Awareness and Knowledge of Oral Cancer among Dental Patients in Aseer Region, Saudi Arabia: A Questionnaire-Based Survey
Introduction: Despite advances in the diagnosis and treatment of oral cancer, cases diagnosed at an early stage is less than 50%, reasons being lack of information about etiology, signs and symptoms of oral cancer among the population. Objective: The objective was to assess the level of awareness and knowledge about oral cancer among dental patients, to correlate the knowledge levels with demographic factors, and to know the habit history of the population in Aseer region of Saudi Arabia. Materials and methods: A cross-sectional questionnaire-based survey was conducted on 775 patients visiting King Khalid University-College of Dentistry in Saudi Arabia. Questionnaire probed demographic details, general information, awareness and knowledge on oral cancer. Results: 50.3% were males and 49.7% females.18.1% were smokers. Participants agreed that tobacco-67.5%, alcohol-36.5%, infection - 23.6%, 48.3%- poor oral hygiene, old age- 7.7% and close contact- 9.3% to be the main cause of oral cancer. Among the patients with improved oral hygiene frequency, only 24.3% were aware of oral cancer Conclusion: General lack of awareness and knowledge on oral cancer was reflected among patients visiting King Khalid University-College of Dentistry in Saudi Arabia. It substantiates the need for robust oral health planning for patients visiting the hospital.
Alqahtani2, Eman Khalid Abdullah2, Saja Abdulaziz Al Thubait2 and Ghaida Salman Ali Asiri2
Dentistry, Saudi Arabia
information, awareness and knowledge on oral cancer.
visiting the hospital.
Keywords: Aseer region; Saudi Arabia; Oral cancer; King Khalid University
Awareness and Knowledge of Oral Cancer among Dental Patients in Aseer Region, Saudi Arabia: A Questionnaire-Based Survey J Dental Sci
Abbreviations: HPV: Human Papillomavirus; TSNA: Tobacco-Specific Nitrosamines.
Introduction
Cancer is one of the major threats to public health in the developed world as well as in the developing world. In developed countries, cancer is the second most common cause of death. Oral carcinoma is one of the 10 most common cancers worldwide and one among topmost cancers in India [1, 2, 3]. Tobacco consumption, unhealthy diet, physical inactivity, and infections are the most common causes of cancer. The risk for development of oral cancer increases when tobacco is used in combination with alcohol or areca nut.
Oral cancer affects the anterior tongue, cheek, floor of mouth, gingiva or any other part of the oral cavity. The most common risk factors responsible for oral cancer are chemical factors like tobacco and alcohol, oro-dental factors, biological factors like human papillomavirus (HPV), syphilis, dietary deficiencies, chronic candidiasis and viruses, genetic predispositions to name a few [4]. Oral carcinogenesis is a multistep process in which genetic events leading to the disruption of the normal regulatory pathways such as functions of oncogenes and tumor suppressor genes. Exposure to tobacco increases exposure to carcinogenic tobacco-specific nitrosamines (TSNA) and to nitrosamines derived from areca nut alkaloids. The family history of head and neck cancer is a significant risk factor. Genetic alterations involving the tumor suppressor genes p16 and p53 are frequently observed in head and neck tumors [5]. According to the World Health Report 2004, 7.1 million deaths in 2003 were due to cancer and it is estimated the overall new cases will rise by 50% in the next 20 years. The prevalence of oral cancer is particularly high among men. It is the eighth most common cancer worldwide. Incidence rates for oral cancer vary in men from 1 to 10 cases per 100 000 population in many countries. It has been estimated that 43% of cancer deaths worldwide are due to tobacco, unhealthy diet, physical inactivity, and infections. The chewing of several tobacco-like substances such as Shammaand qat, prevalent mainly in the Southern region particularly the Jizan area and neighboring Yemen, may contribute to the high frequency of oral cancer [3].
Since oral examination and regular screening for oral cancer in those with the family history of cancer or those with habits of alcohol and tobacco consumption is helpful in early detection and treatment of oral cancer, oral cancer to a large extent is a preventable malignant disorder. The prognosis of oral cancer is poor with lowest survival rates of < 50% within a 5 year period. In spite of advances in the diagnosis and treatment of oral cancer, the proportion of oral cancer cases diagnosed at an early and localized stage is still <50%. Even though, recent advances in the detection and treatment of cancer, visual accessibility of the oral mucosa, and the scientific knowledge on cancer risk factors carry a low survival rate (near 50%). One of the main reasons may be a lack of information about the causes and knowledge of the signs and symptoms of oral cancer among the population [6].
Hence this study was aimed at obtaining the information on awareness and knowledge about oral cancer among the dental patients visiting King Khalid University-College of Dentistry in Saudi Arabia.
Methodology
A cross-sectional questionnaire-based survey was conducted on 775 patients visiting King Khalid University-College of Dentistry in Saudi Arabia. The intention was to record demographic status, knowledge, and awareness on oral cancer, preventive measures and screening. The study was conducted after obtaining clearance from Institutional Ethics Committee of King Khalid University-College of Dentistry and a written informed consent from subjects. The study was conducted for the duration of 6 months.
The questionnaire was divided into two sections. The first section included demographic questionnaire regarding gender, age, education level, habits of smoking, habits of tobacco chewing, alcohol use, dental visits, and lifestyle. The section two questionnaires were targeted towards awareness among dental patients on screening and preventive measures against oral cancers. There was no stipulated time given to complete the questionnaire and most of the participants completed it in less than 15 minutes.
The data collected were then tabulated and demographic data were analyzed and represented as mean + SD, while the data from questionnaire related to awareness about oral cancer were analyzed and presented as the percentage.
Results
The study was carried out among 775 patients visiting King Khalid University-College of Dentistry. Out of these patients, 92.9% (n=720) lived in urban area and included
50.3% (n=390) males and 49.7% (n= 385) females with
average age of 31.81±10.33 (in years). The patients with
$$ \text{postgraduate qualification were} 53.5 \% \quad (n = 415), $$
university-level education: 29% (n=225), primary: 1.2%
and secondary level education: 16.3% respectively (Table
1).
chewers. The study participants agreed that tobacco- 67.5%, alcohol- 36.5%, infection - 23.6%, 48.3%- poor oral hygiene, old age- 7.7% and close contact- 9.3% to be the main cause of oral cancer. Around 67.2% of postgraduates, 74.7%with university education and around 55% with secondary and primary education agreed that tobacco is the main cause of cancer. 36.5% of those with smoking habit agree that alcohol and 7.7% with tobacco chewing habit believe old age is the cause of oral cancer (Table 1).
Out of the total population, 76.9% were non-smokers and 18.1% smokers while the habit of tobacco chewing was observed in 6.5% and 91.4% were tobacco not
| Responses - Expressed as - n (%) | Yes | |||||||
|---|---|---|---|---|---|---|---|---|
| Question related to awareness | ||||||||
| No | 629 (81.2) | 146 (18.8) | ||||||
| Q.1 | Have you heard about oral cancer screening? | No | Yes | |||||
| No | Not Aware | |||||||
| Q.2 | Have you received an oral cancer examination within the last year? | 763 (98.5) | 5 (0.6) | |||||
| Q.3 | Do you think that detection of oral cancer in early stages could increase the success of the treatment? | 11 (1.4) | 694 (89.5) | |||||
| Q.4 | Do you think that changing the lifestyle could reduce the risk of cancer of the mouth? | 42 (5.4) | 602 (77.7) | |||||
| Agree | Don't Know | Disagree | ||||||
| Q.5 | Do you think that 'having oral cancer is a matter of luck and it' | 85 (11) | 426 (55) | |||||
| Q 1 | Do you think that oral cancer a contagious disease? | Don't Know | Disagree | |||||
| Q 1 | 327 (42.2) | 373 (48.1) | ||||||
| Q 2 | What reason do you think for oral cancer? | |||||||
| Tobacco | Alcohol | Dental Treatment | Reduced oral hygiene | Infections in the teeth | Reduced intake of fruit and vegetables | Sun exposure | Old age | |
| 523 (67.5) | 283 (36.5) | 66 (8.5) | 374 (48.3) | 183 (23.6) | 63 (8.1) | 49 (6.3) | ||
| Q 3 | What are the symptoms do you think of oral cancer? | |||||||
| Ulcer that does not heal | Lump or tissue overgrow | Difficulty in swallowing | Abscess, boil, or infection | Persistent white or red patch | Bleeding from Lesions | Don't Know | ||
| 327 (42.2) | 325 (41.9) | 151 (19.5) | 354 (45.7) | 242 (31.2) | 99 (12.8) | 18 (2.3) | ||
Table 1: Question related to awareness.
Around 55% of the population with tobacco chewing habit disagreed with the statement that oral cancer is a matter of luck and there is nothing we can do to avoid it (Table 2). It was also observed during the study that 45.7%believed oral cancer to be a boil, infection or abscess, 42.2% believed it to be an ulcer that does not heal and 41.9% thought it was tissue overgrowth or lump (Table 2). Patients with less than 3 times of dental visits were 75%, 3-5 times visit was seen among 15% and more than 5 times visit in 10.1% of the population. Oral hygiene frequency of > 1/ day was observed in 52.1% and 47.9% showed < 1 /day. It was observed that only 12.9% of those with oral hygiene frequency of less than 1 time daily and 24.3% of those with oral hygiene frequency of more than 1 time daily were aware of oral cancer. 86.3% of those with the oral frequency of less than one time daily early stages could increase the success of the treatment (Table 2).
Inferential Statistics of Question evaluating awareness Question Gender Education Residence Smoking Tobacco Alcohol Fruits Have you heard about
0.96 (0.30)
0.81 (0.05)
0.42 (1.72)
0.008€(7.21) Q.1
oral cancer screening?
Have you received an
0.46 (5.62)
0.001€ (15.03)
0.51 (3.24) oral cancer examination
0.38 (1.91) Q.2
within the last year?
Do you think
that detection of oral cancer
0.12 (7.20)
0.77 (3.28)
0.41 (1.76) in early stages could increase the
0.31 (2.30) Q.3
success of the treatment?
Do you think
that changing the
0.01* (16.10)
0.06 (5.53)
0.80 (1.60) lifestyle could reduce
0.98 (0.03) Q.4
the risk of cancer of the mouth?
Do you think
that ‘having oral cancer
0.37 (1.95)
0.51 (3.26) is a matter of luck and
0.02*(7.74)
0.000¶(27.45) Q.5
there is nothing we can do to avoid it’ Inferential Statistics of Question evaluating Knowledge Question Gender Education ResidenceSmoking Tobacco Fruits & Do you think that oral
0.09 (7.99)
0.29 (2.47)
0.04* (13.16)
0.08 (4.87) cancer a contagious disease?
0.97 (0.06)
0.33 (2.21)
0.68 (0.17)
0.44 (1.60)
0.000¶(16.20)
0.18 (6.14)
0.15 (6.63)
0.004€ (11.15)
0.48 (3.45)
0.12 (4.16)
0.28 (5.05)
0.01* (13.01)
0.47 (1.49)
0.21 (5.85)
0.007€ (9.82)
0.19 (6.09)
0.77 (0.51)
0.41 (3.92)
0.05 (5.73)
0.18 (6.27)
0.04* (9.90)
0.03* (10.54)
0.29 (2.44)
0.37 (4.25)
0.02* (7.49) veg Dental Visit Oral Hygiene
0.58 (2.86)
0.31 (4.77)
0.82 (0.37)
0.14 (6.89)
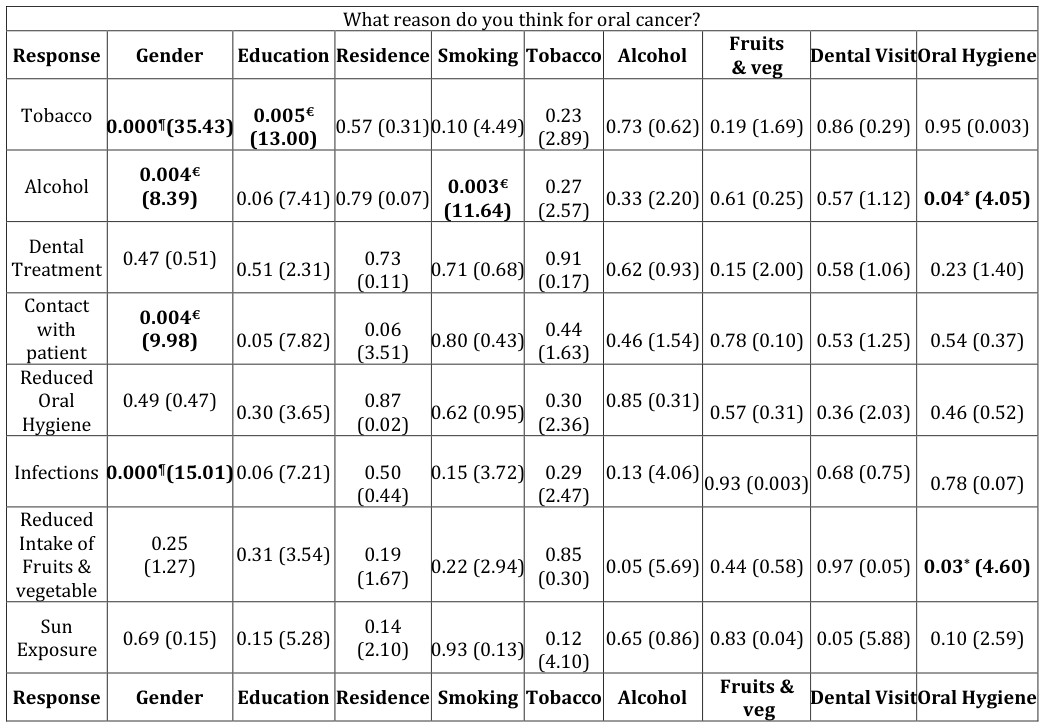
- *= p value =p<0.05;
- Chi Square test is applied with 95% confidence interval
- Significant results are shown in Bold with the following special charters and different p value
- *= p value =p<0.05; €= p value =p<0.01; ¶= p value= p<0.001
Table 2: Comparative Evaluation of Questions between various Parameters Expressed as – p value (Chi square Variate).
94.3% of subjects who consumed more than 5 units of fruits or vegetables per day had received an oral cancer examination within the last year. 5.7% of patients consuming more than 5 units per day believed that bleeding from infection is an important symptom of oral cancer. 15.1% with oral hygiene frequency of 1 time daily and 10.2% with oral hygiene frequency of less than 1 time While assessing data on awareness and preventive measures undertaken, only 47% heard of oral cancers from several sources and 55% believed that having oral cancer can be avoided and is not a matter of luck. And it was also observed that 22.6% of men and 15.1% of women were not aware of oral cancer. Of the total sample size, 81.2% had never heard of oral cancer screening out of which 77.4% were males and 84.9% were females. It was also observed that 98.5% of which 98.9% of urban residents and 92.7% of suburban residents had never received oral cancer examination within the last year (Table 2).
Further, during the study, it was observed that 89.5% were aware that detection of oral cancer in early stages could increase the success of the treatment and 77.7% were aware that lifestyle modification could reduce the risk of cancer of the mouth. Around 80.2% with post- graduate degree, 78.7% with university qualification followed by 69%, 55.5% of secondary and primary education respectively believed that lifestyle modification could reduce the risk of cancer (Table 2).
Discussion
Oral cavity is one of the most common sites for various malignancies and is often associated with tobacco consumption either as smoking or chewing, alcohol consumption, ill-fitting dentures, infections, age, the presence of premalignant lesions etc. [7]. Globally the incidence rate of oral cancer is high despite the advances in therapeutic techniques, screening methods which can be attributed to the lack of knowledge and awareness about the disease.
In our study, 775 patients visiting King Khalid University-College of Dentistry were given a set of questionnaire to assess their level of knowledge and awareness of oral cancer. The majority (92.9%) of participants lived in the urban area with the average age of 31.81±10.33 years and most of them (53.5%) had postgraduate qualification.
Our study similar to the study conducted among randomly selected dental practitioners of UAE [8] showed that tobacco (67.5%) and alcohol (36.5%) is the most important cause of oral cancer. Tobacco use, heavy alcohol consumption, and poor diet altogether are responsible for the majority of oral cancer. Tobacco contents such as tar, nicotine, and nitrosamine vary each method of tobacco consumption thus increasing the risk of head and neck cancer [9].
Our study showed a general lack of knowledge about cancer and only 47% heard of oral cancers from several sources. This is similar to study conducted in Iran where only 54% were aware of probability or oral cancer [10]. This awareness factor also depends on education, an important sociodemographic factor. Therefore it was identified during the study that participants with higher education had more awareness about oral cancer and its screening methods. 67.2% of postgraduates, 74.7%with university education and around 55% with secondary and primary education each agree that tobacco is the main cause of cancer. 52.8% subjects with postgraduates, 44% with university qualification respectively disagreed that oral cancer is contagious. Around 80.2% with post- graduate degree, 78.7% with university qualification followed by 69%, 55.5% of secondary and primary education respectively believed that lifestyle modification could reduce the risk of cancer.
Around 55% of the population with tobacco chewing habit disagreed with the statement that oral cancer is a matter of luck and there is nothing we can do to avoid it. Smokeless tobacco is one of the major risk factors for oral cancer contributing over 90% of the global smokeless tobacco use burden is in South Asia [11]. According to sources of knowledge about oral cancer, most of the participants got the information from mass media (81.9%), family (31.5 %). The dental practitioners provided information to only 8.9% of the population. This is less when compared to the study conducted in conducted in Nigeria, South India, and Iran where dental practitioners were very important sources of information about cancer to the patients [10, 12, 13].
It was also observed that only 0.6% of our study participants received oral cancer examination within the last year which is similar to study conducted in Turkey where 60.7% of participants had never heard of oral cancer and 0.9% reported having had an oral cancer examination within the last year [14].
In our study that 45.7% believed oral cancer to be a boil, infection or abscess, 42.2% believed it to be an ulcer that does not heal and 41.9% thought it was tissue overgrowth or lump which are slightly different from studies conducted earlier where white patch (33.8%), bleeding, painless red patches (25.48%) were considered as the most signs of the oral cancer [15, 16].
Oral hygiene frequency of more than 1 time daily was observed in only 52% of the study participants. Further, during the study, it was observed that 89.5% were aware that detection of oral cancer in early stages could increase the success of the treatment and 77.7% were aware that lifestyle modification could reduce the risk of cancer of the mouth. 94.3% of subjects who consumed more than 5 units of fruits or vegetables per day had received an oral cancer examination within the last year. Good oral hygiene habits characterized by healthy gums, brushing more than once daily, annual dental check-ups, and proper safe dental practices have been associated with reduced risk of oral cancer significantly as observed in a case-control study in India by Gupta B, et al. [17].
Further, during the study, it was observed that 89.5% were aware that detection of oral cancer in early stages could increase the success of the treatment and 77.7% were aware that lifestyle modification could reduce the risk of cancer of the mouth. Around 80.2% with post- graduate degree, 78.7% with university qualification followed by 69%, 55.5% of secondary and primary education respectively believed that lifestyle modification could reduce the risk of cancer. Only 11% agreed that having oral cancer is a matter of luck and there is nothing we can do to avoid it, this observation in our study is better than a study conducted in Portugal where 28.1% believed that whether a person developed oral cancer or not is a matter of luck and therefore is unavoidable [18]. But at the same time similar to findings in the study conducted in a community of Suzhou, China where 11% believed that whether a person developed oral cancer or not is a matter of luck and therefore is unavoidable and 17% subjects do not know [19].
Though our study collects the substantial amount of data on the sociodemographic factors, knowledge, and awareness of oral cancer, the limitation of our study are small sample size, the restricted number of questionnaires on knowledge and awareness among patients, the absence of involvement of dental practitioners or questionnaires about them.
Several studies have been conducted across the globe to assess the knowledge and awareness about oral cancer but still level of public awareness and knowledge about the disease are insufficient. Oral cancer therapy requires multidisciplinary approaches such as chemotherapy, surgery, radiation therapy, etc and the role of dental practitioner becomes very important in the early diagnosis of the disease.
Conclusion
Our study highlights the general lack of awareness and knowledge on oral cancer among dental patients visiting King Khalid University-College of Dentistry in Saudi Arabia. A good oral health planning should be focused on providing basic education on oral cancer, oral cancer screening techniques by the active involvement of both the patients and the dentists.
References
-
Varshitha A (2015) Prevalence of oral cancer in India. Pharm Sci Res 7(10): 845-848.
-
Foundation OC Information-Support-Advocacy- Research and Hope.
-
Petersen PE (2005) Strengthening the prevention of oral cancer: the WHO perspective. Community Dent Oral Epidemiol 33(6): 397-399.
-
Ram H, Sarkar J, Kumar H, Konwar R, Bhatt MLB, et al. (2011) Oral Cancer: Risk Factors and Molecular Pathogenesis. J Oral Maxillofac Surg 10(2): 132-137.
-
Mehrotra R, Yadav S (2006) Oral squamous cell carcinoma: Etiology, pathogenesis and prognostic value of genomic alterations. Indian J Cancer 43(2): 60-66.
-
Gopal KS, Duraiselvi P (2014) Awareness and Knowledge of Oral Cancer among Dental Patients: A Survey Based Questionnaire Study. Int J Adv Health Sci 1(7): 12-15.
-
Jay Mahesh K, Surabhi G, Mitesh P, Jyothi PA, Chetan H (2015) Knowledge, Attitude and Awareness of Oral Carcinoma among Dental Practitioners-a Survey. IJOCR 3(4): 32-36.
-
Abdullah Jaber M (2011) Dental practitioner’s knowledge, opinions and methods of management of oral premalignancy and malignancy. Saudi Dent J 23(1): 29-36.
-
Johnson N (2001) Tobacco use and oral cancer: a global perspective. J Dent Educ 65(4): 328-339.
-
Razavi SM, Zolfaghari B, Foroohandeh M, Doost ME, Tahani B, et al. (2013) Dentists' knowledge, attitude, and practice regarding oral cancer in Iran. J Cancer Educ 28(2): 335-341.
-
Khan Z, Tönnies J, Müller S (2014) Smokeless Tobacco and Oral Cancer in South Asia: A Systematic Review with Meta-Analysis. J Cancer Epidemiol 2014: 394696.
-
Srikanth Reddy B, Doshi D, Padma Reddy M, Kulkarni S, Gaffar A, et al. (2012) Oral cancer awareness and knowledge among dental patients in South India. J Craniomaxillofac Surg 40(6): 521-524.
-
Lawoyin JO, Aderinokun GA, Kolude B, Adekoya SM, Ogundipe BF (2003) Oral cancer awareness and prevalence of risk behaviours among dental patients in South-western Nigeria. Afr J Med Med Sci 32(2): 203-207.
-
Peker I, Alkurt MT (2010) Public awareness level of oral cancer in a group of dental patients. J Contemp Dent Pract 11(2): 49-56.
-
West R, Alkhatib MN, McNeill A, Bedi R (2006) Awareness of mouth cancer in Great Britain. Br Dent J 200(3): 167-169.
-
Tomar SL, Logan HL (2005) Florida adults' oral cancer knowledge and examination experiences. J Public Health Dent 65(4): 221-230.
-
Gupta B, Bray F, Kumar N, Johnson NW (2017) Associations between oral hygiene habits, diet, tobacco and alcohol and risk of oral cancer: A case- control study from India. Cancer Epidemiol 51: 7-14.
-
Luís Silva M, Filomena S, Júlio P, Saman W (2012) Oral Cancer Awareness and Knowledge in the City of Valongo, Portugal. Int J Dent 2012: 8.
-
Vasireddy VK (2016) A Study on knowledge and awareness on oral cancer in a community of Suzhou, China. Value in Health 19(3): 92-93.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells