CBCT-Based Evaluation of Root Canal Configurations of Mandibular Second Molars and Their Relation to Mandibular Canal in Central Gujarat Population-A Cross-Sectional Study
Aim: To evaluate root canal configurations of mandibular second molars and their relation to mandibular canal in Central Gujarat population using CBCT. Materials and Methods: In this retrospective study 260 CBCT volumes from 5 different CBCT centres in Central Gujarat region were collected between November 2020 till May 2021. The parameters of the second mandibular molars assessed were: Vertucci’s root canal configuration, number of canals, distance of root apex from mandibular canal, degree of curvature, presence of extra root and C-shaped canal. The association between age and distance from root apex to mandibular canal was evaluated as secondary outcome. Chi- square test was used to analyse the relationship between the distance of the mandibular molar from the mandibular canal and age, a p-value of < 0.05 was judged statistically significant. Data were statistically analysed using IBM SPSS Version 21.0. Results: 3 canals were discovered in 73.8% of mandibular second molars, with Type II and Type I root canal configurations in the mesial and distal roots, respectively. With a mean curvature of 21.880, the incidence of C-shaped and Radix canal topologies was determined to be 5.3 percent and 6%, respectively. The average distance of mesial and distal roots from the mandibular canal was 3.04 and 2.78 respectively which decreased with age. The average distance between root of the tooth and mandibular canal is more in males than females and as the age advances the distance increases. Conclusion: In Central Gujarat population, mesial root of mandibular second molar shows Vertucci’s type II canal configuration while distal root presented with type I. C shaped canal configuration with fused roots and Radix Entomolaris was seen in (5.4% and 2.3% respectively). Additionally, as the age advances the distance of root apex from mandibular canal increases.
Introduction
The essence of a successful root canal treatment revolves around the knowledge of normal as well as varied canal anatomy along with accurate diagnosis and treatment planning. Any disparity in root canal morphology and surrounding structure should be recognized before or during root canal therapy. Since root canal anatomy and root morphology may have specific racial impacts, different races’ root canal morphologies must be identified [1]. Furthermore, forensic dental identification plays a significant part in ascertaining the identity of unknown decedents due to the distinctiveness of racial dental patterns. Dental matches have been used to identify victims of multiple fatalities, including the September 2001 terrorist attacks and Hurricanes Katrina and Rita in 2005. Following the 2004 Indian Ocean tsunami, dental information was used to identify approximately 80% of non-Thai victims in Thailand [2, 3].
It is well established that mandibular second molars have the greatest number of anatomical diversities in their root canal system such as multiple foramina, additional canals, deltas, C shaped canal, lateral canals, Presence of extra root(radix), curvature, and, most important is its proximity to inferior alveolar canal compared with mandibular first molar.4 This variation makes endodontic treatment difficult and may lead to iatrogenic mishap if not studied before initiating treatment and it also increases successful outcome. Several populations have been studied to know and understand more about the root canal anatomy of mandibular first and second molars [4, 5].
Studies conducted in Mixed populations demonstrate Vertucci’s type IV (57.4%) in the mesial roots and type I (70.4%) in the distal roots of two-rooted second molars in Asian population [6]. The prevalence of C-shaped canal varies between 2.7 and 9.0 % in non-Asian populations, while it can reach 41.27 % in Asian populations such as Chinese, Koreans, and Hong Kong Chinese, indicating its racial diversity [7]. Similarly presence of radix is low and is associated with certain ethnic groups. This occurs at a frequency of 5%– 30% among mongoloids such as Chinese, Eskimos, and Native Americans, and <5% in white Caucasians, Africans, Eurasians, and Indians [8].
Carabelli was the first to discover the existence of an additional root in mandibular teeth in 1844 [9]. REs are often shorter and curved than most roots, and they can be fused to or separate from roots. Another frequently encountered problem in treating mandibular second molar is limited access to root canals orifices and additionally the presence of canal curvature of varying degrees complicates the treatment. Weine stated that managing a root canal with a curve of greater than 60 degrees is technically challenging [10]. Endodontic treatment of such a severe curvature necessitates skilled care to ensure thorough debridement and avoid complications such as ledge formation, foramen transportation, loss of working length, departure from the original canal course, root perforation, and instrument separation [11].
The positional relationship of the mandibular second molars to the mandibular canal and its relationship to the patient’s age is critical. Inferior Alveolar Nerve can be harmed by a variety of endodontic procedures. Several mechanisms have been proposed, (1) including a neuro-toxic effect from root canal filling material penetrating the IAN (2) mechanical pressure on the nerve caused by overextension of filling material or over instrumentation with hand or rotary files and (3) an increase in temperature proximal to the IAN greater than 10oC etc, can cause mechanical or chemical damage to the mandibular nerve [12].
CBCT is a 3-Dimensional, non-invasive imaging modality that provides detailed high-resolution images of oral structures as compared to 2-dimensional radiographs [13]. The use of CBCT allows the operator to see a region in the 3 separate planes (sagittal, coronal, and axial), which has shown to eliminate the superimposition of anatomic components [14]. The high-spatial-resolution along with lower radiation dose is the major advantage associated with CBCT [15].
As there is very little literature available on variations in root canal morphology of mandibular second molars and their relationship to the mandibular canal in the Central Gujarat population, the current CBCT study was designed to evaluate root canal configuration of mandibular second molars and their distance from the mandibular canal in the central Gujarat population.
Materials and Methods
This retrospective, cross-sectional study was conducted between November 2020 and May 2021 in Department of Conservative Dentistry and Endodontics, K M Shah Dental College, Vadodara, Gujarat, India in collaboration with CBCT centres in Central Gujarat region. 260 CBCT Scans were obtained from 5 different CBCT centres located in different cities of central Gujarat like Anand, Nadiad and Vadodara and, Ahmedabad. Prior permission from the institutional Ethics Committee was obtained (SVIEC/ON/Dent/SRP/20128).
Sample Size Calculation
The minimum sample size for CBCT was estimated to be 260 at 95% confidence interval using formula [DEFF x Np(1-p)]/ [(d2/Z21-α/2 x (N-1)+p x (1-p)] [16]. Population size (for finite population correction factor or fpc) (N): 5000 Hypothesized % frequency of outcome factor in the population (p): 9.2%±5 Confidence limits as % of 100(absolute ± %) (d): 5% Design effect (for cluster surveys-DEFF): 1
Inclusion and Exclusion Criteria
The study included CBCT scans of permanent mandibular second molars in the medium FOV (mandibular jaw) and large FOV of individuals aged 18 to 60 years residing in central Gujarat who did not have periapical lesions, periodontal ligament widening, prior endodontic treatment, or root resorption were included in the study. CBCT scans with artefacts obscuring the view of the mandibular canals or showing radio-opacity in mandibular second molar, as well as scans with a fractured mandibular jaw were excluded.
Evaluation of CBCT Scans
All scans were evaluated by the principal investigator and a co-investigator. At first, 30 CBCT scans were assigned to the principal and co-investigator, and then swapped. The remaining 230 scans were reviewed in the same way by both investigators. DICOM files of CBCT scans were evaluated in Sagittal, coronal and axial sections.
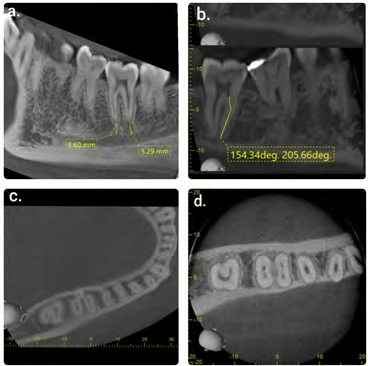
The CBCT scans were evaluated for the following in relation to mandibular second molar. a) Number of root canals in axial sections. b) The root canal system configuration was categorised into the first seven types of Vertucci classification 1984 in Sagittal & coronal sections [1]. c) Distance of root apex of mandibular second molars from the mandibular canal in Sagittal sections of CBCT. d) Degree of curvature present in any of the root canals in Sagittal or Coronal section of CBCT. e) Presence of any extra roots (radix) in mandibular second molars in Axial sections of CBCT. f) Axial and coronal slices of mandibular second molars with C-shaped canals (Fans classification) [17] (Figures 1a-d).
Assessment of Secondary Outcome
The CBCTs were evaluated into four age groups and distance from the root apex to the mandibular canal was calculated: group I (18-30) years of age; group II (31-40) years of age; group III (41-50) years of age; and group IV (51- 60) years of age. Subjects were also divided into two groups based on their gender. All measurements recorded from each root apex were categorised by age and gender for secondary outcome assessment.
Statistical Analysis
The data was then compiled and tallied. IBM SPSS Version 21.0 was used to analyse the data. The mean SD for continuous variables and the frequency % for categorical variables were used to express the data. Association between the variables (age, sex with distance of root apex from mandibular canal) was examined using the Chi- square test and a P-value of less than 0.05 was considered statistically significant.
Results
A total of 260 CBCT scans from the Central Gujarat population where 131 males (50.4%) and 129 females (49.6%) were included in this study. All the CBCT scans were evaluated by two calibrated (Kappa test 85 %) and trained investigators. The commonest root canal anatomy observed was the presence of 2 separate roots located mesiodistally with 3 root canals 192 (73.8%). Whereas, the occurrence of two and four root canals in two rooted mandibular second molars were 26 (10.0%) and 38 (14.6%) respectively. Vertucci’s classification was used to categorise the root canal configurations of these mandibular second molars’ mesial and distal root.
| Vertucci's classification | Percentage | |
|---|---|---|
| Mesial | I | 21 (8.1%) |
| Mesial | II | 150 (57.7%) |
| Mesial | III | 12 (4.6%) |
| Mesial | IV | 65 (25.0%) |
| Mesial | V | 5 (1.9%) |
| Distal | I | 175 (67.3%) |
| Distal | II | 66 (25.4%) |
| Distal | III | 9 (3.5%) |
| Distal | IV | 3 (1.2%) |
| Extra root | I | (100%) |
Table 1: Root canal configurations.
The most common pattern in the mesial roots of two- rooted molars was type II, followed by type IV whereas the occurrence of type I, type V, and type III were uncommon. The canals in the majority of the distal roots were type I, followed by type II, type III and type IV. In only 6(2.3%) of 260 CBCT scans of mandibular second molar Radix Entomolaris was present, and this root showed type I root canal morphology as shown in (Table 1).
The prevalence of C-shaped canal in lower second molar in central Gujarat was 7(5.4%) out of 260 CBCT scans. Cross- sectional canal configuration at coronal third according to Fan et al17 was observed C1 (3.1%), followed by C2 (2.3%). Mandibular second molar root canals persisted some degree of curvature with mean curvature was 21.88o ± 12.09o and range was between (0-45o). The distance from mandibular canal and the mesial and distal root apex of the mandibular second molars was measured in millimetres (mm).
Overall Average
When all of the measurements were aggregated, the distal root of the second molar was the closest to the mandibular canal, measuring 2.75 mm on average, whereas the mesial root measured 3.04 mm.
Association of distance of root apex from mandibular canal and Age: Amongst all the age groups, the distance between root apex and the mandibular canal was the largest for Group IV (>50 years) (mesial root 5.32 mm, distal root 4.66 mm), followed by Group III (41-50 years) (mesial root 3.04 mm, distal root 2.88 mm), Group II (31-40 years) (mesial root 3.1 mm , distal root 2.7 mm)and Group I (<=30 years) (mesial root 2.71 mm , distal root 2.44 mm) respectively and the average distance is represented in (Graph 1) Results of the association using Chi- square test indicated that as the age increases the distance from root apex to mandibular canal increases but statistically insignificant association between age and distance of mesial root(p= 0.538), distal root (p=0.889) from mandibular canal.
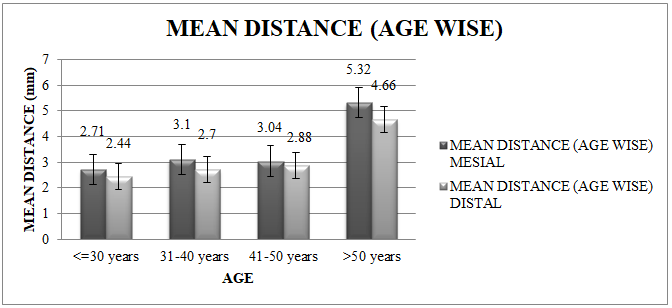
Graph 1: Age wise variation of mean distance of mesial and distal root apex from mandibular canal.
Association of Sex and distance between root apex and mandibular canal: The mean distance of mesial root and distal root for male was 3.33 and 3.05 mm respectively. While the mean distance of mesial root and distal root for female was 2.75 and 2.75 mm respectively. Results of the association using Chi- square test indicated that there was statistically insignificant association between males and females, when compared with distance of mesial (p=0.425) and distal root apex (p = 0.228) from mandibular canal. Thus, the distance from root apex to mandibular canal was more in males than in females shown in (Graph 2).
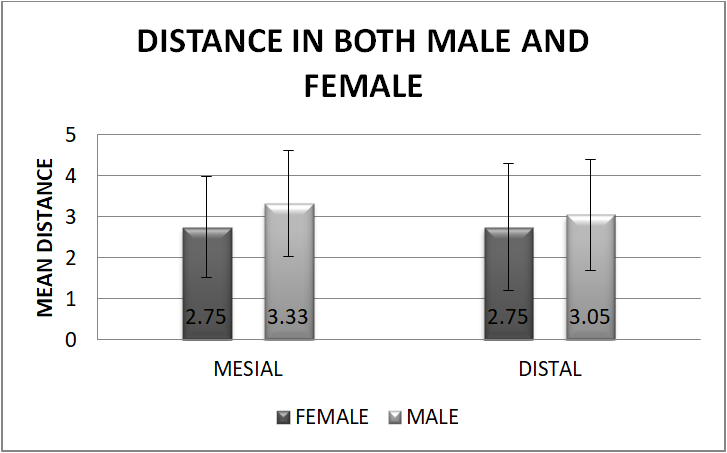
Graph 2: Gender variation of mean distance of mesial and distal root apex from mandibular canal.
Discussion
Mandibular second molars have always been associated with great variations in root patterns and canal morphology. This study examined the root canal anatomy of the mandibular second molars and their relation to the mandibular canal in the Central Gujarat population.
In mandibular second molars the frequently encountered root morphology was the presence of two separate roots (73.8%), which is similar to the findings of Maning, et al. (76%) [18] on Asian population and Neelakantan, et al. [4] (87.8%) on Indian population but was in contrast to study done by Gulabivala, et al. [5] on that of Burmese population was found to be 58.2% only. Mandibular second molars with three roots were seen in 4% of the teeth examined which was similar to study done by Kantilieraki, et al. [19] (4.9%) on Greek Population. The results were in contrast to study done by Gulabivala, et al. [5] on Burmese population in which no mandibular second molars with three roots were observed.
In two-rooted mandibular second molars, the most frequent root canal pattern observed was Vertucci’s type II (57.7%) in the mesial root. Which was similar to study done by Ingle, et al. [20] on American population mesial root (49%) showed type II. But it is contradictory to study done by Sadeghi, et al. [21] on Iranian population reported that the prevalence in mesial root (62% type IV, 26% type II). The difference in root canal configuration was because of geographical variation in the population. The distal roots predominantly exhibited Vertucci’s type I (67.3%) which was similar to systematic review done by Dae Pablo, et al. [22] were 22 studies were evaluate most common configuration was type I h (62.7%). It was also similar to study done by Neelakantan, et al. [4] on Indian population where type I canal configuration was (77.7%) in distal root.
The Vertucci´s configuration in radix was 100% type I in mesial and distal root canals in present study. The present study showed 2.3% of Radix, similar to Shemesh [23] investigation on Israeli population was (1.78%). Also similar to study by Gomez, et al. [24] (2.6%) on Venezuela population. On the other hand, a Korean population study by Kim, et al. [25] showed 0.72% of extra roots in mandibular second molars, and in a Spanish population study by Pérez, et al. [26] -radix variation was not found. Although studies on East Asian populations revealed a prevalence of 43.01% Radix, [27] in our ethnic group, the presence of radix in a mandibular second tooth is unusual. The presence of a supernumerary root can cause complications during endodontic therapy if not diagnosed early because it may not be visible 2D radiographs and may create the false impression of a root fracture [5].
The prevalence percentage of C-shaped canal morphology in our study was 14 % which was similar to the study done by Ashraf, et al. in [28] on Iranian population (13.8%). But our value was higher than study done by Singh RD, et al. on North Indian population (6.72%) [29]. This difference in prevalence rate could be because of methodology and diversity of the ethnicity of the population of the group studied. The most common canal configuration at the coronal level was C1 (3.1%), followed by C2 (2.3%) which was similar to the study done by Wadhwani S, et al. [30] in the Turkish population. However, in a study by Seo and Park [31] in the Korean population C2 type was more prevalent.
In contrast to the premolars and first molars, the mandibular second molar apices have been reported to be the closest to the mandibular canal [32]. Overall average distance of mandibular second molar mesial root apex to mandibular canal was 3.04 mm and distal root apex was 2.75 mm. The overall average distance was found to be greater than the distance found in the prior study by Sato, et al. [33] (0.48mm) on cadaver where panoramic radiographs were used. Because the study was conducted with CBCT, more accurate measurements could be taken since in a panoramic view, the x-ray tube’s negative angulations project the lingual mandibular canal higher. Similar results were seen in study done by Aljarbou, et al. [34] on Saudi population (mesial root 2.33±2.16, for distal root was 1.68±1.98). Another study by Lvovsky, et al. [35] on distance between root apex and Inferior alveolar canal in Israel (4.60 mm), South Korea (5.45 mm), and India (4.35 mm) showed there was significant difference between all the populations.
In our study, we found that females tend to exhibit shorter distances to the mandibular canal compared to males. Moreover, the present findings are also in agreement with another study by Simonton, et al. [36] on Texas population showing similar distances (6.2±2.6 mm for males and 4.9±2.2 mm for females) and overall shorter distances in women compared with men. This could be due to the fact that males typically have larger bodies, so the distance between the mandibular canal and the root apices could be longer in men. Clinically, this means that females are more likely to suffer iatrogenic nerve injury than males [36].
The distance between the mandibular canal and the root apices increased with age. The distances in the age group was largest for age >50 years. Which was similar to study done by Kovista, et al. [32] on American population. These findings indicate that the craniofacial complex changes throughout life like change in vertical distance from inferior alveolar nerve, width of bone and horizontal distance changes [36]. According to Stockdale [37], the distance increases as the teeth erupt. The apices of the teeth are not in close proximity to the mandibular canal when they come into occlusion.
Furthermore, the second molar remains nearer to the mandibular canal than the first molar during dental and skeletal development. A study conducted by Littner, et al. [38] on Israel populations found that the distal root of the mandibular second molar was closer to the mandibular canal than the first molar, which is similar to our findings.
There are various methods of measuring root canal curvature like Schneider’s method, [39] Lutein method, [40] but Weine’s method [41] is easier, reproducible, and efficient, particularly when using CBCT images for determination of root curvature radius. In present study 90% mandibular second molar had curvature in roots (mesial or distal). Our results were similar to study done by Gambarini, et al. [42] on European population were 85% molar have root curvature. Knowing the radius of the root curvature helps for more precise root canal instrumentation planning and reduces the impact of anatomic challenges.
The limitation of this study is the need to evaluate the CBCT of other ethnic groups as well. Also, Larger multi- centre studies are further required to generalized results. Hence, further studies need to be carried out with different geographical areas focusing on different combinations of digital imaging.
Clinical Significance
Root canal morphology can demonstrate variations based on race and sex of patients. By knowing the ethnic variations, clinician can treat those patient more efficiently. CBCT, being 3 dimensional high‑resolution isotropic imaging system is a very useful tool in knowing the internal anatomy of the tooth and calculating exact distance of mandibular canal which is not possible in conventional radiograph. For Dental Practitioner, common information of anatomical variations in number of root canals, presence or absence of extra root, C shaped canal, curvatures and distance of tooth from mandibular canal in male and female patients plays very important role in successful endodontic treatment. This aids in improved accuracy and outcome of the treatment.
Conclusion
Within the limitations of the study, we can conclude that Mesial root of mandibular second molar shows Vertucci’s type II canal configuration while distal root presented with type I. C shaped canal configuration with fused roots was seen in 5.4% of patient in Central Gujarat population. Whereas Radix Entomolaris was present in only 2.3% of population. The distal root shows more proximity to mandibular canal than mesial roots and the mean distance of root apex from mandibular canal was less in females compared to males. Additionally, as the age advances the distance of root apex from mandibular canal increases.
- Acknowledgements: The work was supported by the Departmental library, CBCT scans from Dentscan Imaging Centre (Vadodara, Anand) and Oroscan (Anand, Vadodara & Ahmadabad centre)
- Patients consent: For this type of study, formal consent is not required
References
-
Vertucci F (1974) Root canal anatomy of the mandibular anterior teeth. J Am Dent Assoc 89(2): 369-371.
-
Petju M, Suteerayongprasert A, Thongpud R, Hassiri K (2007) Importance of dental records for victim identification following the Indian Ocean tsunami. Public Health 121(4): 251-257.
-
Schuller Götzburg P, Suchanek J (2007) Forensic odontologists successfully identify tsunami victims in Phuket, Thailand. Forensic Sci Int 171(2-3): 204-207.
-
Neelakantan P, Subbarao C, Subbarao CV, Ravindranath M (2010) Root and canal morphology of mandibular second molars in an Indian population. J Endod 36(8): 1319-1322.
-
Gulabivala K, Aung TH, Alavi A (2001) Root and canal morphology of Burmese mandibular molars. Int Endod J 34(5): 359-370.
-
Gulabivala K, Opasanon A, Ng Y, Alavi A (2002) Root and canal morphology of Thai mandibular molars. Int Endod J 35(1): 56-62.
-
Jin GC, Lee SJ, Roh BD (2006) Anatomical study of C-shaped canals in mandibular second molars by analysis of computed tomography. J Endod 32(1): 10-13.
-
Attam K, Nawal R, Utneja S, Talwar S (2012) Radix Entomolaris in Mandibular First Molars in Indian Population-A Review and Case Reports. Case Rep Dent 2012: 595494.
-
Carabelli G (1844) Systematisches Handbuch der Zahnheilkunde. 2nd (Edn.), Vienna: Braumuller und Seidel, pp: 114.
-
Weine FS (1996) Endodontic Therapy, 5th (Edn.), St. Louis. Mosby-Year Book, Inc, pp:305-394.
-
Cunningham CJ, Senia ES (1992) A three dimensional study of canal curvatures in the mesial roots of mandibular molars. J Endod 18(6): 294-300.
-
Pogrel MA (2007) Damage to the inferior alveolar nerve as the result of root canal therapy. J Am Dent Assoc 138(1): 65-69.
-
Ferrari CH, Abu Hasna A, Martinho FC (2021) Three dimensional mapping of the root apex: distances between apexes and anatomical structures and external cortical plates. Brazilian Oral Research 35: e022.
-
Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG (2007) Endodontic applications of cone-beam volumetric tomography. J Endod 33(9): 1121-1132.
-
Patel S (2009) New dimensions in endodontic imaging: part 2. Cone beam computed tomography. Int Endod J 42(6): 463-475.
-
Jaju S, Jaju PP, Garcha V (2013) Root canal assessment of mandibular incisors in an Indian population using cone beam CT. ENDO - Endodontic Practice Today 7(2): 1-2.
-
Fan B, Cheung GS, Fan M, Gutmann JL, Fan W (2004) C-shaped canal system in mandibular second molars: Part II--Radiographic features. J Endod 30(12): 904-908.
-
Manning SA (1990) Root canal anatomy of mandibular second molars, Part I. Int Endod J 23(1): 34-39.
-
Kantilieraki E, Delantoni A, Angelopoulos C, Beltes P (2019) Evaluation of Root and Root Canal Morphology of Mandibular First and Second Molars in a Greek Population: A CBCT Study. Eur Endod J 4(2): 62-68.
-
Ingle JI (2008) Endodontics. 5th (Edn.), Hamilton London: Bc Decker Inc, pp: 845-858.
-
Sadeghi M, Sadr Lahijani M (2004) An _invitro_ Study of Root Canal Anatomy in Mandibular Molars. J Dent Sch 22(1): 96-103.
-
De Pablo OV, Estevez R, Péix Sánchez M, Heilborn C, Cohenca N (2010) Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod 36(12): 1919-1931.
-
Shemesh A, Levin A, Katzenell V, Itzhak J, Levinson O, et al. (2015) Prevalence of 3 and 4-rooted first and second mandibular molars in the Israeli population. J Endod 41(3): 338-342.
-
Gomez F, Brea G and Francisco J (2021) Root canal morphology and variations in mandibular second molars: an in vivo cone-beam computed tomography analysis. BMC Oral Health 21(1): 424.
-
Kim SY, Kim BS, Kim Y (2016) Mandibular second molar root canal morphology and variants in a Korean subpopulation. Int Endod J 49(2): 136-144.
-
Perez Heredia M, Ferrer Luque C, Bravo M, Castelo Baz P, Ruiz Piñon M, et al. (2017) Cone-beam Computed Tomographic Study of Root Anatomy and Canal Confguration of Molars in a Spanish Population. J Endod 43(9): 1511-1516.
-
Zhang R, Wang H, Tian YY, Yu X, Hu T, et al. (2011) Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J 44(11): 990-999.
-
Ashraf H, Grayeli M (2013) Determine Frequency and Anatomic form of the C-Shaped Canals in Mandibular Second Molars. J Dent Sch 21(4): 441-446.
-
Singh RD, Bal CS, Khatter R, Rajesh Khanna R, Walia S (2015) Incidence and configuration of C-shaped root canals in north Indian population. Indian Journal of Comprehensive Dental Care 5(1): 528-532.
-
Wadhwani S, Singh MP, Agarwal M, Somasundaram P, Rawtiya M, et al. (2017) Prevalence of C-shaped canals in mandibular second and third molars in a central India population: A cone beam computed tomography analysis. J Conserv Dent 20(5): 351-354.
-
Seo MS, Park DS (2004) C-shaped root canals of mandibular second molars in a Korean population: clinical observation and in vitro analysis. Int Endod J 37(2): 139-144.
-
Kovisto T, Ahmad M, Bowles W (2011) Proximity of the Mandibular Canal to the Tooth Apex. J Endod 37(3): 311- 315.
-
Sato I, Ueno R, Kawai T, Yosue T (2005) Rare courses of the mandibular canal in the molar regions of the human mandible: a cadaveric study. Okajimas Folia Anat Jpn 82(3): 95-101.
-
Aljarbou F, Aldosimani M, Althumairy R, Alhezam A, Aldawsari A (2019) An analysis of the first and second mandibular molar roots proximity to the inferior alveolar canal and cortical plates using cone beam computed tomography among the Saudi population. Saudi Medical Journal 40(2): 189-194.
-
Lvovsky A, Bachrach S, Kim H, Pawar A, Levinzon O, et al. (2018) Relationship between Root Apices and the Mandibular Canal: A Cone-beam Computed Tomographic Comparison of 3 Populations. J Endod 44(4): 555-558.
-
Simonton JD, Azevedo B, Schindler WG, Hargreaves KM (2009) Age- and gender-related differences in the position of the inferior alveolar nerve by using cone beam computed tomography. J Endod 35(7): 944-949.
-
Stockdale CR (1959) The relationship of the roots of mandibular third molars to the inferior dental canal. Oral surg Oral Med Oral Pathol 12: 1061-1072.
-
Littner MM, Kaffe I, Tamse A, Dicapua P (1986) Relationship between the apices of the lower molars and mandibular canal-a radiographic study. Oral Surg Oral Med Oral Pathol 62(5): 595-602.
-
Schneider SW (1971) A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 32(2): 271-275.
-
Luiten DJ, Morgan LA, Baugartner JC, Marshall JG (1995) A comparison of four instrumentation techniques on apical canal transportation. J Endod 21(1): 26-32.
-
Weine F (1982) Endodontic Therapy. 3rd (Edn.), St. Louis: CV Mosby, pp: 256-340.
-
Gambarini G, Piasecki L, Ropini P, Miccoli G, Nardo DD, et al. (2018) Cone-beam computed tomographic analysis on root and canal morphology of mandibular first permanent molar among multiracial population in Western European population. Eur J Dent 12(3): 434- 438.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells