Efficacy of Ozonated Water Adjunct to Regular Oral Hygiene Maintenance in Moderate Gingivitis: A Randomized Clinical Trial
Background: The antimicrobial effects and safety of ozone for intraoral use are well known, yet there is limited data from controlled clinical trials regarding the effect of ozonated water in the treatment of gingivitis. We aimed to evaluate the effectiveness of a new electrical oral health system powered by ozonated water against moderate gingivitis. Methods: In this randomized single blinded clinical study 55 volunteers with moderate gingivitis were randomly divided into three groups: group 1 treatment with ozonated water plus regular oral hygiene maintenance (test); group 2 treatment with mouth wash plus regular oral hygiene maintenance (control I); group 3 regular oral hygiene maintenance- twice daily brushing (control II). The gingival index and gingival bleeding index were evaluated at baseline (T0), after 2 weeks of treatment (T1) and after 4 weeks of treatment (T2). Results: Fifty volunteers were included in the analysis. The test group presented significant continuous improvement after ozone treatment, in all outcome measures. There was a statistically significant difference between test group and control II in the gingival index at the end of the four-week trial. There were no significant differences between test group and control I. Conclusion: Ozonated water adjunct to basic oral hygiene maintenance should be considered as an alternative management strategy to treat gingivitis. Specialized periodontal mouth wash was not found to be superior to Ozonated water.
Introduction
Periodontal diseases are one of the most prevalent inflammatory pathologies in adults [1, 2, 3]. The two modes of periodontal disease are Gingivitis and Periodontitis. Gingivitis [4] is reversible and non-destructive, with signs of inflammation: Untreated gingivitis can progress into the second, more severe form of periodontal disease- periodontitis [3]. Periodontal diseases are caused by the build-up of bacteria in the form of dental plaque. Each form of periodontal disease is further subdivided. The most prevalent form of gingivitis is plaque-induced gingivitis [5], with a worldwide prevalence in adults of 75% [6].
Although plaque induced gingivitis does not directly cause tooth loss, the condition can progress to periodontitis [7] if left untreated. Therefore, preventing and treating gingivitis is the main strategy for preventing the development of the destructive form of the disease- periodontitis [8]. The rough surface of mineralized plaque, calculus further promotes the growth of the plaque towards the tooth roots. As the inflammation progresses, a pocket is formed between the gums and the root of the tooth. This pocket hosts and promotes bacterial colonization and without adequate treatment the periodontium will be destroyed and the tooth will become mobile and ultimately potentially lost [9].
There are other local and systemic predisposing factors to periodontal diseases. Local risk factors include: tooth position, presence of prosthetic crowns and bridges with sub gingival finishing lines, overhanging restorations etc. Systemic risk factors for periodontal diseases include: Diabetes mellitus, Cardio vascular diseases, poor saliva flow. Smoking has a profound effect on the gingival tissue [10]. As mentioned above, the primary etiology of periodontitis is dental plaque [11], which constitutes food residues and colonizing bacteria. The fact that periodontitis is rarely painful promotes neglect and enables the inflammation to progress. Good oral hygiene is the key prevention method to control the bacterial load. Plaque control can be achieved by two complimentary methods: mechanical and chemical [12, 13].
Mechanical plaque control includes: removing dental plaque with a tooth brush (manual or electric), oral irrigators, interdental appliances and professional cleaning in a clinic setting. Chemical plaque control includes oral mouthwashes, toothpastes and gels with active anti-plaque agents [13]. For example, Chlorhexidine integrated in mouthwashes and gels is considered the gold standard chemical that combats plaque. There are several adverse effects of chlorhexidine when used more than two weeks continuously: teeth staining, increased calculus, mouth/throat irritation and dry mouth [14].
Ozone therapy for periodontal diseases was initially proposed fifty years ago [15]. Ozone (O3) is a natural gaseous molecule made up of three oxygen atoms. Ozone therapy is oxidative in which oxygen/ozone is administered for therapeutic purposes. There are 3 routes of Ozone administration: 1) gaseous; 2) aqueous; 3) in oil [16]. The Ozone molecule, known for its protective role in the earth’s atmosphere, has bactericidal, virucidal and fungicidal properties that may make it therapeutically beneficial [17].
Early in its history ozone was found to oxidize a spectrum of organic compounds and to interact with unsaturated chemical bonds [15]. The antimicrobial effect of ozone is due to damage to the cytoplasmic membrane. The effect of ozone on bacterial cell membrabes is via oxidation of the lipid and lipoprotein components, and there is also evidence of interactions with proteins. Ozone alters intercellular contents via secondary oxidation effects [17]. Interestingly, studies on E.coli showed that ozone penetrated the cell membranes, reacted with cytoplasmic contents, and cleaved to plasmid DNA thereby impairing bacterial procreation [18]. Only microbial cells are susceptible to the oxidative damage of ozone because of the powerful anti-oxidative and DNA/ RNA repairing abilities of healthy human cells [19, 20].
Aqueous ozone is highly biocompatible with human oral epithelium, and periodontal cells [21]. During World War I, ozone was used to treat infected wounds [22]. Indications for external ozone applications include poorly healing wounds, skin ulcers, burns, fungal lesions, herpes simplex, herpes zoster, lymphedema, and gangrene [16, 17].
Ozonated water has antiseptic and healing capabilities [21, 23], and its antimicrobial, disinfectant and biocompatibility make it suitable for dental use. Specifically, the reduction of signs of gingivitis and periodontitis following ozone use have been noted in several clinical studies [19, 21, 22, 23]. Ozone therapy reduces the growth of A. actinomycetemcomitans, P. gingivalis, and T. forsythia23. Ozone has been used in the treatment of early carious lesions, sterilization of cavities, root canals, periodontal pockets, epithelial wounds, bleaching of discolored endodontically treated teeth, desensitization of sensitive teeth, treatment of peri-implantitis, a rinse for avulsed teeth and as a denture cleaner [24].
Considering the advantages of ozone mouthwash, the aim of this randomized single blinded clinical study was to evaluate the effectiveness of a new electrical oral health ecosystem (invented by PURECARE Dental Ltd.), powered by ozonated water that generates medical grade ozone from oxygen on-demand, for the prevention of gingivitis and promotion of gingival health.
Specific Objectives: a) To determine the effectiveness of the “Purecare” ozonated water oral cleansing method as compared to a regular widely used mouthwash (“Colgate Plax”) in the prevention of gingival bleeding. b) To determine whether there were adverse effects following the use of the “Purecare” electrically ozonated water mouthwash device.
Materials and Methods
The study was approved by the human subject’s ethics board of Hadassah research ethics committee - IRB, 0302- 18-HMO and was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013. Eighty-four patients were screened for moderate gingivitis using the Silness & Löe Gingival Index (GI, 1967) [25] (described below) at the “YAD- SARA” dental center in Jerusalem, Israel. 55 volunteers were diagnosed with moderate gingivitis and met the inclusion criteria listed below. All participants gave full informed consent.
Selection Criteria and Study Sample
Inclusion Criteria a) Over 18 years’ old
b) Systemically healthy c) No need for extensive prosthodontic treatment d) No periodontal treatment within a year prior to the study e) No periodontal disease requiring surgical periodontal care f) At least 20 functional teeth (preferably without crowns or extensive restorations). g) Mild to moderate gingivitis Exclusion Criteria a) Unable or unwilling to sign the informed consent form b) Unable to satisfactorily perform routine oral hygiene procedures c) Pregnant d) Taking medications e) Have removable dental prostheses or fixed orthodontic appliances. f) Smoke The 55 volunteers were randomly divided into three groups. On entering the examination room, participants were requested to blindly draw one of three notes from a covered hat. Note 1 recruited to group 1 (study group); note 2 recruited to group 2 (control 1); note 3 recruited to group3 (control 2). They were instructed not to expose their affiliation to the examiner.
Group 1 participants were instructed to brush their teeth at home twice a day and visited the trial site 3 times a week for 4 weeks for ozone treatment with the PURECARE device (see Fig 2 and device description below). During the first visit the participants were shown how to use the PURECARE device and operated it alone on subsequent visits.
Group 2 was instructed to brush their teeth twice a day and to use a regular mouth rinse (COLGATE® PLAX PEPPERMINT) every evening for 4 weeks. The manufacturers of this mouthwash claim that it combats plaque and bacteria for up to 12 hours, protects gums and has a refreshing taste.
Group 3 participants were instructed to brush their teeth twice a day for 4 weeks, and not use a mouthwash.
All participants used the same toothpaste (COLGATE TOTAL® CLEAN MINT) with Stannous Fluoride (0.454%) indicated for the prevention of cavities, gingivitis and to protect against sensitivity with a manual Colgate® 360® toothbrush. All participants were given oral hygiene instructions by a registered dental hygienist. All participants visited the clinic at 3 time points: Day 0, before treatment (t0) Day 14 (t1) and Day 30 (t2), at each visit the entire oral cavity was examined for any adverse effects (irritation, sensitivity etc.)- including all hard and soft tissues, with an emphasis on the gingivae and gingival margins. At each visit the GBI index [26] and the GI index [25] were determined. The examiner was blind to the treatment received by the participant (Chart 1, Figure 1).
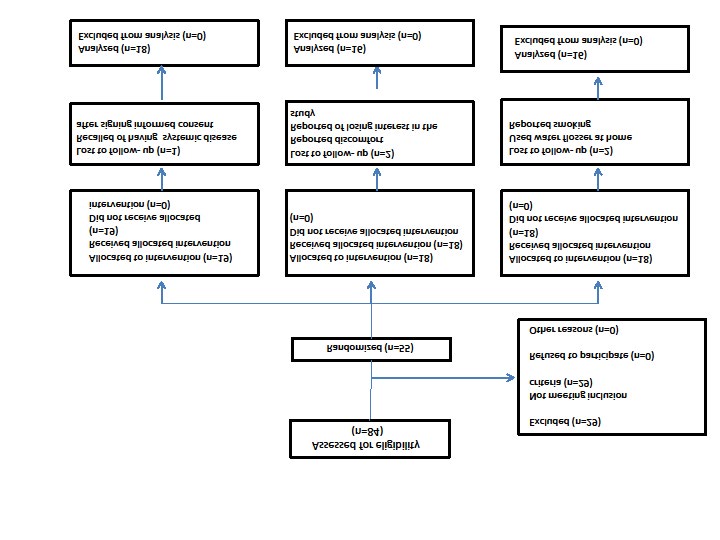
Chart 1: The chart summarizes the timeline of the treatment and the clinical measurements.

The PURECARE device can produce ozonated water from O2 and tap water. The Ozonated water was used immediately after preparation and ozone concentration was between 1.25-2.0 ppm.
Fundamentals of Ozonated water preparation a) Oxygen flows from the capsule and contacts the Ozone electrode.
b) The electrode transforms the oxygen into O3 using the Electrical Corona discharge technique.
c) The ozone gas is dissolved into the water using a micron diffuser.
Clinical Outcome Variables
1) Bleeding was scored according to the Carter & Barnes, Gingival Bleeding Index (GBI, 1974) [26]. This index records the presence or absence of gingival inflammation as determined by bleeding from interproximal gingival sulci after passing un-waxed dental floss into the sulci. The mouth is divided into six segments and flossed in the following order; upper right, upper anterior, upper left, lower left, lower anterior and lower right. After passing the floss, the examiner waits thirty seconds then inspects each segment. Bleeding is recorded as present or absent. For each patient a Gingival Bleeding Score is obtained by noting the total units of bleeding and the total susceptible areas examined.
2) Gingival inflammation was scored according to the Silness & Löe Gingival index (GI, 1967) [25]. The Silness & Löe Gingival index analyzes marginal and interproximal tissues, a score of 3= Normal gingivae;
1=Mild inflammation-slight change in color and slight edema but no bleeding on probing; 2=Moderate inflammation–redness, edema and glazing, bleeding on probing; 3=Severe inflammation-marked redness and edema, ulceration with tendency of spontaneous bleeding. The overall GI is calculated by adding the values for each tooth and dividing by the number of teeth examined. A score of 0.1-1.0 = mild inflammation; 1.1-2.0=moderate inflammation from, and 2.1-3.0 signifies severe inflammation. This index assesses the severity of gingivitis based on color, consistency, and bleeding on probing, and the scores are from four dental surfaces: mesial, distal, buccal/labial, lingual.
Before entering the trial, subjects answered a written questionnaire with three questions 1) gender (Male/ Female); 2) if they had visited a dentist in the year prior to the study (Yes/No); 3) age. Adverse effects to soft and hard tissue were measured clinically and by self-report.
Statistical Analysis
Data were analyzed using SPSS software version 25.0. (SPSS Inc. Headquarters, 233 S. Wacker Drive, 11th floor Chicago, Illinois 60606, USA). Significance levels were set at 0.05. Baseline characteristics are presented as means and standard deviations for continuous variables and as frequencies and percentages for categorical variables. Differences between groups were evaluated using Kruskal- Wallis tests for continuous variables and by Chi-Square test for categorical variables. Mann-Whitney non-parametric tests were used to measure the differences between two independent groups. Improvement from baseline to T1 and T2 was tested using the non-parametric Friedman tests followed by the Wilcoxon rank test for paired groups.
Results
Five participants (one from the test group and two from each of the other groups) were lost to follow up, therefore data from 50 subjects were analyzed. Demographic and the baseline findings are detailed in Table 1. There were significantly more men in the control group. The majority of the study participants visited their dentist within the last year with no statistically significant differences between the groups. There was no statistically significant difference between the groups in the clinical indices measured at baseline (T0). Specifically, the GI mean (SD) was 1.59 (0.31) for the test group, 1.49 (0.23) for group 2 and 1.49 (0.27) for group 3. There was no statistically significant difference in the GI max between the groups at (T0). The GBI mean (SD) was 12.4 (7.5) for the test group, 13.3 (4.8) for group 2 and 11.7 (5.5) for group 3.
| Test group | Group 2 | Group 3 | P | |
|---|---|---|---|---|
| Parameter | PURECARE device + Regular oral hygiene | Mouth wash + Regular oral hygiene | Regular oral hygiene | |
| n=18 | n=16 | n=16 | ||
| Sex (F), n (%) | 12(67) | 10(62) | 4(25) | 0.03 |
| Dental visit in the last year | 12(57) | 12(75) | 10(63) | 0.873 |
| Age (years) | 32±8.1 | 28±9.1 | 36±15 | 0.174 |
| GI | 1.59±0.31 | 1.49±0.23 | 1.49±0.27 | 0.43 |
| GI Max | 2.06±0.23 | 2.0±0.0 | 2.06±0.25 | 0.625 |
| GBI | 12.4±7.5 | 13.3±4.8 | 11.7±5.5 | 0.754 |
Table 1: Demographic and clinical findings at baseline.
Values are presented as mean + SD or n (%). GI, gingival index; GBI, gingival bleeding index; GI max, worst score measured Table 1: Demographic and clinical findings at baseline.
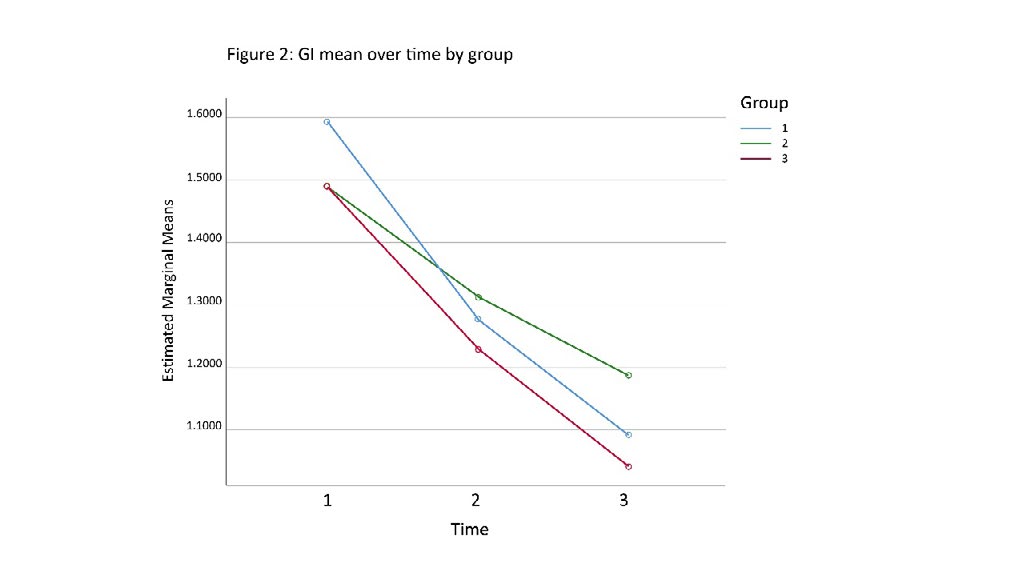
The study group showed significant continuous improvements in all outcome measures after ozone treatment (Table 2). The GI mean (SD) improved from 1.59 (0.31) at baseline, to 1.28 (0.32) after two weeks of treatment, and to 1.09 (0.32) after four weeks of treatment. The number of bleeding areas also decreased significantly, GBI mean (SD) was 12.4 (7.5) at baseline, 6.83 (6.0) after two weeks of treatment, and 5.89 (5.21) after four weeks of treatment.
| Parameter | T0 | T1 | T2 | P012 | P01 | P02 |
|---|---|---|---|---|---|---|
| GI Mean | 1.59±0.31 | 1.28± 0.32 | 1.09± 0.32 | <0.001 | 0.001 | <0.001 |
| GI Max | 2.06±0.23 | 1.72 ±0.46 | 1.61 ±0.50 | 0.003 | 0.01 | 0.002 |
| GBI | 12.4±7.5 | 6.83 ±6.0 | 5.89 ±5.21 | <0.001 | <0.001 | <0.001 |
Table 2: Changes over time in the study group.
Values are presented as mean + SD. GI, gingival index; GBI, gingival bleeding index; GI max, worst score measured. T0, baseline; T1, after 2 weeks of treatment, T2, after 4 weeks of treatment P012, difference between the indices at T0, T1, T2. P01, difference between the indices at T0, T1. P02, difference between the indices at T0, T2. Table 2: Changes over time in the study group.
| Parameter | Group 1 | Group 2 | Group 3 | P123 | P12 | P13 |
|---|---|---|---|---|---|---|
| After four weeks of treatment | ||||||
| GI Mean | 0.31±0.32 | 0.26±0.38 | 0.18±0.25 | 0.458 | 0.652 | 0.172 |
| GI Max | 0.33±0.48 | 0.31±0.48 | 0.19±0.54 | 0.669 | 0.901 | 0.415 |
| Num Bleeding | 5.56±4.7 | 6.93±4.1 | 5.56±4.6 | 0.601 | 0.37 | 0.997 |
| After four weeks of treatment | ||||||
| GI Max | 0.44±0.51 | 0.44±0.51 | 0.19±0.40 | 0.229 | 0.969 | 0.117 |
| GI Mean | 0.50±0.29 | 0.48±0.32 | 0.30±0.22 | 0.121 | 0.623 | 0.035 |
| Num Bleeding | 6.50±5.1 | 6.31±4.2 | 6.0±5.2 | 0.956 | 0.909 | 0.78 |
Table 3: The long-term observed improvement was greatest in the study group for all outcomes. After four weeks of treatment, the
Differences between the groups are present in Table 3. The long-term observed improvement was greatest in the study group for all outcomes. After four weeks of treatment, the mean GI was significantly lower and improved earlier compared to group 3.
The differences between GI mean and GI max were not significantly different between the groups 1 and 2.
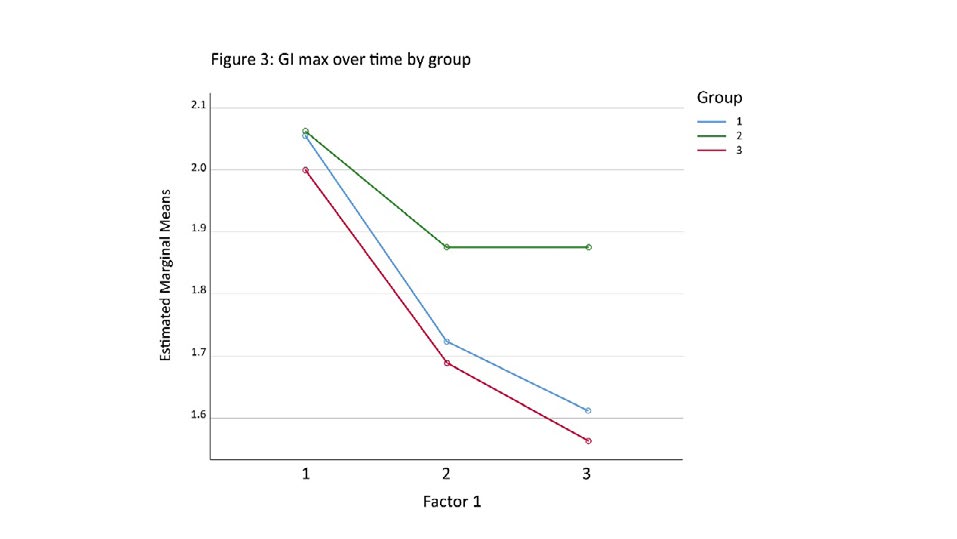
Figures 2 and 3 present similar improvements for the study group and the control groups for the GI measures. The study group showed a clearly more improved tendency, but not statistically significance.
Discussion
Ozone has many clinical applications [27], and is particularly useful in dentistry when in the form of ozonated water [28]. For example, ozonated water improves wound healing by increasing oxygen availability, serves as a hemostatic agent and as a disinfectant. Ozonated water has antimicrobial, anti-inflammatory and oxidizing effects [29]. There was no adverse effect reported, this is in accordance with other studies [18, 19] indicating biocompatibility.
Many studies have reported that ozonated water is a beneficial adjunct to treatment for periodontitis [30, 31, 32, 33]. There are only a few clinical trials on the influence of ozone on gingivitis. This is surprising considering that gingival inflammation in response to bacterial plaque accumulation is the key risk factor for the onset of periodontitis [34]. In vitro studies Huth KC, et al., Broadwater WT, et al. and Tonetti MS, et al. [35, 36, 37] found that ozone has potent bactericidal activity against periopathogenic bacteria and is not cytotoxic to human oral epithelial cells. Hayakumo S, et al. [33], reported that ozone in the form of nano- bubbles had bactericidal activity against periodontal pathogens including Porphyromonas and Aggregabitacter actinonomycetemcomitans. Huth KC, et al. [35] found that aqueous ozone at 1.25 ppm reduced the levels of P.gingivalis and A. actinomycetemcomitans by approximately 60% after 1 min of exposure.
Considering that gingivitis is the most prevalent form of periodontal inflammation [35] and that plaque induced gingivitis is the most prevalent form of gingivitis, management of gingivitis is essential in the prevention of periodontitis [38]. The present study shows that ozonated water at concentrations of 1.5-2 ppm adjunct to regular oral hygiene maintenance caused a statistically significant improvement in the clinical signs of gingivitis. This trial was unique and our findings are important due to the lack of clinical data. Our evidence that ozonated water at the concentrations of 1.5-2 ppm used as a mouthwash 3 times a week significantly reduced the mean GI, and GBI in patients with moderate gingivitis is strong.
The adjunctive effect of regular water oral irrigators in addition to tooth brushing is inconclusive. In their review, Husseini, et al. [39] concluded that oral irrigators using water do not reduce plaque and may be slightly beneficial compared to brushing alone. Katti SS, et al. [40], compared the clinical effect of oral irrigator using ozonated water to one using saline and concluded that ozonated water was superior.
When considering the chemical agents used to control periodontal bacteria there is broad consensus that Chlorhexidine (despite its adverse effects including staining the teeth and tongue), provides significant reduction in gingival inflammation [41]. Furthermore, Parkar SM, et al. [42] demonstrated that ozonated water was as effective as 0.2% chlorhexidine in reducing gingivitis and Indurkar M, et al. [43] concluded that ozonated oil and 1% chlorhexidine gel, are similarly effective in maintaining and improving gingival health. Our study showed that ozonated water as used in the study group and regular mouthwash both independently reduced gingival inflammation significantly. The effect of the ozonated water can be attributed to the antimicrobial effects of ozone against periodontic pathogens [44]. Although the differences between the two modes were similar, the improvement was noted more rapidly in the study group. The rapid action of ozone against pathogens is well documented, e.g. Filippia A [45] found that one molecule of ozone kills pathogenic organisms 3500 times faster than chlorine.
Conclusion
The use of ozonated water in dentistry is becoming more popular. Extensive research over the past 50 years has demonstrated the utility of ozonated water for infection control. This trial strongly supports the use of Ozonated water in the treatment of gingivitis.
References
-
Nazir MA (2017) Prevalence of periodontal disease, its association with systemic diseases and prevention. International Journal of Health Sciences 11(2): 72-80.
-
Tonetti ST, Jespen S, Jin L, Corgel JO (2017) Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J Clin Periodontol 44(5): 456-462.
-
Williams RC (1990) Periodontal Disease. N Engl J Med 322: 373-382.
-
Page RC (1986) Gingivitis. Journal of Clinical Periodontology 13(5): 345-355.
-
Trombelli L, Farina R, Silva CO, Tatakis DN (2018) Plaque-induced gingivitis: Case definition and diagnostic considerations. J Clin Periodontol 45(20): 44-67.
-
Albandar JM, Rams TE (2008) Global epidemiology of periodontal diseases: an overview. Periodontology 2000 29(1): 7-10.
-
(2001) Treatment of plaque-induced gingivitis, chronic periodontitis, and other clinical conditions. J Periodontol 72(12): 1790-1800.
-
Sreenivasan P, Prasad K, Javali S (2016) Oral health practices and prevalence of dental plaque and gingivitis among Indian adults. Clin Exp Dent Res 2(1): 6-17.
-
Tonetti MS, Chapple ILC, Jepsen S, Sanz M (2015) Primary and secondary prevention of periodontal and peri- implant diseases Introduction to, and objectives of the 11th European Workshop on Periodontology consensus conference. J Clin Periodontol 42(16): 1-4.
-
Pihlstrom BL, Michalowicz BS, Johnson NW (2005) Periodontal diseases. Lancet 366(9499): 1809-1820.
-
Caton JG, Armitage G, Berglundh T, Chapple ILC, Jepsen S, et al. (2018) A new classification scheme for periodontal and peri-implant diseases and conditions-Introduction and key changes from the 1999 classification J Clin Periodontol 45(20): 1-8.
-
Westfelt E (1996) Rationale of mechanical plaque control. Journal of Clinical Periodontology 23(3): 263- 267.
-
Jafer M, Patil S, Hosmani J, Bhandi SH, Chalisserry EP, et al. (2016) Chemical Plaque Control Strategies in the Prevention of Biofilm-associated Oral Diseases. J Contemp Dent Pract 17(4): 337-343.
-
James P, Worthington HV, Parnell C, Harding M, Lamont T, et al. (2017) Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst Rev 3(3): CD008676.
-
Schonbein C Notice of C Sch., the discoverer of ozone. Annual Report of the Board of Regents of the Smithsonian Institution 1868, Washington, DC, US Government.
-
Sunnen G (1988) Ozone in Medicine: Overview and future directions. Journal of Advancement in Medicine 1(3): 159-174.
-
Viebahn R (1999) The Use of Ozone in Medicine. Odrei Publishers, Iffezheim.
-
Ishizaki K, Sawadaishi D (1987) Effect of ozone on plasmid DNA of scherichia coli in situ. Water Res 21(7): 823-828.
-
Pietrocola G, Ceci M, Preda F, Poggio C, Colombo M (2018) Evaluation of the antibacterial activity of a new ozonized olive oil against oral and periodontal pathogens. J Clin Exp Dent 10(11): 1103-1108.
-
Mudd JB, Leavitt R (1969) Reaction of ozone with amino acids and proteins. Atmos Environ 3(6): 669-681.
-
Gupta G, Mansi B (2012) Ozone therapy in periodontics. J Med Life 5(1): 59-67.
-
Werkmeister H (1985) Subatmospheric treatment of therapy-resistant wounds and ulcerations. Ozo Nachrichten 4: 53-59.
-
Brauner A (1991) Clinical investigation of the therapeutic success of ozonized water for gingivitis and periodontitis 2: 48-50.
-
Gopalakrishnan S, Parthiban S (2012) Ozone-A New Revolution in Dentistry. J Bio Innov 1(3): 58-69.
-
Löe H (1967) The Gingival Index, the Plaque Index and the Retention Index Systems. The Journal of Periodontology 38(6): 610-616.
-
Carter HG, Barnes GP (1974) The Gingival Bleeding Index. Journal of Periodontology 45(11): 801-805.
-
Chitnis P, Bhusari BM, Sah N, Banavali KA (2013) Ozone therapy: A New Revolution In Periodontics. International Journal of Innovative Research & Development 2(5): 1173-1180.
-
Gupta G, Mansi B (2012) Ozone therapy in periodontics. Journal of Medicine and Life 5(1): 59‐67.
-
Baysan A, Whiley R (2004) Anti-microbial effects of novel ozone generating deviceon microorganisms associated with primary root carious lesion in vitro. Caries Res 34(6): 498-501.
-
Katti SS, Chava VK (2013) Effect of ozonized water on chronic periodontitis – a clinical study. J Int Oral Health 5(5): 79-84.
-
Kshitish D, Laxman VK (2010) The use of ozonated water and 0.2% Chlorhexidine in the treatment of periodontitis patients: a clinical and microbiological study. Indian J Dent Res 21(3): 341-348.
-
Dadwad V, Gupta S, Kumar K, Sethi M, Masamatti S (2011) Changing paradigm in pocket therapy – Ozone versus Conventional irrigation. Int J Pub Health Den 2(2): 7-12.
-
Hayakumo S, Arakawa S, Takahashi M, Kondo K, Mano Y, et al. (2014) Effects of ozone nano-bubble water on periodontopathic bacteria and oral cells - in vitro studies. Sci Technol Adv Mater 15(5): 1-7.
-
Murakami S, Mealey B L, Mariotti A, Chapple ILC (2018) Dental plaque–induced gingival conditions. J Clin Periodontol 45(20): 17-27.
-
Huth KC, Jakob FM, Saugel B, Cappello C, Paschos E, et al. (2006) Effect of ozone on oral cells compared with established antimicrobials. Eur J Oral Sci 114(5): 435- 440.
-
Broadwater W T, Hoehn RC, King PH (1973) Appl. Microbiol 26: 391-393.
-
Tonetti MS, Chapple ILC, Jepsen S, Sanz M (2015) Primary and second‐ary prevention of periodontal and peri‐implant diseases. J Clin Periodontol 42(16): 1‐4.
-
Quirynen M, Dadamio J, Van den Velde S, et al. (2009) Characteristics of 2000 patients who visited a halitosis clinic. J Clin Periodontol 36(11): 970-975.
-
Husseini DE, Slot GA, Van der W (2008) The efficacy of oral irrigation in addition to a toothbrush on plaque and the clinical parameters of periodontal inflammation: a systematic review. International Journal Dental Hygiene 6(4): 304-314.
-
Sandeep SK, Chava VK (2013) Effect of Ozonised water on Chronic Periodontitis - A Clinical Study. Journal of International Oral Health 5(5): 79-84.
-
Herrera D (2013) Chlorhexidine mouthwash reduces plaque and gingivitis. Evid Based Dent 14(1): 17-18.
-
Parkar SM, Shah K, Darjee N, Sharma A (2017) Efficacy of ozonated water and chlorhexidine mouth rinse against plaque and gingivitis: A randomized clinical trial. J Clin Sci 14(2): 81-85.
-
Indurkar M, Sanjeev VR (2016) Effect of ozonated oil and chlorhexidine gel on plaque induced gingivitis: A randomized control clinical trial. J Indian Soc Periodontol 20(1): 32-35.
-
Baysan A, Whiley RA, Lynch E (2000) Antimicrobial effect of a novel ozone-generating device on microorganisms associated with primary root carious lesions in vitro. Caries Res 34(6): 498-501.
-
Filippia A (2001) The effect of ozonated water on epithelial wound healing. Douch Dent J 143: 9.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells