Non-Syndromic Generalized Radiculomegaly: A Brief Pediatric Case Series
Background: Radiculomegaly is an idiopathic root malformation characterized by abnormally long tooth roots and, consequently, an increased root-crown ratio of teeth. Although radiculomegaly is rare, non-syndromic radiculomegaly is highly rare. There are no reports of non-syndromic, generalized radiculomegaly affecting both primary and permanent dentition in pediatric patients. Description: This case series presents two unique pediatric cases of non-syndromic, generalized radiculomegaly affecting both primary and permanent dentition. Panoramic radiographs during mixed and permanent dentition were used to calculate root-crown ratios of all teeth to diagnose radiculomegaly. Concurrently, both cases also presented with hypodontia and gemination. These concurrent findings may point to an association of radiculomegaly with other specific tooth anomalies. This case series discusses diagnosis, management, and anticipatory guidance for individuals with radiculomegaly. Conclusion: Panoramic radiographs are vital for efficient diagnosis of radiculomegaly as such a diagnosis will impact future endodontic, orthodontic, and surgical management.
Introduction
Radiculomegaly (RM) is an idiopathic root malformation characterized by excessively long tooth roots and, consequently, an increased root-crown ratio of teeth [1]. RM has been reported as localized or generalized depending on the number of teeth involved [1, 2]. The syndromes commonly associated with RM are oculofaciocardiodental syndrome, Klinefelter syndrome, and Cockayne syndrome [1]. Although syndromic RM is rare, non-syndromic RM is highly rare [1]. Furthermore, non-syndromic RM affecting both primary and permanent dentition is exceptionally rare [3]. There are no pediatric cases reporting generalized RM affecting both the primary and permanent dentition. This case series provides details of two pediatric cases of generalized, non-syndromic RM affecting both the primary and permanent dentition followed at Children’s Hospital Colorado for routine dental care and annual intra-oral radiographs between ages 5-17. The Institutional Review Board approved the study (#PAM002). Root-crown (RC) ratio was calculated for each tooth using panoramic radiographs based on Lind’s method [4]. Briefly, a midpoint of a line drawn connecting the mesiodistal cementoenamel junctions of the tooth on a radiograph was noted. A linear distance between this midpoint and the apex of the root was considered as the root length. Similarly, a linear distance between the midpoint and the most coronal point of the crown was considered as the crown length. The ratio of root-crown lengths was used to calculate root-crown (RC) ratio from three measurements for each tooth; mean RC scores for all teeth in each case are presented in Table 1. The schematic for calculation of RC ratio is given in Figure 1C.
| Case 1 | Case 2 | |
|---|---|---|
| Tooth # | RC ratio | RC ratio |
| Primary dentition | ||
| #A | 2.31 | 2.03 |
| #B | 1.61 | 1.83 |
| #C | 2.61 | 2.37 |
| #H | 2.64 | 2.40 |
| #I | 1.73 | 1.83 |
| #J | 2.36 | 2.06 |
| #K | 3.00 | 2.57 |
| #L | 2.09 | 2.11 |
| #M | 2.59 | 2.56 |
| #R | 2.60 | 2.73 |
| #S | 2.00 | 2.04 |
| #T | 3.04 | 2.67 |
| Permanent dentition | ||
| #1 | Unerupted | Unerupted |
| #2 | 3.03 | 2.83 |
| #3 | 3.37 | 3.18 |
| #4 | 2.73 | 2.81 |
| #5 | 2.70 | 2.97 |
| #6 | 3.14 | 2.72 |
| #7 | 2.71 | 2.38 |
| #8 | 2.59 | 2.08 |
| #9 | 2.56 | 2.08 |
| #10 | 2.46 | 2.41 |
| #11 | 3.08 | 2.76 |
| #12 | 2.77 | 2.95 |
| #13 | 2.86 | 2.81 |
| #14 | 3.02 | 3.19 |
| #15 | 3.00 | 2.79 |
| #16 | Unerupted | Unerupted |
| #17 | Gemination | Unerupted |
| #18 | Missing | 2.79 |
| #19 | 3.20 | 3.02 |
| #20 | 3.47 | 2.61 |
| #21 | 3.00 | 2.67 |
| #22 | 3.13 | 2.76 |
| #23 | 2.58 | 2.28 |
| #24 | 2.62 | 2.46 |
| #25 | 2.62 | 2.48 |
| #26 | 2.83 | 2.30 |
| #27 | 3.11 | 2.41 |
| #28 | 3.63 | 2.76 |
| #29 | 3.48 | Missing |
| #30 | 3.27 | 3.00 |
| #31 | Missing | Gemination |
| #32 | Missing | Missing |
Table 1: The schematic for calculation of RC ratio is given in Figure 1C.
Case Series
Case 1 was a seventeen-year-old Caucasian female with height and weight as 171.6 cm and 58.5 kg, respectively. She had noncontributory medical and family history. Her dental history was significant for multiple restorations and extractions of over-retained primary teeth. Her extraoral facial profile was straight with dolicocephalic head and leptoprosopic facial forms. Intraoral exam revealed gemination of #17, congenital absence of #s 18, 31, and 32 with pulp stones in all first permanent molars. Panoramic radiographs were taken during mixed (age 8, Figure 1A) and permanent (age 16, Figure 1B) dentition stages.
Case 2 was a sixteen-year-old African American female patient with height and weight as 160.2 cm and 58.8 kg, respectively. She had no significant medical or family history and dental history included a few restorations in primary teeth. Her extraoral exam revealed convex facial profile with mesocephalic head and mesoprosopic facial form. Intraoral exam revealed mild molar-incisor hypomineralization, pulp stones in permanent first molars, gemination of #32, and congenital absence of #s 29 and 31. Panoramic radiographs were taken at ages 8 (Figure 2A) and 16 (Figure 2B).
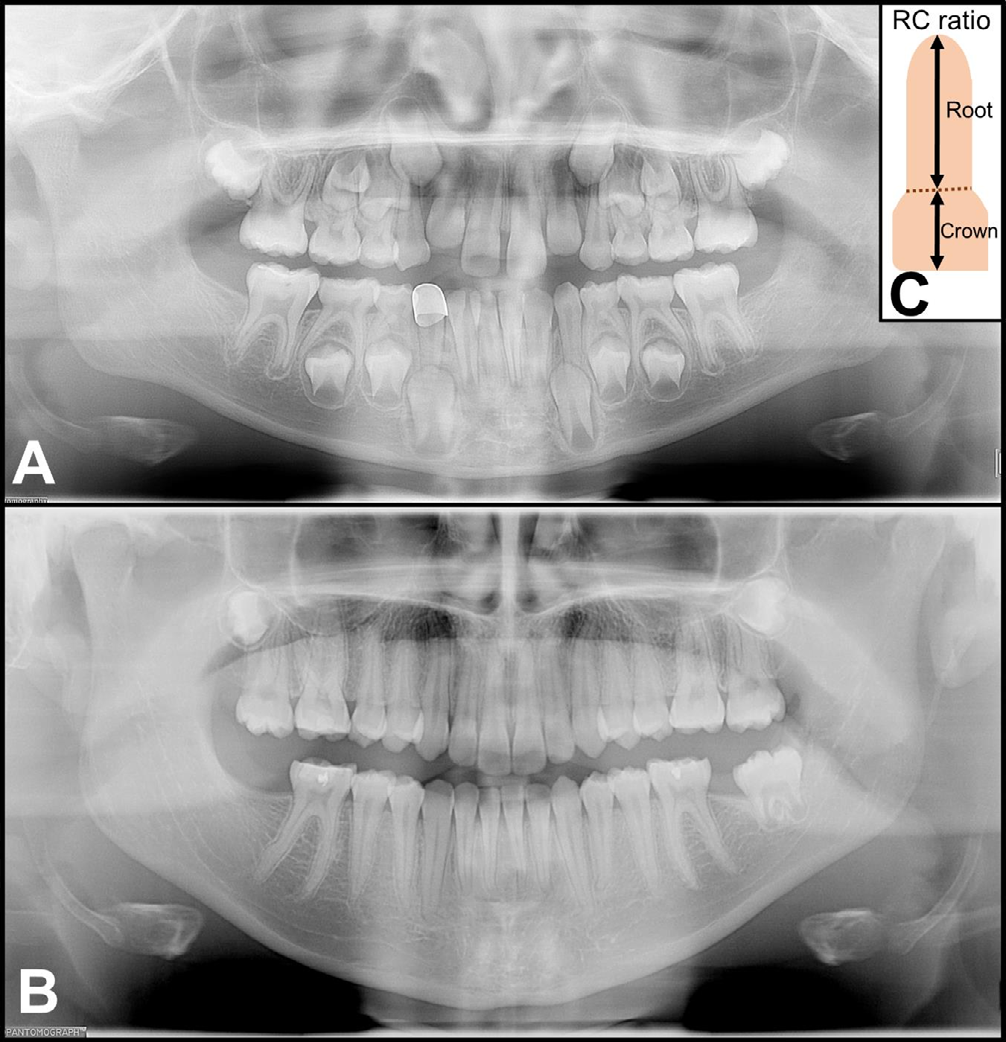
Figure 1: Panoramic radiographs from case 1 taken during mixed dentition (8 years) and permanent dentition (16 years) stages showing non-syndromic, generalized radiculomegaly affecting both primary (A) and permanent dentition (B) along with the schematic to calculate root-crown ratio (C). Note congenital absence of #s 18, 31, and 32 with gemination of #17.
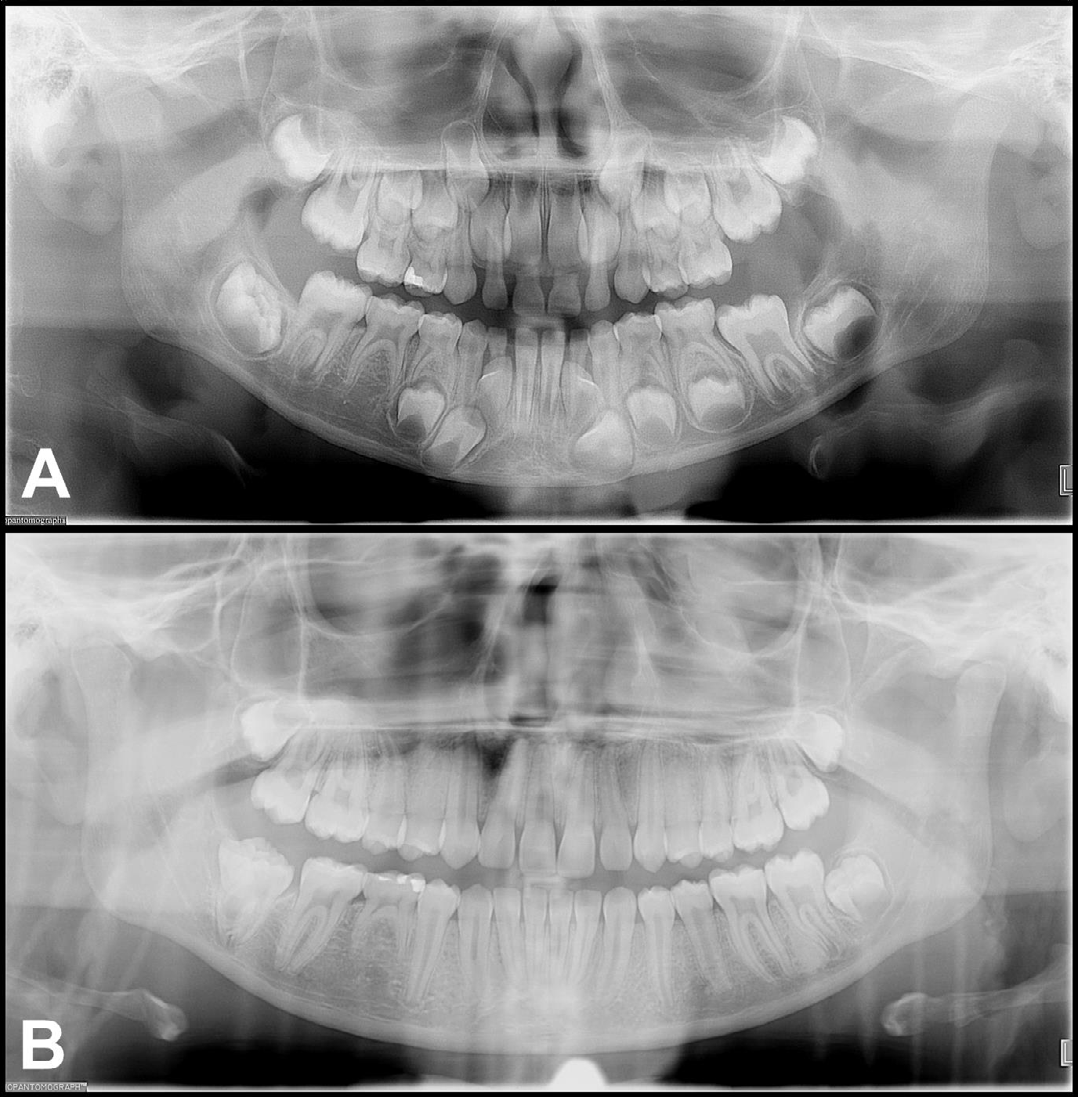
Figure 2: Panoramic radiographs from case 2 taken during mixed dentition (8 years) and permanent dentition (16 years) stages showing non-syndromic, generalized radiculomegaly affecting both primary (A) and permanent dentition (B). Note congenital absence of #s 29 and 31 with gemination of #32. Multiple linear radiopacities are seen vertically on right and left side of the radiographs consistent with braids of hair. The polymeric additives in hair products can be the reason as to why these braids are visible on panoramic radiographs.
Discussion
RM has been previously reported in both the primary and permanent dentition in an individual with oculofaciocardiodental syndrome [3]. Most reported cases of RM have been associated with oculofaciocardiodental, Klinefelter, or Cockayne syndromes [1]. There are only singular reports of localized [2], and generalized [1], non- syndromic RM affecting only primary or permanent dentition, respectively. In the case of localized RM, the patient had a history of cataracts and other ophthalmic anomalies which may indicate undiagnosed oculofaciocardiodental syndrome [2]. This suggests that syndromic RM is rare, but non- syndromic RM is highly rare [1]. Furthermore, non-syndromic RM affecting both the primary and permanent dentition is exceptionally rare [3]. In both the presented cases oculofaciocardiodental, Klinefelter, and Cockayne syndromes were ruled out due to non-significant medical history and age-appropriate development. It is important to note that both the reported cases were unrelated and of different ethnicities. Also, we noted two additional dental anomalies associated with non-syndromic RM: hypodontia and gemination. Hypodontia is a number anomaly while gemination is a shape anomaly; these anomalies were observed in the permanent dentition only. Future evaluation of additional cases of RM is warranted to conclusively confirm such associations. However, it is important to emphasize the need for routine panoramic radiographs for assessment of growth and development including evaluation for dental anomalies during mixed and permanent dentition stages. RM can impact endodontic, orthodontic, and surgical care in pediatric patients. Endodontic treatment of RM-affected teeth would be incredibly challenging with or without dilacerations. Root blunting, secondary to orthodontic treatment, may not impact patients with generalized RM. However, certain orthodontic movements such as intrusion or distalization can bring the root apices closer to the nerve and can lead to transient or permanent paresthesia due to nerve impingement [5]. Concurrent findings such as hypodontia and gemination should also be considered during orthodontic treatment planning. Surgical implications of RM include difficulty in extraction of affected teeth due to long roots and proximity to nerves. Additionally, no data is available on the impact of traumatic dental injuries on RM- affected teeth. Critical review and reporting of RM cases is vital to generate an evidence-base for clinical guidelines regarding management of teeth with RM. It is crucial to provide anticipatory guidance to patients and families regarding the implications of RM and overall dental well- being.
Implications for Dentists
This case series presents exceptionally rare, unrelated, pediatric cases of generalized, non-syndromic radiculomegaly affecting both primary and permanent dentitions. Details on diagnosis and clinical implications of radiculomegaly are provided in this case series for clinical decision-making. Previously unreported dental anomalies associated with radiculomegaly are also provided in this case series.
This case series also underlines the importance of capturing panoramic radiographs during mixed and permanent dentition stages to assess growth, development, and dental anomalies in children.
References
-
Al Obaida M (2020) A Rare Case of Nonsyndromic Generalized Radiculomegaly with a Literature Review. Case Rep Dent 2020: 3974829.
-
Fujimura A, Suetsugu H, Onodera M, Nozaka K, Nozaka Y (2008) Long root of deciduous anterior teeth. Odontology 96(1): 61-64.
-
Nishiguchi M, Sasaki Y, Satoh K, Kamasaki Y, Kondo Y (2018) Long-term observation of a case of oculo-facio- cardio- dental syndrome that showed remarkable radiculomegaly of primary teeth. J Transl Sci 5(2): 1-4.
-
Puranik CP, Hill A, Henderson Jeffries K, Harrell SN, Taylor RW, et al. (2015) Characterization of short root anomaly in a Mexican cohort-hereditary idiopathic root malformation. Orthod Craniofac Res 1: 62-70.
-
Baxmann M (2006) Mental Paresthesia and Orthodontic Treatment. Angle Orthod 76(3): 533-537.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells