The Management of a Persistent Periapical Lesion in Endodontically Treated Teeth: About Two Case Reports
The present article describes a combination of endodontic therapy and surgical intervention related to two cases report with use of mineral trioxide aggregate (MTA) or IRM. It highlights a successful management of periapical defects.
Alojaym Tariq1*, Ben Ghenia Hedia2 and Jihed Ben Ammar3
Arabia
Kingdom of Saudi Arabia
of Saudi Arabia, Tel: +966506621671; Email: tariq2303@gmail.com Keywords: Periapical surgery; Periapical lesion; Retrograde treatment; MTA; IRM
Introduction
The specific goals of periapical surgery are to access the affected area, remove the diseased tissue, evaluate the root circumference and root canal system, and place a biocompatible seal in the form of a root-end filling that can stimulate regeneration of the periodontium. The evaluation of failure or success after periapical surgery is based on clinical and radiographic criteria [1].
There are many causes described in the endodontic literature for post treatment disease as poor access cavity design, untreated canals, canals that are poorly cleaned and obturated, complications of instrumentation (ledges, perforations, or separated instruments), overextensions of root-filling materials and coronal leakage [2, 3].
Nonsurgical retreatment is the first choice for attempting to correct obvious deficiencies in the previous treatment. But, when it is difficult, dangerous or impossible, periapical surgery is the last attempt to maintain the tooth [4, 5].
Currently, surgical technique employs the operative microscope which has considerably broadened the indications and therapeutic possibilities [6].
The surgical intervention aims to remove the infected root-end and seal any remaining bacteria in the root canal system from the periradicular tissues [7]. In addition to the elimination of pathological tissues, periapical surgery usually comprises root resection, preparation of root-end cavity and placement of a root-end filling material [8].
Suggested requirements for a retrograde root-filling material are, in addition to sufficient apical obturation, it should be nontoxic, non-resorbable, stable, and biocompatible [9]. IRM (DENTSPLY International Inc.) has been used as a retrograde rootend filling material before MTA, which was invented in the early 1990s, is reinforced zinc-oxide eugenol cement gives a high physical strength and a considerably easier manipulation. MTA was invented and developed at Loma Linda University, California by Torabinejad and co-workers is reported to show good sealing ability and a high degree of biocompatibility [10, 11].
Case 1
A 48 -year-old male with a non-contributory medical history was referred to conservative dentistry and endodontic department at dental clinic of dental medicine due to periodic swelling and discomfort associated with his upper right central incisor. The report from the referring dentist noted that the endodontic treatment was started on this tooth which is a bridge support; the access cavity was made through the crown and a K file was fractured in the canal. Intraoral examination revealed slight sensitivity to palpation of the tissues adjacent to the apex of the tooth. The periodontium was normal with attached gingiva width superior to 5mm. Initial radiographs showed radiolucency related to the apex of the tooth #11# (Figure 1). According to the clinical and radiographic findings, the final clinical diagnosis was Previously Initiated Therapy and Asymptomatic Apical Periodontitis.

The decision was to continue the endodontic therapy, in the first session the chemo-mechanical preparation was conducted after bypassing the fractured file and calcium hydroxide dressing was applied. A second appointment was fixed after 2 weeks.
The patient didn’t show up and lost to sight for 8 months. He returned when the tooth became symptomatic with painful palpation. A lateral perforation at the level of the fractured file was noticed and the apical path was not found and we failed to bypass again the file (Figure 2).

The perforation was sealed with MTA (Figure 3). After 48h the canal obturation was fulfilled (Figure 4).
Endodontic surgery was recommended to the patient. The risk and benefits of the proposed treatment were described, and informed consent was obtained.


After surgical procedure and initial curettage, granulation tissues were completely removed. After root- end resection (~3 mm), the root-end was prepared with an ultrasonic retrotip. MTA powder and liquid were mixed according to the manufacturer’s instructions; the cement was delivered into the root-end cavity and packed with microplugger. After radiographic control of the root- end filling (Figure 5). The patient returned three days later for suture removal with no postoperative pain. The patient presented for a recall appointment 6 months later (Figure 6). Clinical examination revealed no sensitivity to percussion or palpation, and the tooth was fully functional with normal probing depths. Radiographic examination showed the apical lesion had healed with a normal PDL established.


Case 2
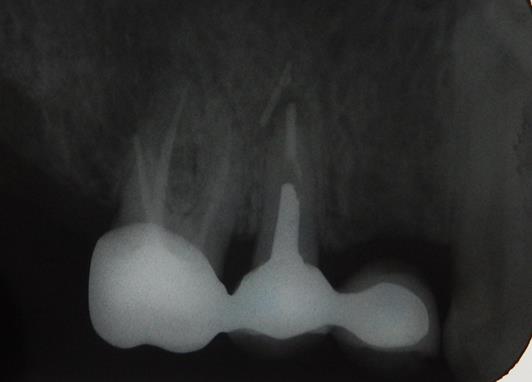
A 60 year old female patient with a non-contributory medical history was referred to the Department of Conservative Dentistry and Endodontics for sporadic swelling in the right maxillary region and tenderness to percussion of the maxillary second premolar. The intraoral radiograph revealed radiolucent periapical lesion related to the apices of the maxillary second premolar and involving extruded gutta percha (Figure 7). The CBCT scans revealed a casted post in each canal and a palatal canal none filled.
According to the clinical and radiographic findings, the final clinical diagnosis was previously treated tooth and chronic apical abscess. The decision was an apical resection with retrograde treatment.
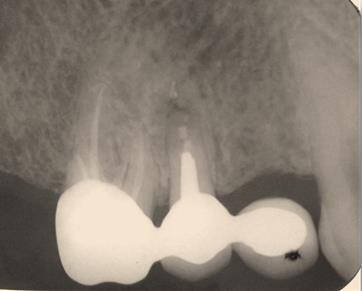
After performing an endodontic surgery, the granulation tissue was curetted and osteotomy was prepared. 3mm of root apex was resected for buccal and palatal roots. The root end preparation was carried out with ultrasonic in a P5 unit (Satalec; France) to contact with metallic posts under copious amounts of coolant of sterile saline. The root end was dried and IRM was placed and packed in to place with microplugger. After confirmation with postoperative radiograph (Figure 8). The patient returned three days later for suture removal with no postoperative pain; healing was uneventful. The patient was examined clinically and radiographically at a 3 month and 9 month recall visit. Periapical healing around roots was observed radiographically at the 9 month recall (Figure 9).

Discussion
The success rate achieved by traditional means of surgery varies from 40% to 90%. With the advanced endodontic surgical armamentarium, the success rate increased to 96.8% [12]. Zuolo, et al. reported that the postsurgical outcome is 97% for the anterior teeth and 85%for for the posterior teeth due to complex radicular anatomy [13]. Both retrograde root-filling materials, IRM and MTA can serve as a root-end seal in periapical surgery performed with an ultrasonic root-end preparation technique [14].
In the first case the separated file and the lateral perforation impede the shaping and cleaning procedures to full working length.
In the second case, the presence of two long casted posts (more than 5 mm) was an early indication for the surgery.
In many cases, a prosthetic crown or post has to be removed before the retreatment of the orthograde root filling can be performed and this procedure can involve the risk of causing a root fracture. In such cases periapical surgery is the best treatment alternative [15]. In a long- term perspective the orthograde retreatment of the root filling offers a more favorable outcome, 83% versus 72% for periapical surgery after 4-6 years [16].
Periodical radiographs provide limited information because the three-dimensional anatomy is represented in a two-dimensional image. In contrast, the CBCT eliminates the superimposition of the surrounding structures, detects un-diagnosed lesions and can differentiate between apical cysts and granuloma [17]. MTA was used in the first case; include biocompatibility, low cytotoxicity, antimicrobial properties, low microleakage, and the ability to set in the presence of blood or moisture. Drawbacks of MTA include a long setting time, difficulty in manipulation.
In the second case, IRM was employed as a retrograde biocompatible filling material, ad it is easy to handle make it a good sealing alternative.
IRM elicited little to no inflammatory effects after 90 days, which led to the conclusion that the oral tissue was just as tolerant of IRM as it was of any other retrograde filling material. From the biologic perspective of regeneration of the periradicular tissues. MTA appears to have a clear advantage over the other available materials including IRM without affecting significantly the outcome [16, 18, 19, 20, 21, 22]. In the present cases, Radiographic follow-up is important to determine the amount and speed of bone regeneration. After following the cases for 6 and 9 months we have observed that there was uneventful healing, which shows that the long term prognosis of the teeth is good.
Conclusion
Two case reports of surgical interventions are presented, each one utilizing a modern technique with retrograde filling MTA or IRM. IRM and MTA can serve as a root-end seal in periapical surgery performed with an ultrasonic root-end preparation technique. The clinical and radiographic follow-up confirmed the success.
References
-
Vivek Chat, Shefali Ch (2012) Regenerative Therapy as an Adjunct to Periapical Surgery: A Case Report. Int J Clin Pediatr Dent 5(1): 75-77.
-
Chugal NM, Clive JM, Spangberg LS (2003) Endodontic infection: some biologic and treatment factors associated with outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96(1): 81-90.
-
Stropko JJ, Doyon GE, Gutmann JL (2005) Root-end management: resection, cavity preparation, and material placement. Endod Topics 11(1): 131-151.
-
Roda R, Getteman B (2016) Non-surgical retreatment. In: Kenneth M & Hargreaves Louis H Berman (Eds.), Cohen’s pathways of the pulp, 11th (Edn.), Missouri: Elsevier, pp: 324.
-
Parirokh M, Torabinejad M (2010) Mineral trioxide aggregate: a comprehensive literature review – Part III: Clinical applications, drawbacks, and mechanism of action. J Endod 36(3): 400-413.
-
Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG (2007) Endodontic applications of cone-beam volumetric tomography. J Endod 33: 1121.
-
Christiansen R, Kirkevang LL, Horsted-Bindslev P, Wenzel A (2009) Randomized clinical trial of root- end resection followed by root-end filling with mineral trioxide aggregate or smoothing of the orthograde gutta-percha root filling-1 year follow-up. Int Endod J 42(2): 105-114.
-
Gutman JL, Harrison JW (1991) Surgical endodontics. Botson: Blackwell Scientific.
-
Chong BS, Pitt Ford TR (2005) Root-end filling materials: rationale and tissue response. Endod Topics 11(1): 114-130.
-
Torabinejad M, Hong CU, Lee SJ, Monsef M, Pitt Ford TR (1995) Investigation of mineral trioxide aggregate for root end filling in dogs. J Endod 21(12): 603-608.
-
Saidon J, He J, Zhu Q, Safavi K, Spångberg LS (2003) Cell and tissue reactions to mineral trioxide aggregate and Portland cement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 95(4): 483-489.
-
Kim S, Kratchman S (2006) Modern endodontic surgery concepts and practice: a review. J Endod 32(7): 601-623.
-
Zuolo ML, Ferreira MO, Gutmann JL (2000) Prognosis in periradicular surgery: a clinical prospective study. Int Endod J 33(2): 91-98.
-
Tang Y, Li X, Yin S (2010) Outcomes of MTA as root- end filling in endodontic surgery: a systematic review. Quintessence Int 41(7): 557-566.
-
Walivaara DA, Abrahamsson P, Fogelin M (2016) Periapical Surgery with IRM and MTA as Retrograde Root-end Fillings‒A Prospective Randomized Clinical Study of 186 Consecutive Teeth. Dentistry 6: 393.
-
Torabinejad M, Corr R, Handysides R, Shabahang S (2009) Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod 35(7): 930-937.
-
Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR (2008) Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod 34(3): 273- 279.
-
Walivaara DA, Abrahamsson P, Isaksson S, Salata LA, Sennerby L, et al. (2012) Periapical tissue response after use of intermediate restorative material, gutta- percha, reinforced zinc oxide cement, and mineral trioxide aggregate as retrograde root-end filling materials: a histologic study in dogs. J Oral Maxillofac Surg 70(9): 2041-2047.
-
Torabinejad M, Pitt Ford TR, McKendry DJ, Abedi HR, Miller DA, et al. (1997) Histologic assessment of Mineral Trioxide Aggregate as a root-end filling in monkeys. J Endod 23(4): 225-228.
-
Baek SH, Plenk H Jr, Kim S (2005) Periapical tissue responses and cementum regeneration with amalgam, Super EBA, and MTA as root-end filling materials. J Endod 31(6): 444-449.
-
Johnson B, Fayad M (2016) Periradicular surgery. In: Kenneth M. Hargreaves Louis H. Berman, editors. Cohen’s pathways of the pulp, 11th (Edn.), Missouri: Elsevier, pp: 387.
-
Harrison JW, Johnson SA (1997) Excisional wound healing following the use of IRM as a root-end filling material. J Endod 23(1): 19-27.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells