hygiene with caries in mandibular right first molar i.e. 46. Clinically, class III gingival recession and on probing a 15mm periodontal pocket probing depth was observed with relation to distal root of 46. Also, the tooth was grade II mobile and sensitive to percussion (Figure 1). Intra-oral periapical radiograph of the tooth confirmed carious lesion, grade III furcation involvement and a radiolucent area around distal root confirming endoperio lesion in 46 (Figure 2). Treatment options including extraction of 46 followed by placement of dental implant, fixed partial denture or removable partial denture were explained. The patient did not wish to have the tooth removed, so a conservative option of root canal treatment with subsequent hemisection was planned in this case.
Accordingly, access cavity was prepared, working root canal length determined followed by bio mechanical preparation of root canals using a step back technique. The root canal obturation was achieved by lateral condensation (Figure 3). Patient was recalled for surgical intervention. After appropriate local anesthesia, a crevicular incision was made and a full thickness mucoperiosteal flap was elevated to provide adequate access for visualization and instrumentation (Figure 4). A long shank tapered fissure diamond point was used to make vertical cut towards the bifurcation area taking care that bone and adjacent was not traumatized while removing distal root. The distal root was then extracted and platelet rich plasma, bioactive glass bone graft (Perioglass, US Biomaterials Corp, FL, USA) and bioresorbable collagen membrane (PeriocolTM, Eucare Pharmaceuticals Private Limited) were used for socket preservation of the distal extraction socket (Figure 5). The furcation area was trimmed to ensure that no residual debris was present that could cause further periodontal irritation. The remaining tooth was restored as premolar with completion of core build-up, the occlusal table was minimized to redirect the forces along the long axis of the retained mesial root. Oral hygiene reinforcement was carried out and after satisfactory tissue healing, it was followed by prosthodontic rehabilitation (Figures 6 & 7).
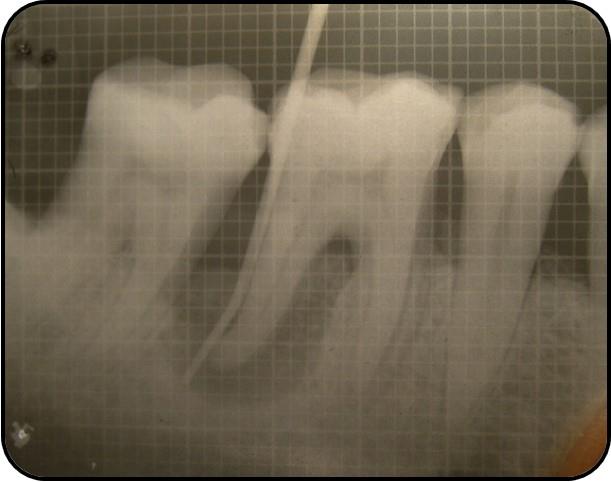
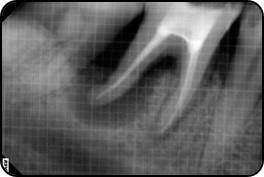



Figure 5 A, B & C: Socket Preservation of distal extraction socket with PRP, Bioactive glass bone graft & Bioresorbable collagen membrane.
Figure 6 A & B: Post operative evaluation.
Figure 7 A, B & C: Prosthodontic Rehabilitation.
Discussion
The management and long-term retention of a mandibular molar exhibiting furcal invasion has always been a challenge for the treating clinician. Earlier the cases of furcal caries, large perforations and severe bone loss involving either of the surfaces of the root were considered untreatable and planned for extraction. A guiding principle should be to try and maintain what is present [2]. Hemisection represents a form of conservative dentistry, aiming to preserve as much tooth structure as possible rather than extraction of whole tooth [3]. It involves removal of significantly compromised root structure and the associated coronal structure through deliberate excision. It differs from bicuspidization wherein the molar roots are separated in the furcation area without removal of any root. Before selecting a tooth for hemisection, the oral hygiene status of the patient, caries index, medical status, access to furcation area as well as good bone support for the remaining root needs to be considered. It is imperative that this procedure be performed after proper selection of cases based on periodontal, endodontic & restorative assessment [4]. From a periodontal perspective, this procedure is indicated if severe bone loss involves only one root or involvement of class III furcation that could produce a stable root after hemisection. Extensive exposure of roots because of dehiscence, unfavourable proximity of roots of adjacent teeth, prevention of maintenance of adequate oral hygiene in proximal areas are other indications for excision of root. From an endodontic and restorative perspective, hemisection is useful in cases with failure of an abutment within a fixed prosthesis, provided a tooth portion could be retained to function as an abutment for the prosthesis, perforation of tooth through the pulp chamber, if pulp canal of one of endodontically involved tooth cannot be instrumented, external root resorption, trauma, vertical root fracture or any severe destructive process confined to a single root of a multirooted tooth. Contraindications include presence of a strong adjacent tooth adjacent to the proposed hemisection, which could act as an abutment to a prosthesis, inoperable canals in root to be retained as well as fusion or proximity of roots that may prevent their separation [1]. Special care needs to be taken while reshaping of root surfaces as reshaped root surfaces in the furcation area are more prone to caries so no lisp/ledges should be left that may further lead to caries in addition to acting as a nidus for bacteria. Root fracture is the main cause of failure after hemisection, so necessary occlusal adjustments along with proper prosthodontic rehabilitation needs to be performed for better prognosis [5]. For this patient, hemisection was selected as treatment despite implant therapy also being offered to him as the patient couldn't afford dental implant. The distal root of 46 was resected in this case because of the severe bone loss in distal root. The literature on distal root resection is scanty as more often this root is retained and mesial root removed as, the distal root is broader and straighter, making it more suitable for an abutment [6]. The mesial root contains a longitudinal groove, which decreases its surface area and contraindicates the use of posts [4]. Implant therapy is a predictable option with good functionality [7] but in this case the patient chose an alternative treatment because of financial considerations and the desire to save the tooth. After satisfactory healing the definitive prosthodontic treatment was carried out with a fixed partial denture. The smaller size of occlusal tables, under-contouring of the embrasure spaces and ensuring that the crown margin encompasses the furcation are all factors in the high success rates observed with hemisection therapy [8].
Conclusion
With the advent of the implant systems along with the aggressive marketing & finances involved, more and more clinicians are going the non-conservative way. The option of hemisection must be offered to the patients as it is a reliable and predictable procedure with excellent prognosis provided the proper case selection and prosthodontic rehabilitation is relative to the occlusal and periodontal needs of the patient. Hemisection may be suitable alternative to extraction followed by implant therapy and should be discussed with the patients during the consideration of treatment options.
Conflict of Interest
The authors declared that this case has no personal and financial relationship with any corporate affiliations or any other organizations.
References
-
Weine FS (1996) Endodontic Therapy, Mosby, St Louis, Mo, USA, 5th (Edn,).
-
Nowakowski AT, Serebnitski A, Pesun IJ (2010) Hemisection as a treatment option: a case report. Oral Health 100(3): 83-89.
-
Kost WJ, Stakiw JE (1991) Root amputation and hemisection. J Can Dent Assoc 57(1): 42-45.
-
Saad MN, Moreno J, Crawford C (2009) Hemisection as an alternative treatment for decayed multirooted terminal abutment: A case report. J Can Dent Assoc 75(5): 387-390.
-
Kryshtalskyj E (1986) Root amputation and hemisection. Indication, technique and restoration. J Can Dent Assoc 52(4): 307-308.
-
Rosenstiel SF, Land MF, Fujimoto J (1995) Contemporary fixed prosthodontics. 2nd (Ed.), St. Louis: Mosby Year Book, Inc.
-
Bashutski JD, Wang HL (2007) Common implant esthetic complications. Implant Dent 16(4): 340-348.
-
Rapoport RH, Deep P (2003) Traumatic hemisection and restoration of a maxillary first premolar: a case report. Gen Dent 51(4): 340-342.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells