Decontamination of Hard Tissue Using a Scanning Pulsed 9.3-μm CO2 Laser
Purpose: The aim of the study was to evaluate the use of a scanning 9.3-µm CO2 laser beam to reduce or eliminate bacteria on hard tissue as a new method of non-specific decontamination to prevent cross-contamination during dental or medical procedures. Methods: A low energy level of a 9.3-μm CO2 laser beam was designed to deliver overall uniform photothermal energy in a 2-mm-diameter beam to eliminate bacteria on the surface of dental enamel without damaging the surface of the tooth. The study was conducted in two parts. The first part consisted of 10 human molars polished to a 1-μm finish and inoculated with S. mutans. The bacteria were stained with methylene blue and imaged through cross-polarization microscopy, and the area of the imaged surface containing bacteria was analyzed using ImageJ. The second part of the study consisted of 20 uncleaned extracted human molars used for evaluating cross-contamination of bacteria by measuring bacteria Colony Forming Units (CFU) ejected during an aerosol-generating procedure in vitro. Tryptic soy agar (TSA) plates were used to collect bacteria while cutting enamel. The TSA plates were incubated at 35o C for 24 hours, after which bacteria colonies were counted. Results: Examination using cross-polarization microscopy and imaging showed that the CO2 laser eliminated >98% of bacteria on the surface without altering the surface of teeth and similarly >98% in the aerosol/splatter from cutting of the enamel. Conclusion: The 9.3-μm CO2 laser resulted in nearly a complete elimination of viable bacteria.
Background
Given the challenges brought on by the severe acute respiratory syndrome coronavirus (SARS-CoV-2) pandemic, it has become increasingly important for clinicians to improve upon the sterilization and safety techniques used in their practices [1, 2, 3]. In particular, the relatively high risk of cross contamination and infections during aerosol-generating dental procedures has motivated the need for methods to eliminate bacteria and other oral pathogens [4, 5].
Common methods of decontaminating tooth structures include the use of the exogenous substances such as chlorhexidine, natural substances such as antimicrobial peptides and lactoperoxidases, and mechanical methods such as ultrasonic scalers [6, 7, 8]. However, several key drawbacks to these methods must be considered. The use of chlorhexidine mouthwash has been noted to have potential side effects including cytotoxicity, tooth staining, altered taste, and urticarial [6, 9, 10]. Recent studies have also shown the danger of mechanical decontamination methods, including the use of ultrasonic scalers. Live pathogens in the mouth can mix with oral fluids and be projected by high- energy drilling instruments, producing pathogen-containing aerosols that pose health risks to clinicians who operate in close proximity to their patients [11, 12].
Lasers of varying wavelengths have been used for decades in oral surgery and in some cases, laser treatment has become state of the art as compared to conventional techniques to disinfect root canals, periodontal pockets, cavity preparations and sites of peri‐implantitis [13, 14, 15, 16, 17]. The 9.3-μm CO2 laser has a strong absorption of hydroxyapatite in teeth, which allows for a rapid heat accumulation near the surface of the tooth [18, 19]. In soft tissues, the 9.3-μm CO2 laser is absorbed by water and therefore is very effective for the surgery of soft tissues, in addition to providing hemostatic and bactericidal effects [20, 21]. This study aimed to evaluate the efficacy of a 9.3-μm CO2 laser in eliminating bacteria on the dental enamel surface using relatively low power irradiation and in reducing the viability of bacteria that may be released into the air via aerosols/splatter generated while cutting enamel.
Methods
Laser Settings
A 9.3 μm CO2 laser (Solea, Convergent Dental, Inc., Needham, MA) was used with a modified design to allow for low power irradiation. The native beam diameter was collimated to a diameter of 2 mm (measured by 1/ e2 method) at the output of the handpiece. The beam was scanned over the irradiated surface for 5 seconds at a pulse scan rate of 315 Hz using a pair of computer-controlled mirrors in a uniform geometric pattern with a point-spacing of 0.9 mm between centers of each adjacent single laser spot and a randomization of point sequencing. This distribution of single irradiation spots was developed to distribute the accumulation of heat energy from irradiation more uniformly over a larger area to prevent damage and provide a broader treatment area. The average power was 3 W.
Experimental Designs
Two different experiments were conducted in the study: 1) surface decontamination to quantify the elimination of bacteria from the surface of polished teeth referred to and 2) cross-contamination to measure the amount of bacteria colony forming units (CFU) that were ejected in the aerosol/ splatter during an in vitro cutting procedure before and after decontamination with laser irradiation.
Surface Decontamination
A total of 10 human molars were obtained, mounted, and polished to a 600-grit finish (Therametrics, Inc Therametric Technologies, Inc., Noblesville, IN). Then, the samples were individually hand polished with a 1-μm diamond suspension to provide a surface finish using an automated polisher, Metkon Forcipol 1V (Kemet International, Kent, ME). The samples were then inoculated with Streptococcus mutans in Tryptic Soy or Blood Agar (470179-170, VWR, Radnor, PA) for 24 hours at 37oC. After incubation, samples were air dried. The right half of each sample was mas masked by a razor blade with the sharp edge touching the middle of the enamel surface. The aiming beam from the handpiece was positioned in the center of the enamel surface, and laser irradiation following the above parameters was performed.
Cross-Contamination
To investigate a nonspecific decontaminating effect from the laser, a total of 20 human molars were extracted, gently cleaned of tissues and blood, and stored in a container with paper towels soaked in distilled water to prevent dehydration and refrigerated for less than 3 months before use. Of the 20 molars, 10 were irradiated at the recommended cutting settings of 30% cutting speed (~8.3 W), 9 mL/min mist flow, and low air pressure (10 psi) using the 1.25 mm spot size. The entire buccal or lingual surface was cut. These were referred to as the non-treated group. For the other 10 molars, all sides of the teeth were first treated with the decontamination laser irradiation (referred to as the treated group), and then cut using the same settings as the untreated control group.
A sedimentation bacteria collection method [22, 23] was used with tryptic soy blood agar (TSA) plates (Eurofins EMLab P&K laboratories, Marlton, NJ) to measure the amount of bacteria released into aerosols/splatter while cutting the teeth in both groups. Agar plates were positioned 8 cm from the tooth at an angle of ~45° above the test area such that any aerosolized bacteria would settle onto the agar plate in the direction that a clinician might be located (the distance was chosen to increase the collection of aerosols and splatter and improve the signal-to-noise ratio). The plates were exposed to the generated aerosol during a 10 second cutting period. After 10 seconds, the agar plates were lidded and incubated at 37oC for 24 hours. Bacteria colonies were then imaged and counted for both groups.
Standard aseptic techniques were followed. Prior to the experiment, all surfaces involved in the set up were cleaned with alcohol disinfecting wipes and 70% ethanol. Gloves were worn during the experiment and were cleaned with 70% ethanol before handling sterile plates. Mounting devices holding the plates and teeth were both cleaned with alcohol disinfecting wipes between each measurement. Additionally, the experiment was performed in a fume hood which was turned on for 30 seconds between measurements to minimize cross-contamination of samples.
Image Analysis for Surface Decontamination
A semi-automated approach using ImageJ [24] was applied to quantify the percentage of area covered by bacteria in microscope images of tooth surfaces obtained before and after application of the laser, as shown in Figure 1. Each pair of images, one of the non-irradiated tooth surface and another post-lasing, was analyzed side-by-side. Both images were uploaded to ImageJ and a circle of diameter
550 pixels, matching the maximum uniformly illuminated region, was cropped from the same location in each image. The images were then inverted, and the color threshold values for hue, saturation, and brightness were adjusted until identical values were applied to both images such that bacteria (in white) was clearly distinguishable from the background (in black) with minimal signal loss. This was verified by comparing each processed image to its original. Next, the ‘analyze particles’ feature was used to highlight the areas above the selected thresholds, and the percentage of area covered by bacteria was determined as the ratio of the highlighted region to the total area of the circle.
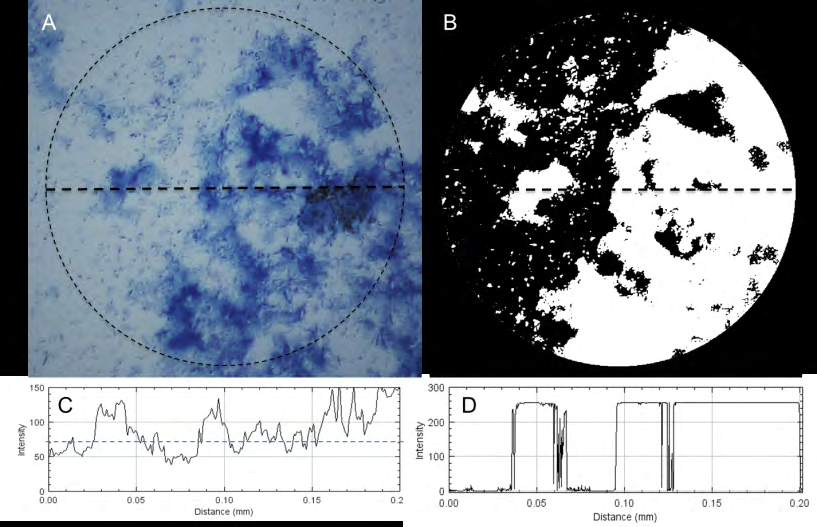
Figure 1: Depiction of the analysis for determining % area covered by methylene blue-stained bacteria on the dental enamel surface using cross-polarization microscopy. A) A pre-processed image is shown with the circle representing the analyzed area, and a horizontal dashed line corresponding to a profile of the intensity of pixels along the line (C). B) A post-processed image after assigning a color threshold is shown with a horizontal line, corresponding to a profile of intensity along the line (D).
Image Analysis for Cross-Contamination
Images for each TSA plate in the cross-contamination study were taken under identical imaging conditions. A semi- automated approach using ImageJ [24] was done to obtain bacteria colony counts for each TSA plate. The boundaries around the central regions of the TSA plates in the images were cropped and grayscale image thresholds were adjusted such that bacteria colonies (white) were discernible from the background (black), which worked due to the increased absorption of light from the bacterial colonies. To ensure an accurate representation of bacteria colonies, each new black and white image was visually compared to its original. The ‘analyze particles’ feature was then used to provide a total count of the colonies on each plate.
Scanning Electron Microscopy of Bacteria on Surface
2 human molars were fixed by immersion in electron microscopy grade 2.5% glutaraldehyde and 2.0% paraformaldehyde in 0.1 M sodium cacodylate buffer, pH 7.4 (Polysciences, Inc. Warrington, PA), at refrigerator temperatures for 4 hours, after which the fixative was replaced with 0.1 M sodium cacodylate buffer, pH 7.4. Prior to imaging, the buffer was replaced with an ascending ethanol series (37%, 67%, and 95% at 10 minutes each on a shaker table), and three times 100% ethanol, at 10 minutes each change, on the shaker table. The 100% ethanol was then replaced with hexamethyldisilazane (Polysciences, Inc. Warrington, PA) for 10 to 15 minutes, after which the HMDS was removed and allowed to evaporate in the fume hood.
The samples were mounted on a custom-made 1.75-inch- diameter aluminum SEM stub using Leit-C-Plast plastic conductive carbon cement (SPI Supplies, West Chester, PA), sputter-coated with 8 nm of gold/palladium (Desk-V sputter coater and Au/Pd target from Denton Vacuum, Moorestown NJ), grounded with silver paint (SPI Supplies), and imaged in the vacuum chamber of a Quanta 450 ESEM- FEG environmental scanning electron microscope (Thermo Fisher MSD, Hillsboro OR) in Hi-Vac mode at 7.5 kV, spot 3, at a working distance of roughly 10 mm.
Results
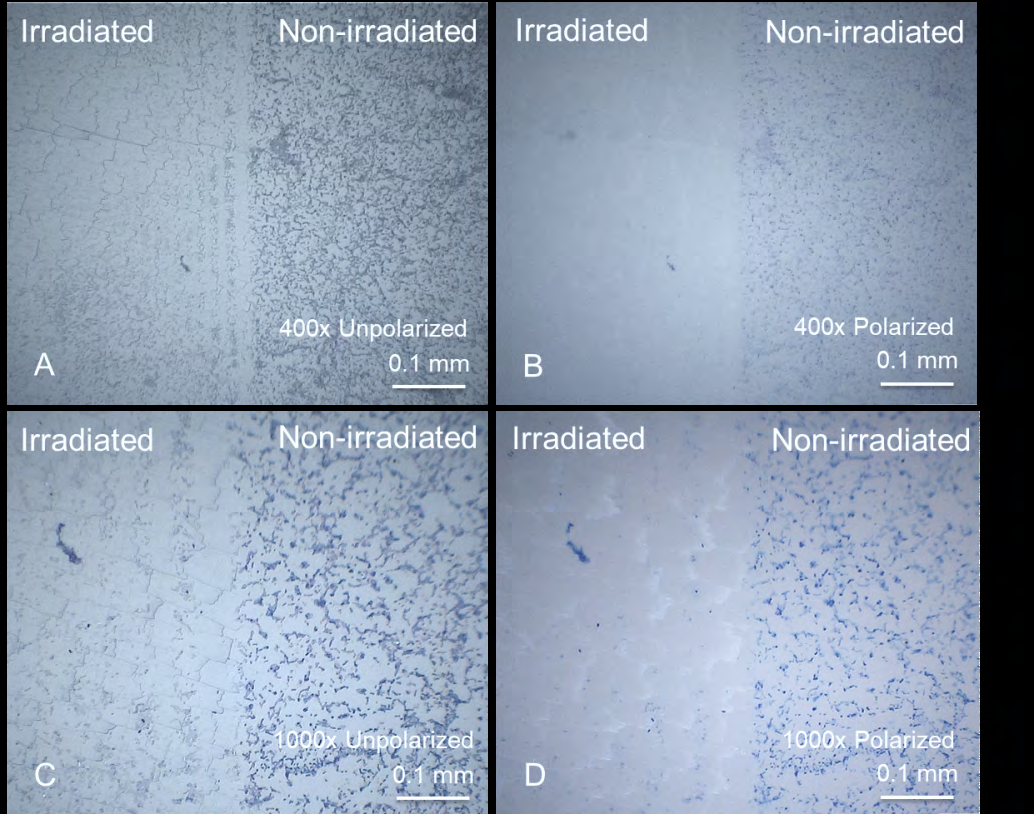
Figure 2 shows images of the methylene blue- stained bacteria on the enamel surface at 400x and 1000x magnifications, both with and without cross-polarization. The razor blade successfully masked the non-irradiated area and generated a clear vertical boundary between the irradiated and non-irradiated sides. Some diffraction effects from the edge of the blade were observed near the boundary. Additionally, a small degree of harmless superficial effects from irradiation were observed. Most of the bacteria were destroyed or removed from irradiation. Some residue from the bacteria was apparent in the unpolarized images and was verified by cross-polarization images mostly not to be intact bacteria.
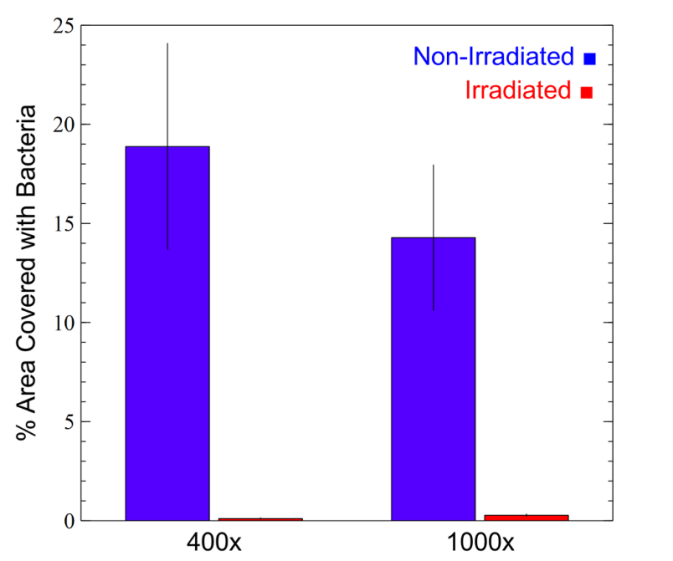
For the surface decontamination study, a summary of the calculated % area of the enamel surface covered in bacteria in the irradiated and non-irradiated areas at both 400x and 1000x magnifications is shown in Table 1 and plotted in Figure 3. At 400x, the mean % area covered with bacteria for the non-irradiated area was 14.3 ± 3.67, while for the irradiated area it was 0.276 ± 0.0635. This provided a percent reduction of bacteria on the surface of 98.1 ± 4.02. At 1000x, the mean % area covered with bacteria for the non- irradiated area was 18.9 ± 5.20, while for the irradiated area it was 0.109 ± 0.0318. This provided a similarly large percent reduction of bacteria on the surface of 99.4 ± 2.21. All values were statistically significantly different (p < 0.001).
| Magnification | Mean Non-Irradiated % Area Covered | Mean Irradiated % Area Covered | % Reduction in Bacteria from Irradiation | p-value (95% CI) |
|---|---|---|---|---|
| 1000x | 14.3 ± 3.67 | 0.276 ± 0.0635 | 98.1 ± 4.02 | p < 0.001 |
| 400x | 18.9 ± 5.20 | 0.109 ± 0.0318 | 99.4 ± 2.21 | p < 0.001 |
Table 1: Mean Reduction in % Area Covered with Bacteria from Laser Irradiation
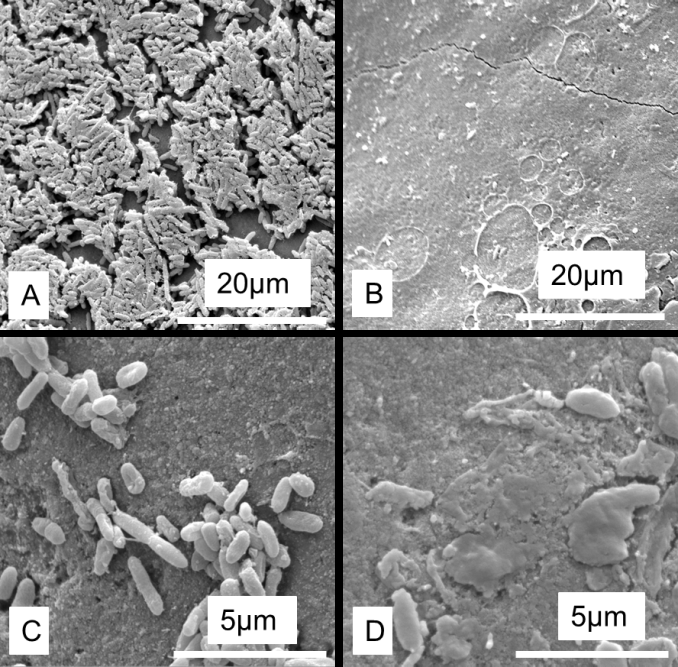
SEM images revealed a significant presence of bacteria on the inoculated molars, with some areas having dense biofilms developing, as shown in Figure 4A and 4C. After irradiation with the CO2 laser, a substantial reduction in bacteria on the enamel was observed, leaving only some residue from the biofilm. Damage to the enamel was not observed, which exception to some minor sub-micron crazing lines and occasional signs of surface pre-melt.
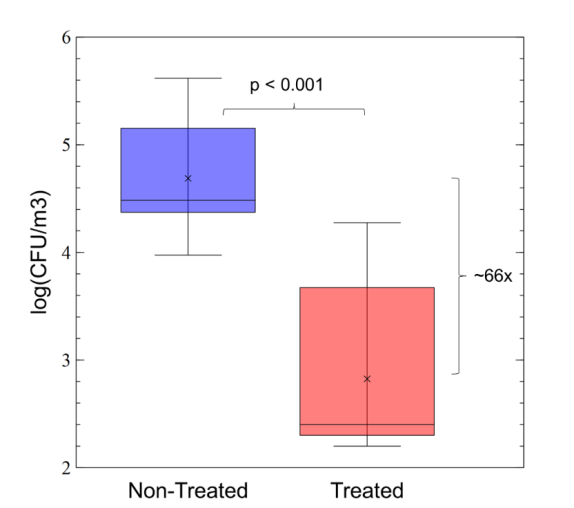
For the cross-contamination study, CFU from collected bacteria during an aerosol-generating procedure are shown in Figure 5. A log-transformation of the data was used for analysis, which showed a 66x reduction in CFU caused by a pre-treatment with decontaminating laser irradiation (p < 0.001).
Discussion
In part due to the recent pandemic, oral procedures have been of particular concern due to their inherent generation of aerosols and splatter [1–3], which exposes dental practitioners to potential harm. An approach to decontaminate tissues in a non-specific way may be highly desirable to reduce the transmission of pathogens. Lasers provide one potential avenue to avoid the use of potentially cytotoxic substances while still achieving a decontamination due to a controllable bulk tissue heating from absorption [18, 25]. This study aimed to demonstrate the capability of a 9.3-μm CO2 laser to decontaminate the surface of dental enamel, as measured through the removal of viable bacteria.
A novel method of measuring bacteria in a semi- automated manner through cross-polarization microscopy and methylene blue staining was used. Results from the surface decontamination study showed a reduction in bacteria from irradiation over 98% with fairly consistent results. This is not surprising when considering the thermal effects of irradiation, during which the surface temperature of enamel would reach several hundred degrees [18]. While some minor signs of superficial crazing were observed, this is not a concern since this minor surface effect would remineralize easily and has actually been reported to allow for slight reduction in caries formation or erosion, likely due to a removal of carbonate groups [26, 27, 28, 29]. Regardless, a substantial reduction in surface bacteria was presented here, so a reasonable assumption would be that even lower levels of irradiation may produce an effective decontamination with less evident surface effects from irradiation.
A similar >98% reduction in bacteria was found when uncleaned molars were pre-treated with the decontamination laser treatment prior to ablating the enamel. Since there was likely a broad spectrum of bacteria present on the molars, this helped to serve as an indication for the nonspecific nature of this laser decontamination. Such a rapid thermal decontamination at hundreds of degrees Celsius near the surface should allow for a broad-spectrum effect. A near- elimination of bacteria on the enamel surface after irradiation was observed under SEM, which further served to verify this decontaminating effect from the laser.
Lasers have been used for many years in oral surgery and in some cases, laser treatment has become state of the art as compared to conventional techniques to disinfect root canals, periodontal pockets, and sites of peri‐implantitis [30, 31]. The study presented here demonstrated that a 9.3-μm CO2 laser may be used for general hard tissue decontamination with minimal side effects. More importantly, the scanning mechanism of the laser beam along with the wavelength absorption of the laser allowed for a controlled thermal distribution of the heat on the surface were essential in not damaging the surface of the enamel in any significant way. Furthermore, the decontamination irradiation parameters used in this study may be modified to work for potentially any tissue type.
Conclusion
Tissue decontamination with the 9.3-μm CO2 laser can minimize the risk of exposure to live pathogens for clinicians who perform aerosol-generating procedures without the potential side-effects noted with other traditional decontamination methods.
References
-
Leggat PA, Kedjarune U (2001) Bacterial aerosols in the dental clinic: A review. Int Dent J 51(1): 39-44.
-
Harrel SK, Molinari J (2004) Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. J Am Dent Assoc 135(4): 429-437.
-
Miller RL, Micik RE, Abel C, Ryge G (1971) Studies on dental aerobiology: II. microbial splatter discharged from the oral cavity of dental patients. J Dent Res 50(3): 621-625.
-
Slots J, Slots H (2011) Bacterial and viral pathogens in saliva: Disease relationship and infectious risk. Periodontol 2000 55(1): 48-69.
-
Allison J, Currie C, Edwards DC, Bowes C, Coulter J, et al. (2020) Evaluating aerosol and splatter following dental procedures: addressing new challenges for oral healthcare and rehabilitation. biorxiv.org 00(1-12): 2020.06.25.154401.
-
Qiu W, Zhou Y, Li Z, Huang T, Xiao Y, et al. Application of Antibiotics/Antimicrobial Agents on Dental Caries. Biomed Res Int. 2020: 5658212
-
Magacz M, Kędziora K, Sapa J, Krzyściak W (2019) The significance of lactoperoxidase system in oral health: Application and efficacy in oral hygiene products. Int J Mol Sci 20(6): 1443.
-
Tunkel J, Heinecke A, Flemmig TF (2002) A systematic review of efficacy of machine-driven and manual subgingival debridement in the treatment of chronic periodontitis. J Clin Periodontol. 29(3): 72-81.
-
Rath SK, Singh M (2013) Comparative clinical and microbiological efficacy of mouthwashes containing 0.2% and 0.12% chlorhexidine. Dent Res J (Isfahan) 10(3): 364-369.
-
Chopra V, Chopra H, Sharma A (2013) Allergic urticaria: A case report of rare skin allergy with a common mouthwash. Indian J Dermatol 58(1): 85.
-
Aldahlawi SA, Afifi IK (2020) COVID-19 in Dental Practice: Transmission Risk, Infection Control Challenge, and Clinical Implications. Open Dent J 14(1): 348-354.
-
Bennett AM, Fulford MR, Walker JT, Bradshaw DJ, Martin MV, et al. (2000) Microbial aerosols in general dental practice. Br Dent J 189(12): 664-667.
-
Everett JD, Rossmann JA, Kerns DG, Al Hashimi I (2017) Laser Assisted Non-surgical Periodontal Therapy: A Double Blind, Randomized Clinical Trial. Open Dent J 11(1): 79-90.
-
Klinke T, Klimm W, Gutknecht N (1997) Antibacterial effects of Nd: YAG laser irradiation within root canal dentin. J Clin Laser Med Surg 15(1): 29-31.
-
Mehl A, Folwaczny M, Haffner C, Hickel R (1999) Bactericidal effects of 2.94 μm Er:YAG-laser radiation in dental root canals. J Endod 25(7): 490-493.
-
Romanos G, Ko HH, Froum S, Tarnow D (2009) The use of CO2 laser in the treatment of peri-implantitis. Photomed Laser Surg 27(3): 381-386.
-
Taku Kato D, Kusakari H, Hoshino E (1998) Bactericidal Efficacy of Carbon Dioxide Laser against Bacteria- Contaminated Titanium Implant and Subsequent Cellular Adhesion to Irradiated Area. Lasers Surg Med 23(5): 299-309.
-
Fried D, Seka WD, Glena RE, Featherstone JD (1996) Thermal response of hard dental tissues to 9‐ through 11‐μm CO2‐laser irradiation. Opt Eng 35(7): 1976-1984.
-
Featherstone JD, Nelson DG (1987) Laser effects on dental hard tissues. Adv Dent Res 1(1): 21-26.
-
Garg N, Verma S, Chadha M, Rastogi P (2015) Use of carbon dioxide laser in oral soft tissue procedures. Natl J Maxillofac Surg 6(1): 84-88.
-
Gutknecht N, Wilkert Walter C, Lampert F (1998) Bactericidal effect of the CO2 laser in the root canal: an in-vitro study. In: Featherstone JDB, et al. (Eds.), Lasers in Dentistry IV.
-
Sundri MI (2018) Bacteria and fungi levels in crowded indoor areas. IOSR J Environ Sci 12(9): 39-45.
-
Borrego S, Guiamet P, Gómez de Saravia S, Batistin P, Garcia M, et al. (2010) The quality of air at archives and the biodeterioration of photographs. Int Biodeterior Biodegrad 64(2): 139-145.
-
Schneider CA, Rasband WS, Eliceiri KW (2012) NIH Image to ImageJ: 25 years of image analysis. Nat Methods 9(7): 671-675.
-
Gnyawali SC, Chen Y, Wu F, Bartels KE, Wicksted JP, et al. (2008) Temperature measurement on tissue surface during laser irradiation. Med Biol Eng Comput 46(2): 159-168.
-
Badreddine AH, Couitt S, Donovan J, Cantor Balan R, Kerbage C, et al. (2020) Demineralization Inhibition by High-Speed Scanning of 9.3 µm CO2 Single Laser Pulses Over Enamel. Lasers Surg Med 53(5): 703-712.
-
Rechmann P, Le CQ, Kinsel R, Kerbage C, Rechmann BMT (2020) In vitro CO2 9.3-μm short-pulsed laser caries prevention-effects of a newly developed laser irradiation pattern. Lasers Med Sci 35(4): 979-989.
-
Rechmann P, Charland DA, Rechmann BMT, Le CQ, Featherstone JDB (2013) In-vivo occlusal caries prevention by pulsed CO2 -laser and fluoride varnish treatment--a clinical pilot study. Lasers Surg Med 45(5): 302-310.
-
Featherstone JDB, Fried D (2001) Fundamental interactions of lasers with dental hard tissues. Med Laser Appl 16(3): 181-194.
-
Jurič IB, Anic I (2014) The use of lasers in disinfection and cleaning of root canals: A review. Acta Stomatol Croat 48(1): 6-15.
-
Alshehri FA (2016) The role of lasers in the treatment of peri-implant diseases: A review. Saudi Dent J 28(3): 103-108.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells