Tooth Preparation with a 9.3 µm CO2 Laser Reduces Demineralization around Dental Restorations
Objective: To determine if cavity preparation using a 9.3 µm CO2 -laser can prevent demineralization around a traditional composite, bioactive composite, flowable composite, or glass ionomer restoration compared to preparation with a traditional carbide-bur. Methods: Forty human posterior teeth were randomized. Vickers surface hardness measurements (MicroMet® 2104 Buehler) of enamel were taken. Twenty samples were irradiated with the 9.3μm CO2 -laser and twenty were identically prepared using a carbide-bur. Each group (n=5) was restored with Filtek™ One Bulk Fill Restorative (3M) (Filtek OB), ACTIVA™ BioACTIVERESTORATIVE™ (Pulpdent) (ACTIVA), GC Fuji IX GP® FAST (GC) (Fuji), or Filtek™ Bulk Fill Flowable Restorative (3M) (Filtek F) per manufacturer instructions. Samples were placed in 0.05M acetate buffer demineralizing solution for 7 days, thermomechanically cycled for 10,000 cycles between 4-5°C and 55-60°C with a dwell time of 15s, immersed in 2% methylene blue solution and cut longitudinally. Three Vickers surface hardness measurements of enamel and dentin were taken near the subsurface restorative margin. Microleakage was assessed by measuring dye penetration along the gingival floor. Samples restored with the same material were compared using the two-sample t-test. Significance level was set at 0.0042 using the Bonferroni correction for multiple comparisons. Results: Laser-irradiated and bur prepared groups had similar baseline surface microhardness for all materials. Sub-surface enamel microhardness of laser-irradiated samples in ACTIVA and Filtek F groups, and dentin microhardness of laser-irradiated samples in Filtek OB, ACTIVA, Fuji, and Filtek F groups were statistically significantly greater than bur-prepared samples. There was no difference in microleakage between laser-irradiated and bur-drilled samples. Conclusion: Using a 9.3 µm CO2-laser in tooth preparation can prevent demineralization around Filtek OB, ACTIVA, Fuji and Filtek F restorations compared to traditional carbide-bur preparation.
Introduction
Lasers have been suggested for use in the dental field since the mid-1960’s for a wide array of procedures. Some of the first proposed functions in the field of dentistry include the 9.3um CO2 lasers’ ability to prevent demineralization by altering surface enamel [1, 2, 3, 4, 5]. As the use of lasers in dentistry expanded other lasers such as the Er:YAG [6, 7, 8] and the Nd:Yag [9, 10, 11] were suggested for their ability to cause similar changes in tooth structure ultimately resulting in a resistance to acid and demineralization. As such laser treatments have become more and more promising in the field of preventative dentistry, studies have explored the use of other lasers such as the Er, Cr: YSGG laser [12] and the argon laser [13, 14] as well as combination treatments of different laser types and the addition of fluoride [9, 15, 16, 17].
Studies have shown that the melting and hardening of the smear layer prevent acid demineralization in both enamel and dentin hard tissues [5]. Treatment of tooth structure with CO2 laser irradiation has shown to melt the enamel structure and fuse it making it significantly more resistant to demineralization and decreasing its solubility [18, 19, 20]. The effect has been well studied and the mechanism of action is best demonstrated by using the CO2 laser to irradiate caries, as there is a significantly increased ratio and content of Ca and P in the surrounding treated hard tissue [18]. In dentin, similar structural alterations have been shown to prevent demineralization [18, 19, 21, 22]. Additionally, dentin tubules exposed by the cutting abilities of the laser become sealed and both the surface and subsurface dentin are protected from the full detriment that a demineralizing environment would have on the tooth structure [22].
Since the initial work with CO2 lasers, studies have explored the ability of these lasers to prevent such demineralization at varying wavelengths, ultimately concluding that 9.3 and 9.6 μm lasers are most successful in inhibiting demineralization without the subsurface temperature rises [2, 23]. Konishi, et al. showed, in a pilot study, that teeth prepared using a 9.3 μm CO2 laser were more resistant to secondary caries than teeth drilled with a high speed handpiece [3]. However, this study used resin composite to restore the teeth prior to a demineralization assay and noted that they did not use any etchant or adhesive, and that use of either or both may have changed the outcome [3]. Since this finding, others have re-enforced the ability of a 9.3μm CO2 laser to prevent enamel demineralization and analyzed its protective features in connection with fluoride use, however such studies observed the laser’s ability to prevent demineralization on surface enamel rather than prepared and restored teeth [24, 25]. Rechmann, et al. showed that such findings are applicable to vital teeth in his in vivo study of teeth with bonded orthodontic brackets that received 9.6μm laser irradiation prior to bonding, finding that these teeth were more resistant to demineralization than those that had not received such treatment [26].
The aim of the present study is to investigate at the ability of a 9.3μm CO2 laser to prevent demineralization of enamel and dentin at the sub-surface margins of a preparation that has been restored in a clinically applicable fashion using appropriate etch, adhesive and conditioner.
Material and Methods
Forty de-identified extracted human posterior teeth collected and stored for less than six months with no prior restorations and no gross decay were disinfected in a 1:10 bleach dilution. Teeth were randomized and divided into 8 groups according to their future preparation and restorative technique. The mesial surface of each tooth was identified and initial measurements of Vickers surface hardness were taken at 4 standardized points in the enamel, two buccal and two lingual, around the intended margins of the future preparation and restoration using a microhardness tester (MicroMet® 2104 Buehler, IL, USA) [27]. Each point was 2mm away from one another. All samples were prepared with a 1.5-2mm deep and 4mmx4mm box on the mesial side, with the gingival floor 1mm below the cementoenamel- junction (CEJ) in correspondence with the location of the original microhardness measurements. Half the samples, or four groups (n=5) were prepared using the Solea 9.3μm CO2 laser (Solea® Dental Laser, Convergent Dental, Needham, MA, USA) and half the samples were prepared with a carbide bur in correspondence with their assigned group. Samples were stored in distilled water after preparation. One laser-prepared group (n=5) and one bur-prepared group (n=5) was restored with Filtek™ One Bulk Fill Restorative (3M, St Paul MN, USA) (Filtek OB), ACTIVA™ BioACTIVE- RESTORATIVE™ (Pulpdent, Watertown MA, USA) (ACTIVA), GC Fuji IX GP® FAST (GC, Alsip IL, USA) (Fuji), or Filtek™ Bulk Fill Flowable Restorative (3M, St Paul MN, USA) (Filtek F) per manufacturer instructions. Samples were placed in 0.05M acetate buffer demineralizing solution for seven days to create artificial caries [3, 19, 28]. To assess microleakage, samples were then thermo-mechanically cycled for 10,000 cycles between 4-5°C and 55-60°C with a dwell time of 15s to simulate a service year [29]. All samples were then immersed in 2% methylene blue solution and cut longitudinally (IsoMet® 1000, Buehler) and gingival margin microleakage was measured using OmniMet analysis (OmniMet Buehler, IL, USA). Vickers surface hardness measurements of the longitudinally cut samples was then taken again in both the dentin and subsurface enamel. Three samples 10μm apart of enamel and dentin were taken 50μm away from the restoration margin. Laser and bur samples of surface enamel restored with the same material were compared using the two-sample t-test. Significance level was set at 0.0042 using the Bonferroni correction for multiple comparisons.
Results
Laser and bur group samples (n=5) from Filtek OB, ACTIVIA, Fuji, and Filtek F restorative groups had similar baseline enamel microhardness (P 0.17, 0.36, 0.23, 0.82 respectively). Microleakage was not statistically significantly different between laser and bur groups (Table 1). The sub- surface enamel microhardness of lased samples in ACTIVA and Filtek F groups was statistically significantly greater than bur prepared samples (P .004 and <.001 respectively) (Table 2, Figure 1). The dentin microhardness of the lased samples in Filtek OB, ACTIVA, Fuji, and Filtek F groups was statistically significantly greater than bur prepared samples (P <0.001, <0.001, 0.002, 0.004 respectively) (Table 2, Figure 2).
| Group | Laser Microleakage | Bur Microleakage | P value |
|---|---|---|---|
| Filtek OB | 58.3 ± 43.5 | 58.3 ± 43.0 | 1 |
| ACTIVA | 55.7 ± 35.7 | 68.0 ± 36.2 | 0.63 |
| Fuji | 97.9 ± 4.7 | 76.3 ± 35.6 | 0.22 |
| Filtek F | 48.8 ± 11.4 | 62.9 ± 42.8 | 0.49 |
Table 1: Post-Demineralization Values of Microleakage.
Laser and bur samples of surface enamel to be restored with the same material were compared using the two-sample t-test with equal variances. P values <0.0042 were considered significant. Table 1: Post-Demineralization Values of Microleakage.
| GROUP | Post-Demineralization | Post-Demineralization | ||||
|---|---|---|---|---|---|---|
| Enamel Microhardness | Dentin Microhardness | |||||
| Laser | Bur | P value | Laser | Bur | P value | |
| Filtek OB | 246.4 ± 38.8 | 205.1 ± 26.9 | 0.09 | 48.6 ± 4.7 | 31.3 ± 2.4 | <0.001 |
| ACTIVA | 242.7 ± 17.7 | 184.4 ± 12.5 | < 0.001 | 54.7 ± 6.4 | 36.3 ± 1.5 | <0.001 |
| Fuji | 230.1 ± 40.0 | 192.9 ± 12.3 | 0.08 | 41.4 ±3.5 | 26.8 ± 6.2 | 0.002 |
| Filtek F | 276.5 ± 48.2 | 185.1 ± 16.8 | 0.004 | 51.0 ± 6.2 | 37.3 ± 4.5 | 0.004 |
Table 2: ** Enamel and Dentin Microhardness.
Post-demineralization mean and standard deviation of enamel and dentin samples within the same group (n=5) were calculated. Significance level was set at 0.0042 using the Bonferroni correction for multiple comparisons. P values <0.0042 were considered significant. Table 2: Enamel and Dentin Microhardness.
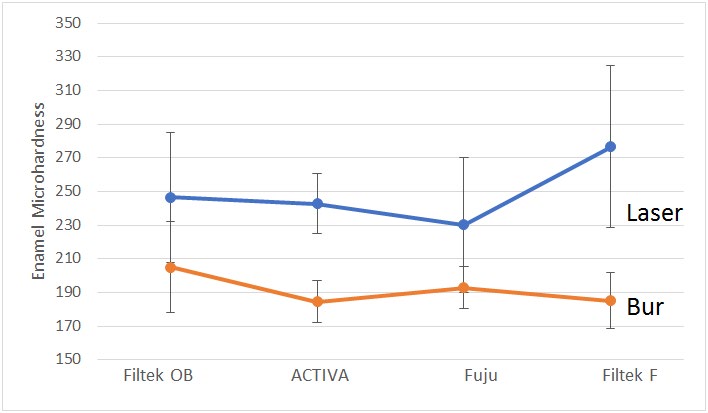
*Bars on graph denote standard deviations. Figure 1: Post-Demineralization Microhardness of Cut Enamel.
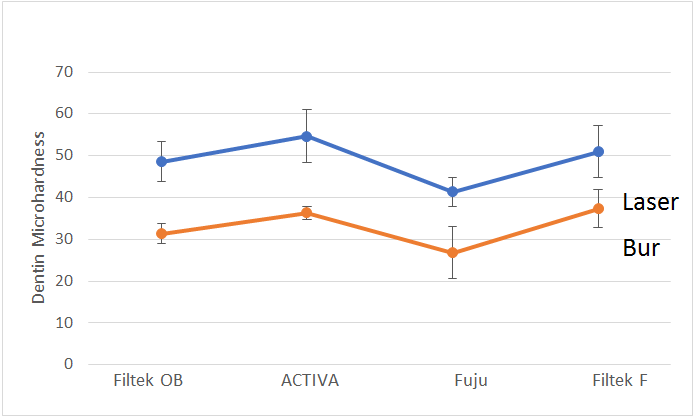
*Bars on graph denote standard deviations. Figure 2: Post-Demineralization Microhardness of Cut Dentin.
Discussion
The benefits of using a 9.3um CO2 laser for tooth preparation include it’s technically accuracy, ease of use and diversity in preparing both soft and hard tissue. This study provides evidence for an added benefit, the decrease in demineralization around the margin of a restoration when using a 9.3 μm CO2 laser to remove caries and prepare teeth. While previous studies have shown the ability of a 9.3 μm CO2 laser to change tooth structure resulting in a decrease susceptibility to acid erosion [2, 3, 24, 30] the current study was designed in a clinically-relevant manner by using the laser to create preparations and restoring them with a variety of popular clinical restorative material per their manufacturers recommendations for etch, conditioner and adhesive. In doing so, the results demonstrate the ability of the 9.3 μm CO2 laser to inhibit demineralization adjacent to many common clinical restorations and provide support for the expanded use of the laser in clinical preparations.
Because samples were to be prepared in a clinically relevant manner of tooth preparation and subsequent restoration, the initial microhardness measurements were done on uneven, unpolished surfaces introducing the possibility for error in the measurements taken on the Vicker’s microhardness machine which functions most ideally on ground, polished and acrylic-embedded samples. The standard deviations in initial microhardness for each group showed a much greater variance when compared to microhardness readings taken on the sectioned, flat, polished post-demineralization sub-surface samples. These higher standard deviations are likely due to the uneven tooth surfaces and while the testing machine can appropriately measure surface hardness as recorded in this method, when measuring such uneven surfaces it is likely necessary to spread out measurements across the surface and take a greater number of readings to reduce variance between measurements as compared to measurements taken on a flat and polished surface.
The post-demineralization enamel and dentin microhardness readings showed that there was a statistically significantly higher microhardness in laser prepared ACTIVA and Filtek F enamel groups and all four laser prepared dentin treatment groups as compared to bur prepared samples restored with the same material, indicative of an increased resistance to acid and therefore demineralization (Table 2). These results verify that, as predicted, the laser is able to produce an acid resistant layer that even when restored and exposed to an acid challenge, prevents acid erosion and ultimately demineralization and loss of tooth structure hardness. While many previous studies have shown the laser’s ability to produce acid resistance [2, 24] the current study verifies that if the laser is used in cavity preparation and clinical restoration a similarly effective acid resistant layer is both formed and functions to reduce demineralization. While in dentin, an innately softer and more acid-susceptible tissue, a decrease of hardness was prevented in all four laser prepared groups, in enamel only two of the four experimental groups showed such acid resistance. It is possible that in order to replicate sufficient acid erosion in order to see a statistically significant difference in microhardness a longer, more acidic or combination remineralization/ demineralization assay such as that used in Rechmann et al. would be necessary [2, 24].
Results showed that there was no difference in the percentage of microleakage measured between samples prepared with a CO2 laser compared to those prepared with a carbide bur. Microleakage occurs when bacteria and bacterial byproducts are able to leak at the tooth-restoration interface ultimately leading to dentin sensitivity and the need to replace restorations. Previous studies such as Shafiei, et al. Mozaffari, et al. and Santos, et al. have shown that restorations pre-treated with a CO2 laser have not had a reduced susceptibility to microleakage as may have been predicted [31, 32, 33]. While the laser is able to change the enamel and dentin structure to prevent sub-surface marginal demineralization, such changes do not improve the tooth-restoration interface in a way that prevents microleakage better than the control. Ultimately, the CO2 laser has no adverse effect on the sealing of enamel at the sub-surface margins of preparations restored in any of the four restorative groups. It can however be hypothesized that while microleakage may still occur in these laser prepared restorations, dentin irritation and enamel degradation typical of microleakage may be prevented by increased hardness of the sub-surface tooth structure indicated by the results of the subsurface microhardness assays and needs to be explored in future studies in vital teeth.
Additional studies should explore the ability of the laser to provide such changes in dentin and sub-surface enamel on a larger scale and with additional restorative products. Further studies may also find a better way to control for the differences in initial hardness and mineralization both between samples and within the same sample. Such error between samples could possibly be minimized by creating bur and laser preparations on the same tooth and comparing results within one sample. Instead of using surface enamel as a non-demineralized control, measuring subsurface enamel on the cut enamel samples in a deeper area that was not affected by the acid demineralization, could provide a more accurate control. Alternatively, masking an area of each tooth from the demineralization solution and taking a measurement at the same depth as the prepared, demineralized and sectioned data, could provide more comparable controls. Finally, while Rechmann, et al. looked at the abilities of a similar 9.6 um CO2 laser to prevent demineralization intraorally, the study look at surface laser treatment adjacent to orthodontic bracket placement as opposed to an intraoral cavity preparation and restoration [26]. Ultimately, studies should be conducted in- vivo using the 9.3 um CO2 laser for cavity preparation with complete clinical restoration as such results have not been shown and would provide high levels of evidence of the benefits of laser cavity preparation.
Conclusion
This study demonstrated that sub-surface enamel and dentin immediately adjacent to the internal margins of a preparation and restoration are more resistant to demineralization when prepared using a 9.3um CO2 laser than when prepared with a traditional carbide bur. While the study was in vitro and had some limitations, the tooth’s increased resistance to demineralization could indicate an intraoral reduction in recurrent carries around the margins of restorations and ultimately provide further longevity to restorations prepared with the 9.3um CO2 laser than those prepared with a traditional carbide bur.
References
-
Stern RH, Vahl J, Sognnaes RF (1972) Lased enamel: ultrastructural observations of pulsed carbon dioxide laser effects. J Dent Res 51(2): 455-460.
-
Featherstone JD, Barrett Vespone NA, Fried D, Kantorowitz Z, Seka W (1998) CO2 laser inhibitor of artificial caries-like lesion progression in dental enamel. J Dent Res 77(6): 1397-1403.
-
Konishi N, Fried D, Staninec M, Featherstone JD (1999) Artificial caries removal and inhibition of artificial secondary caries by pulsed CO2 laser irradiation. Am J Dent 12(5): 213-216.
-
Lombardo G, Pagano S, Cianetti S, Capobianco B, Orso M, et al. (2019) Sub-ablative laser irradiation to prevent acid demineralisation of dental enamel. A systematic review of literature reporting in vitro studies. Eur J Paediatr Dent 20(4): 295-301.
-
Hossain M, Nakamura Y, Kimura Y, Ito M, Yamada Y, et al. (1999) Acquired acid resistance of dental hard tissues by CO2 laser irradiation. J Clin Laser Med Surg 17(5): 223-226.
-
Apel C, Schafer C, Gutknecht N (2003) Demineralization of Er:YAG and Er, Cr:YSGG laser-prepared enamel cavities in vitro. Caries Res 37(1): 34-37.
-
Fornaini C, Brulat N, Milia G, Rockl A, Rocca JP (2014) The use of sub-ablative Er:YAG laser irradiation in prevention of dental caries during orthodontic treatment. Laser Ther 23(3): 173-181.
-
Colucci V, de Souza Gabriel AE, Scatolin RS, Serra MC, Corona SA (2015) Effect of Er:YAG laser on enamel demineralization around restorations. Lasers Med Sci 30(4): 1175-1181.
-
Kwon YH, Kwon OW, Kim HI, Kim KH (2003) Nd:YAG laser ablation and acid resistance of enamel. Dent Mater J 22(3): 404-411.
-
Pereira DL, Freitas AZ, Bachmann L, Benetti C, Zezell DM, et al. (2018) Variation on Molecular Structure, Crystallinity, and Optical Properties of Dentin Due to Nd:YAG Laser and Fluoride Aimed at Tooth Erosion Prevention. Int J Mol Sci 19(2): 433.
-
Braga SR, de Oliveira E, Sobral MA (2017) Effect of neodymium: yttrium-aluminum-garnet laser and fluoride on the acid demineralization of enamel. J Investig Clin Dent 8(1).
-
de Freitas PM, Rapozo Hilo M, Eduardo Cde P, Featherstone JD (2010) In vitro evaluation of erbium, chromium:yttrium-scandium-gallium-garnet laser- treated enamel demineralization. Lasers Med Sci 25(2): 165-170.
-
Anderson AM, Kao E, Gladwin M, Benli O, Ngan P (2002) The effects of argon laser irradiation on enamel decalcification: An in vivo study. Am J Orthod Dentofacial Orthop 122(3): 251-259.
-
Noel L, Rebellato J, Sheats RD (2003) The effect of argon laser irradiation on demineralization resistance of human enamel adjacent to orthodontic brackets: an in vitro study. Angle Orthod 73(3): 249-258.
-
Steiner Oliveira C, Rodrigues LK, Lima EB, Nobre dos Santos M (2008) Effect of the CO2 laser combined with fluoridated products on the inhibition of enamel demineralization. J Contemp Dent Pract 9(2): 113-121.
-
Moslemi M, Fekrazad R, Tadayon N, Ghorbani M, Torabzadeh H, et al. (2009) Effects of ER, Cr:YSGG laser irradiation and fluoride treatment on acid resistance of the enamel. Pediatr Dent 31(5): 409-413.
-
Al Maliky MA, Frentzen M, Meister J (2020) Laser- assisted prevention of enamel caries: a 10-year review of the literature. Lasers Med Sci 35(1): 13-30.
-
Takahashi K, Kimura Y, Matsumoto K (1998) Morphological and atomic analytical changes after CO2 laser irradiation emitted at 9.3 microns on human dental hard tissues. J Clin Laser Med Surg 16(3): 167-173.
-
Chang NN, Jew JM, Simon JC, Chen KH, Lee RC, et al. (2017) Influence of multi-wavelength laser irradiation of enamel and dentin surfaces at 0.355, 2.94, and 9.4 μm on surface morphology, permeability, and acid resistance. Lasers Surg Med 49(10): 913-927.
-
Vieira KA, Steiner Oliveira C, Soares LE, Rodrigues LK, Nobre dos Santos M (2015) In vitro evaluation of enamel demineralization after several overlapping CO2 laser applications. Lasers Med Sci 30(2): 901-907.
-
Kimura Y, Takahashi Sakai K, Wilder Smith P, Krasieva TB, Liaw LH, et al. (2000) Morphological study of the effects of CO2 laser emitted at 9.3 microm on human dentin. J Clin Laser Med Surg 18(4): 197-202.
-
Nammour S, Renneboog Squilbin C, Nyssen Behets C (1992) Increased resistance to artificial caries-like lesions in dentin treated with CO2 laser. Caries Res 26(3): 170-175.
-
Staninec M, Darling CL, Goodis HE, Pierre D, Cox DP, et al. (2009) Pulpal effects of enamel ablation with a microsecond pulsed lambda = 9.3-microm CO2 laser. Lasers Surg Med 41(4): 256-263.
-
Rechmann P, Rechmann BM, Groves WH, Le CQ, Rapozo Hilo ML, et al. (2016) Caries inhibition with a CO2 9.3 μm laser: An in vitro study. Lasers Surg Med 48(5): 546-554.
-
Lee R, Chan KH, Jew J, Simon JC, Fried D (2017) Synergistic effect of fluoride and laser irradiation for the inhibition of the demineralization of dental enamel. Proc SPIE Int Soc Opt Eng.
-
Rechmann P, Fried D, Le CQ, Nelson G, Hilo MR, et al. (2011) Caries inhibition in vital teeth using 9.6-μm CO2- laser irradiation. J Biomed Opt 16(7): 071405.
-
Ghanbarzadeh M, Ahrari F, Akbari M, Hamzei H (2015) Microhardness of demineralized enamel following home bleaching and laser-assisted in office bleaching. J Clin Exp Dent 7(3): 405-409.
-
Belcheva A, El Feghali R, Nihtianova T, Parker S (2018) Effect of the carbon dioxide 10,600-nm laser and topical fluoride gel application on enamel microstructure and microhardness after acid challenge: an in vitro study. Lasers Med Sci 33(5): 1009-1017.
-
Gale MS, Darvell BW (1999) Thermal cycling procedures for laboratory testing of dental restorations. J Dent 27(2): 89-99.
-
Rechmann P, Le CQ, Kinsel R, Kerbage C, Rechmann BMT (2020) In vitro CO2 9.3-μm short-pulsed laser caries prevention-effects of a newly developed laser irradiation pattern. Lasers Med Sci 35(4): 949-989.
-
Shafiei F, Memarpour M (2013) Effect of surface pretreatment with two desensitizer techniques on the microleakage of resin composite restorations. Lasers Med Sci 28(1): 247-251.
-
Mozaffari HR, Ehteshami A, Zallaghi F, Chiniforush N, Moradi Z (2016) Microleakage in Class V Composite Restorations after Desensitizing Surface Treatment with Er:YAG and CO2 Lasers. Laser Ther 25(4): 259-266.
-
Santos LC, Sfalcin RA, Garcia EJ, Zanin FAA, Brugnera A, et al. (2019) Microleakage of “Bulk-Fill” Composite Resin for Class II Restorations Pretreated With CO2 Laser in Deciduous Molars: An In Vitro Study. J Lasers Med Sci 10(4): 304-309.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells