Syndrome Associated with Cervical Vertebrae Anomalies and Orthodontic Relevance
Cervical vertebrae anomalies (such as Dehiscence, fusion of cervical spine, occipitalization) are associated with myelopathy, cause limitation in neck movement, muscular atrophy, and regional sensory loss. These cervical vertebrae anomalies are associated with syndromes such as Klippel-Feil syndrome, Goldenhar syndrome, Pfeiffer syndrome, Crouzon syndrome, Apert syndrome, Larsen syndrome and 22q11.2 micro deletion syndromes. Cervical vertebrae anomalies can be visualized in lateral cephalogram which is routinely advised for orthodontic patients to assess maxillary and mandibular relationship. Assessment of CVA in lateral cephalogram at an early age is essential, not only for treatment of the malformation but because there may be an association with other spinal and non-spinal diseases related to development. Present review discusses about various syndromes and clinical manifestations associated with cervical vertebrae anomalies and its relevance in orthodontics.
Introduction
Cervical vertebrae anomalies such as Dehiscence, fusion of upper cervical spine, occipitalization and combination of any of the above can cause compression of vertebral artery which reduces blood flow to the brain and compression of the nerves may lead to neurological disorders. Cervical vertebral anomalies can present with myelopathy, cause limitation in neck movement, muscular atrophy, and regional sensory loss [1]. Early diagnosis of cervical vertebrae anomalies (CVA) is critical in determining the risk of associated diseases at the time of presentation in young patients and the occurrence of secondary neurological symptoms later in life.
Embryological Basis of CVA
CVA develops during early intrauterine life due to a combination of the genetic and environmental factors. Malformation of the notochord, the poor performance of retinoids, decreased local blood supply to the spine and an alteration in gene expression, especially the members of Hox and Pax family genes, are some of the proposed reasons for interrupted development and fusion of the cervical vertebrae [2]. Cervical vertebrae development and the approximation of the developing palatine shelves arising from the maxillary process of either side occur during early intrauterine life with a closure of the shelves occurring around 8-9 weeks. The CVA and the development of the cleft seem to be interrelated. A short neck with vertebral synostosis or other changes limiting head extension of the foetus interfere with the anterior and descending development of the glosso-mandibular complex. Consequently, there may be inadequate space above the tongue, which is required to allow horizontal approximation of the palatal shelves towards the midline, the failure of which may result in incomplete closure of the palate [3].
Fusion of the cervical vertebrae is also prevalent in conditions, such as Klippel-Feil syndrome [1], Goldenhar syndrome [4], Pfeiffer syndrome [5], Crouzon syndrome [6] and Apert syndrome [7], Larsen syndrome [8] and 22q11.2 micro deletion syndromes [9]. Fusion of the cervical vertebrae can be a cause for precordialgia, a condition of cervicogenic angina due to the union of the C3-C4 vertebrae [10].
Types of Cervical Vertebrae Anomaly
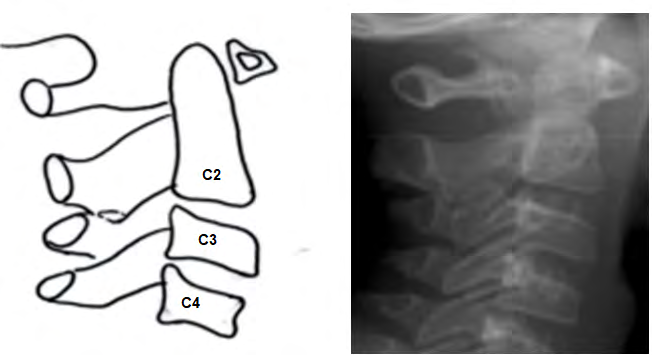
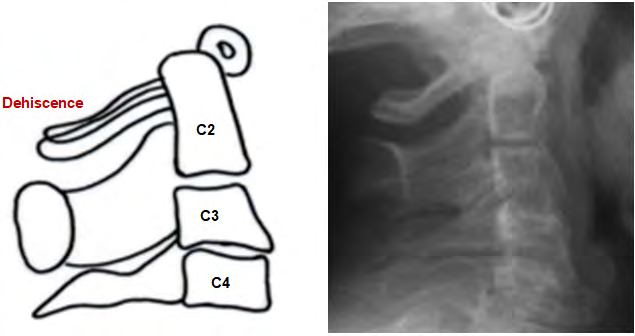
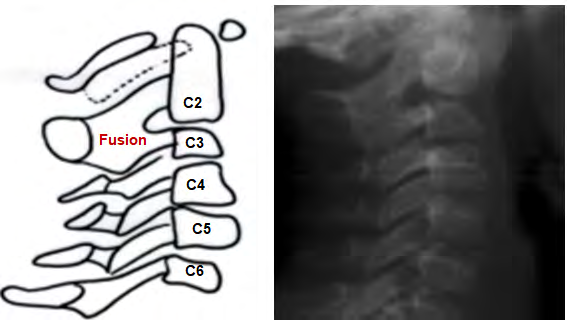
CVA are broadly divided into posterior arch deficiencies (PAD) and fusions [11, 12]. PAD are subdivided into dehiscence and spina bifida. Dehiscence implies incomplete development of the structures. Dehiscence is common in the midline and posterior arch, but in rare cases it can occur in the anterior arch also. Spina bifida refers to incomplete ossification of the spinous process and generally occurs in the posterior arch of the vertebral unit. Fusion is bony union of one unit with another at the articulation facets, neural arch, or transverse processes. Fusion can occur between two vertebrae or multiple vertebrae (block fusion). Occipitalization is atlantooccipital fusion which refers to the assimilation of the atlas to the base of the skull [13, 14] Figures 1-3.
Syndromes Associated with CVAs
Klippel-Feil syndrome: Klippel-Feil syndrome (KFS) is characterised by the presence of congenital synostosis of some or all cervical vertebrae. This congenital vertebral fusion results from the faulty segmentation along the embryonal axis during the first 3 to 8 weeks of gestation. The diagnostic clinical triad consists of short neck, low posterior hairline, and limited neck movements. Fewer than 50% of the patients show this clinical triad. Feil described three morphological subtypes of this anomaly. Type I comprises of a single congenitally fused cervical segment; Type II includes multiple non-contiguous congenitally fused segments, and Type III is characterised by multiple contiguous, congenitally fused cervical segments [15].
Based on the position of cervical vertebra fusion, the status of familial trait and its characteristics; 4 classes (KF 1, 2, 3, and 4) were identified [16]. KF1 is characterised by C1 fusion and marked autosomal recessive trait; KF2 is marked by a fusion of C2-3 and an autosomal dominant trait. KF3 is characterised by fusion of C3, and the trait is autosomal recessive type. In KF4, an X-linked trait and eye anomalies along with cervical fusion is present [16]. Despite the heterogeneous presentation it has been reported that the fusion of C5-C6 and C2-C3 is most common [17]. Goldenhar Syndrome: Goldenhar syndrome is a congenital disorder of the first and second branchial arches. Clinical manifestations include craniofacial microsomia, ocular dermoid cysts, vertebral anomalies, and cardiac and renal defects [18]. Various types of cervical spine fusion have been reported in 8% to 61% of cases. Occipitalization of the atlas ranges from 4.4% to 30% in various studies [19]. Pfeiffer syndrome: Pfeiffer syndrome is characterised by craniosynostosis, broad thumbs and great toes and, soft tissue syndactyly of the hands and feet. Cohen (1993) has sub-grouped Pfeiffer syndrome into three types; type 1 is the classic Pfeiffer syndrome associated with satisfactory prognosis, type 2 and type 3 is subgrouped according to the presence or absence of cloverleaf skull and has a poor outcome [20]. It is characterised by the presence of cervical spine fusions which is progressive. Upper and middle cervical spine fusions are more common [5]. Crouzon syndrome: Crouzon syndrome is an autosomal dominant disorder caused by premature closure of coronal and sagittal sutures. Crouzon syndrome is characterised by proptosis and divergent strabismus, ocular hypertelorism and maxillary hypoplasia. It is caused by the mutation of FGFR2, a gene critical to the transformation of fibrous joint lines between sutures to osseous bone matrix [21]. Cervical region radiologic abnormalities associated with this syndrome include butterfly-shaped vertebra and fusion of the posterior bodies and elements. Fusion of C2-C3 and C5- C6 have been found to be equally affected [22]. Apert syndrome: Apert syndrome is characterized by the presence of craniosynostosis, midface retrusion, and syndactyly of the hands. All affected individuals have coronal craniosynostosis, and a majority may also have an involvement of the sagittal and lambdoidal sutures. A subset of affected individuals have cleft palate. The hands in Apert syndrome always includes fusion of the middle three digits; the thumb and fifth finger are also sometimes involved. Cervical fusion of C5-C6 fusion is the most common, alone or in combination with other fusions [7]. Larsen Syndrome: Larsen syndrome is a genetic disorder of autosomal dominant or autosomal recessive type inheritance. The clinical presentation is characterised by multiple joint dislocations (elbows, hips, and knees), flat forehead, depressed nasal bridge, flat midface, hypertelorism, and club foot, heart defects, cleft palate, and neonatal tracheomalacia [8]. This is syndrome is characterised by cervical kyphosis instability which can progress with time [23]. 22q11.2 Deletion Syndrome: The 22q11.2 microdeletion has been seen in patients with velocardiofacial syndrome, DiGeorge syndrome, conotruncal face anomaly syndrome, CHARGE syndrome, and many others. Systemic issues prevalent in this syndrome include conotruncal heart defects, tetralogy of fallot, typical facies, cognitive delays, and anxiety [9]. Cervical spine anomalies associated with this syndrome includes platybasia (91%), open C1 posterior arch (59%), dysmorphic dens (58%), and C2 to C3 fusions (34%) [19].
CVA in Orthodontic Patients
Of the different types of malocclusions (Angle Class I, Class II and Class III), no significant difference in the distribution of CVA has been observed and with no gender dimorphism [24]. Farman, et al. [25] evaluated lateral cephalograms of 220 normal adolescent orthodontic patients and patients with craniofacial dysostosis and oculodento-osseous dysplasia. Variation was observed in the morphology of the upper cervical vertebrae which exhibited posterior arch dehiscence in eight individuals. Three patients had accessory ossicles above the posterior arch of the atlas, and two showed evidence of fusion of the second and third cervical vertebrae.
Yoshihara, et al. [1] incidentally encountered an anomaly of the cervical vertebrae during an orthodontic examination of an eight year old boy who presented with a cleft lip and palate. The patient was diagnosed with Klippel-Feil syndrome by an orthopaedic specialist to whom referral was made for a detailed examination. Mild cases of CVA may not present with significant clinical symptoms but may develop neurological symptoms secondary to degenerative disc diseases of the adjacent mobile segments, spinal instability from hypermobility or resulting after trauma, or spinal stenosis in the later decades of life. Fusion of the first and second cervical vertebra (C1 and C2) tends to produce symptoms in the first decade of life, while the fusion of the second and third cervical vertebra (C2 and C3) exhibit neurological symptoms in the third decade. Most symptoms, regardless of the location of the lesion, appears before 30 years of age.
Meibodi, et al. [26] showed that 73.3% of Class III patients exhibited fusion of cervical vertebrae compared to 32.6% of Class I patients. Sun and Lee [27] found that males and females with cleft lip and palate had lower skeletal maturity than their unaffected peers and a delayed pubertal growth peak. Patients with CVA are at a higher risk of developing obstructive sleep apnoea [28]. CVA may narrow the spinal canal so that hyperextension of the neck during endotracheal intubation or while positioning the patient head for palatoplasty may injure the spinal cord. Pharyngeal flap surgery may not be advisable in adult patients with cleft palate [29]. A lateral cephalogram offers an excellent diagnostic tool to rule out CVA.
Lateral cephalogram is routinely advised for orthodontic patients. CVA can be assessed on the lateral cephalogram. Patient and parents can be informed about the syndromes associated with CVA and clinical manifestations of syndrome which may not be present during early decades of life but can occur or worsen in 2nd and 3rd decades of life. Early counselling and appropriate management will help the patient to reduce or prevent clinical manifestation later in life.
Prevalence of CVA in Patients with Cleft Lip and Palate
CVA within cleft and non-cleft groups show considerable global variation. The prevalence of CVA in cleft group varied from 13% to 39% while it varied from 0.8% to 31% in non- cleft cases [29]. A study by Kharbanda, et al. reported that the prevalence of CVA was 37.7% (95% CI: 29.8% – 46.1%) in the cleft group and 20.7% (95% CI: 14.5% – 28.0%) [30] in the non-cleft group. Fusion of cervical vertebrae as the most common anomaly within the cleft/non-cleft groups irrespective of cleft type.
Clinical Relevance of CVA
The association between two or more anomalies linked to a common embryologic factor is frequently reported in studies related to craniofacial dysmorphia. Based on this observation, a relationship between the CLP and CVA was hypothesised. Ross and Lindsay [3] studied the association and questioned inappropriate cervical development in CLP aetiology. Developmental abnormalities of the cervical spine vary widely, are often sporadic, and may be isolated or a part of a multi-organ-systemic syndrome anomaly. Many anomalies are asymptomatic and go undetected, but several types may result in biomechanical instability or compress neurologic structures, thus placing the patient at risk of neurologic injury or chronic pain from the deformity [2]. Identifying the lesions with significant clinical implications at an early age is essential, not only for treatment of the malformation but because there may be an association with other spinal and non-spinal diseases related to development.
Orthodontic implication of CVA
Lateral cephalograms are routinely advised for the patients in orthodontic and cleft and craniofacial clinic for diagnosis and treatment planning. During the clinical visit of the patient CVAs can be diagnosed by the orthodontist in the lateral cephalogram. In case of presence of CVAs patient can be referred for genetic evaluation to assess the presence of syndromes. Even so, a high proportion of cleft and non- cleft cases were observed which showed CVAs. If a more sensitive imaging technique such as CBCT and MDCT are used, the prevalence may well be different [31]. However, such techniques are associated with exposure to radiation and come with specific indications. The finding of a CVA in a lateral cephalogram should be interpreted with caution and identified. Cases appropriately referred to the neurologists/ orthopaedic specialist or for counselling and alternative management.
The long-term sequelae of a cleft associated CVA are a subject requiring further investigation. The orthodontic management of patients with clefts and CVA does not differ from that of other patients. A diagnosis of CVA allows a better understanding of the cleft development process. Early diagnosis of fusion is critical in determining the risk of other associated diseases at presentation and secondary neurological symptoms in the future. CVA, which may have remained obscure, can be revealed incidentally via radiological examinations performed for orthodontic reasons.
Limitations and Future perspectives
The advancement of technology using 3D reconstruction from cone beam computed tomography images with reduced radiation will enable a more accurate assessment of the cervical spine area.
Conclusion
Identified orthodontic cleft and noncleft patients with cervical vertebrae anomalies need a timely referral to appropriate specialist for counselling and management to prevent spinal and non-spinal diseases related to development later in life.
References
-
Yoshihara T, Suzuki J, Yawaka Y (2010) Anomaly of cervical vertebrae found on orthodontic examination: 8-year-old boy with cleft lip and palate diagnosed with Klippel-Feil syndrome. Angle Orthod 80(5): 975-980.
-
Mardani M, Borujeni S, Javad M, Esfandiary E (2016) Congenital fusion of cervical vertebrae: a review on embryological etiology. Rev Clin Med 3(4): 148-153.
-
Ross RB, Lindsay WK (1965) The cervical vertebrae as a factor in etiology of cleft palate. Cleft palate 36: 273-281.
-
Al Kaissi A, Ben Chehida F, Ganger R, Klaushofer K, Grill F (2015) Distinctive spine abnormalities in patients with Goldenhar syndrome: tomographic assessment. Eur Spine J 24(3): 594-599.
-
Moore MH, Lodge ML, Clark BE (1995) Spinal anomalies in Pfeiffer syndrome. Cleft Palate-Craniofacial J 32(3): 251-254.
-
Hemmer KM, McAlister WH, Marsh JL (1987) Cervical spine anomalies in the craniosynostosis syndromes. Cleft Palate J 24(4): 328-333.
-
Kreiborg S, Barr M, Cohen MM (1992) Cervical spine in the Apert syndrome. Am J Med Genet 43(4): 704-708.
-
Larsen LJ, Schottstaedt ER, Bost FC (1950) Multiple congenital dislocations associated with characteristics facial abnormality. J Pediatr 37(4): 574-581.
-
Dormans JP, Drummond DS, Sutton LN, Ecker ML, Kopacz KJ (1995) Occipitocervical arthrodesis in children: a new technique and analysis of results. J Bone Joint Surg Am 77(8): 1234-1240.
-
Chatterjee D (2014) An unusual cause of chest pain: Fused cervical vertebra (C3-C4). Indian Journal of Pain 28(1): 44-46.
-
Osborne GS (1968) The prevalence of anomalies of the upper cervical vertebrae in patients with craniofacial malformations and their effect on osseous nasopharyngeal depth. Carbondale: Southern Illinois University, Dissertation.
-
Sandham A (1986) Cervical vertebral anomalies in cleft lip and palate. Cleft Palate J 23(3): 206-214.
-
Uğar DA, Semb G (2001) The prevalence of anomalies of the upper cervical vertebrae in subjects with cleft lip, cleft palate, or both. Cleft Palate-Craniofacial J 38(5): 498-503.
-
Klimo P, Rao G, Brockmeyer D (2007) Congenital anomalies of the cervical spine. Neurosurg Clin N Am 18(3): 463-478.
-
Samartzis DD, Herman J, Lubicky JP, Shen FH (2006) Classification of congenitally fused cervical patterns in Klippel-Feil patients: epidemiology and role in the development of cervical spine-related symptoms. Spine (Phila Pa 1976) 31(21): 798-804.
-
Clarke RA, Catalan G, Diwan AD, Kearsley JH (2008) Heterogeneity in Klippel Feil syndrome: a new classification. Pediatr Radiol 28(12): 967-974.
-
Gruber J, Saleh A, Bakhsh W, Rubery PT, Mesfin A (2018) The prevalence of Klippel-Feil syndrome: a computed tomography-based analysis of 2,917 patients. Spine Deform 6(4): 448-453.
-
Feingold M, Baum J (1978) Goldenhar’s syndrome. Am J Dis Child 132(2): 136-138.
-
McKay SD, Al Omari A, Tomlinson LA, Dormans JP (2012). Review of Cervical Spine Anomalies in Genetic Syndromes. Spine 37(5): 269-277.
-
Cohen MM (1993) Pfeiffer syndrome update, clinical subtypes and guidelines for differential diagnosis. Am J Med Genet 45(3): 300-307.
-
Helman SN, Badhey A, Kadakia S, Myers E (2014) Revisiting Crouzon syndrome: reviewing the background and management of a multifaceted disease. Oral Maxillofac Surg 18(4): 373-379.
-
Bowling EL, Burstein FD (2006) Crouzon syndrome. Optometry 77(5): 217-222.
-
Campbell RM Jr. (2009) Spine deformities in rare congenital syndromes: clinical issues. Spine 34(17): 1815-1827.
-
Kamak H, Yildirim E (2015) The distribution of cervical vertebrae anomalies among dental malocclusions. J Craniovertebr Junction Spine 6(4):158-161.
-
Farman AG, Nortjé CJ, Joubert JJ (1979) Radiographic profile of the first cervical vertebra. J Anat 128(Pt 3): 595-600.
-
Meibodi SE, Parhiz H, Motamedi MHK, Fetrati A, Meibodi EM, et al. (2011) Cervical vertebrae anomalies in patients with class III skeletal malocclusion. J Craniovertebr Junction Spine 2(2): 73-76.
-
Sun L, Li WR (2012) Cervical vertebral maturation of children with orofacial clefts. Cleft Palate-Craniofac J 49(6): 683-688.
-
Ray S, Datana S, Jayan B, Jain A (2015) Cervical vertebral anomalies in patients with obstructive sleep apnea. APOS Trends Orthod 5(6): 262-266.
-
Kharbanda OP, Qureshi T, Kandasamy T (2019) Prevalence of cervical vertebrae anomalies in patients with cleft lip and palate. Australasian Orthodontic Journal 35(1): 46-52.
-
Zook EG, Salmon JH (1977) Anomalies of the cervical spine in the cleft palate patient. Plast Reconstr Surg 60(1): 96-99.
-
Patcas R, Tausch D, Pandis N, Manestar M, Ullrich O, et al. (2013) Illusions of fusions: assessing cervical vertebral fusion on lateral cephalograms, multidetector computed tomographs, and cone-beam computed tomographs. Am J Orthod Dentofacial Orthop 143(2): 213-220.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells