Maspin Expression in Salivary Mucoepidermoid Carcinoma: Auclair vs. Brandwein Grading System
Purpose: Maspin is a member of serpin (serine protease inhibitor) family, and is known to have tumor-suppressor function. Maspin has been reported to play a critical role in processes relevant to tumor growth and metastasis such as cell invasion, angiogenesis, and apoptosis. The aim of this study is to evaluate immunohistochemical expression of maspin and its correlation to histologic grade of salivary mucoepidermoid carcinoma. Materials and Methods: A total of 22 formalin-fixed, paraffin-embedded specimens of mucoepidermoid carcinoma were prepared for immunohistochemical staining with maspin antibodies. Maspin immunoreactivity was evaluated by calculating the proportion of positively-stained tumor cells present in 5 high-power fields. Results: All cases were expressed maspin with variable cellular localization. No significant correlation was found between maspin expression and clinicopathologic features such as patient’s age, gender, tumor site, clinical stage and lymph node metastasis (p> 0.05), whereas maspin expression showed a statistically significant correlation with grade of tumors classified in regard to Auclair system (p= 0.011), compared to that evaluated by Brandwein system (p= 0.155). Conclusion: Salivary mucoepidermoid carcinoma showed maspin immunoreactivity with variable levels and cellular localization. Maspin is a valuable biomarker to predict the prognosis of salivary mucoepidermoid carcinoma.
Introduction
Mucoepidermoid carcinoma (MEC) is the most common malignancy of salivary gland origin, accounting for 30% of these neoplasms [1]. It is characterized by diverse histomorphological features and biological behavior of prognosis correlated with histologic grade [2, 3]. Hence, grading methods for MEC are based on different parameters, by which tumors are stratified into low, intermediate, and high grades [4]. Although the grading systems of MEC are enigmatic, time-consuming, and somewhat have complex criteria, they often seem to be prognostically effective and display reproducibility among pathologists [5, 6, 7, 8]. However, the most popular grading schemes which are used to predict the biologic behavior of MEC are: The Auclair system [9], and that proposed by Brandwein, et al. [10].
Maspin is a 42-KDa protein which belongs to the large superfamily referred to as serine protease inhibitors (serpin), including a group of proteins with different biological activities [11, 12]. Despite that the molecular mechanism of maspin is still unclear, its functional domain is thought to be located at reactive central loop (RCL); which is an active site moiety for maspin gene [13]. Moreover, RCL appears to mediate interaction to a cell surface receptor that enhances cell adhesion to type I collagen and fibronectin. Hence, maspin may increase cell-cell adhesion, subsequently prevent tumor invasion and metastasis [14]. In addition, maspin inhibits in vivo, neoplasm-associated angiogenesis [15, 16]. Maspin expression has been demonstrated in different cell types, and appeared to be down-regulated in breast, prostate, and gastric cancers [17, 18, 19]. On the other hand, maspin was over-expressed in pancreatic, gallbladder and thyroid cancers [20, 21, 22]. These controversial views are attributed to the subcellular localization of maspin in different cancer cells (nuclear, cytoplasmic, or pan-cellular expression); via interaction with extracellular matrix (ECM) components, or due to epigenetic modifications [23, 24, 25]. The purpose of this study is to evaluate the immunohistochemical expression of maspin and its correlation with histologic grade of salivary MEC categorized by Auclair and Brandwein systems.
Materials and Methods
A total of 22 formalin fixed, paraffin-embedded MEC specimens were collected from the archives of the Department of Oral Diagnosis/ College of Dentistry/ Baghdad University and Department of specialized surgery in Al-Shaheed Ghazi Hospital in Baghdad. Clinical information concerning the age, gender, and site of tumor and lymph node metastasis was obtained from patients’ medical records, during the period from 2009 to 2017. For all specimens, 4µm thick sections were prepared and stained with hematoxylin and eosin (H&E) stain to confirm the diagnosis. The tumor histologic grade in this study was evaluated according to criteria of Auclair and Brandwein systems that are published in The WHO classification of tumors.
Immunohistochemistry (IHC) of maspin
Immunohistochemical (IHC) staining for maspin was carried out as follows: the tissues were deparaffinized in xylene and rehydrated through graded alcohol and washed with distilled water. According to the manufacturers’ protocol, the slides require no antigen retrieval. To quench endogenous peroxidase activity, the slides were immersed in 3% H2O2 for 20 minutes then washed with phosphate buffer saline (PBS). Nonspecific binding was inhibited by treatment with protein blocks at room temperature for 10 minutes, the sections were incubated with anti-maspin rabbit polyclonal antibody (1:100 dilution; Abcam, Cambridge, UK) at 37 C° for 3 hours and then incubated overnight at 4C in a humidified chamber. Negative control was performed by omitting the primary antibody. After washing with PBS, the tissue sections were incubated with Secondary-Goat anti- rabbit HRP (Abcam) for 15 minutes and the slides were then washed again in PBS. Subsequently, DAB chromogen was applied for antibody staining (brown). The tissues prepared were then allowed to react with Mayer’s hematoxylin for 5 minutes, dehydrated by serial dilution of ascending alcohol and then covered with a cover glass.
IHC Scoring and Statistical Analysis
The degree of IHC staining was evaluated separately by two pathologists who were blinded to the clinicopathologic information. Maspin immunostaining was scored by counting the proportion of positively stained tumor cells in 5 microscopic high power fields that reveal higher immunopositivity as follows: score 1 (<5% positive cells); score 2 (5-50% positive cells); score 3 (>50% positive cells). Subsequently, score 1 was negative (cell positivity=0), or weak (1-5% positive cell), whereas, scores 2 and 3 showed moderate and strong immnoexpression, respectively. A Mann- Whitney test, Kruskal Wallis test, and Spearman´s correlation coefficient test were used to analyze the correlation between maspin immunoreactivity and clinicopathologic features. These analyses were achieved with the assistance of the Statistical program SPPS (Statistical Package for the Social Sciences) version 22.0 for Windows (SPSS, Chicago, IL, USA). A (P<0.05%) was considered statistically significant in all cases.
Results
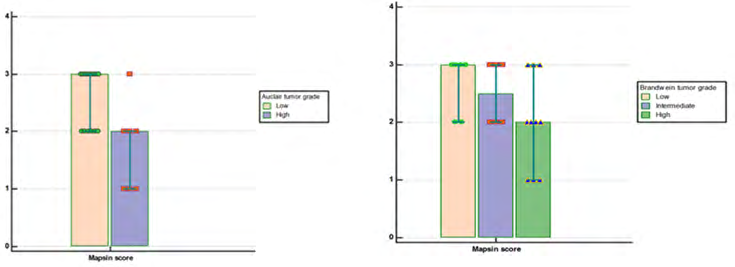
In this study, the cases were distributed according to clinico pathologic features as shown in (Table 1). Regarding IHC results, positive maspin expression was observed in all cases, with different levels and cellular localization. Maspin mainly showed cytoplasmic immunosignaling in both normal ductal epithelium (used as a positive control), and tumor cells of MEC, although in few instances, maspin expression was also localized to the cell membrane, or secreted into extracellular spaces (Figures 1A-E). Table 2 shows the relationship between maspin expression and the clinicopathological features of tumor. However, there was no significant correlation between maspin expression and characteristic parameters as age, gender, site, clinical stage and lymph node status (p>0.05). Maspin expression was found to be correlated significantly with Auclair system (p=0.011), while there was no statistically significant relation between maspin expression and Brandwein system (p>0.05), (Figure 2).
| Total No. | (%) | |
|---|---|---|
| Age group (years) | ||
| <40 | 5 | 22.7 |
| >40 | 17 | 77.3 |
| Gender | ||
| Female | 12 | 54.5 |
| Male | 10 | 45.4 |
| Site | ||
| Major | 11 | 50 |
| Minor | 11 | 50 |
| Clinical stage | ||
| I | 9 | 40.9 |
| II | 7 | 31.8 |
| III | 3 | 13.6 |
| IV | 3 | 13.6 |
| Lymph node status | ||
| -ve | 16 | 72.7 |
| +ve | 6 | 27.3 |
| Auclair grading system | ||
| Low grade | 15 | 68.1 |
| High grade | 7 | 31.9 |
| Brandwein grading system | ||
| I | 6 | 27.3 |
| II | 6 | 27.3 |
| III | 10 | 45.4 |
Table 1: Cases distribution according to Clinicopathologic parameters.
Age group (years)
Gender
Site
Clinical Stage
Parameters Maspin* Maspin* Maspin* p-value
Score 1 Score 2 Score 3
<40 0 3 2 0.13 >40 3 3 8 [NS]
Male 1 4 5 0.87
Female 2 5 5 [NS]
Major 1 5 5 0.8
Minor 2 4 5 [NS]
I-II 1 6 9 0.12
III-IV 3 2 1 [NS]
| Lymph node metastasis | ||||
|---|---|---|---|---|
| N0 | 1 | 6 | 9 | 0.3 |
| N1 | 1 | 1 | 1 | |
| N2 | 1 | 1 | 1 | [NS] |
| Auclair grading system | ||||
| Low grade | 0 | 6 | 9 | 0.011** |
| High grade | 3 | 3 | 1 | |
| Brandwein grading system | ||||
| GI | 0 | 2 | 4 | 0.15 |
| GII | 0 | 3 | 3 | [NS] |
| GIII | 3 | 4 | 3 |
Table 2: Distribution of maspin expression scores.
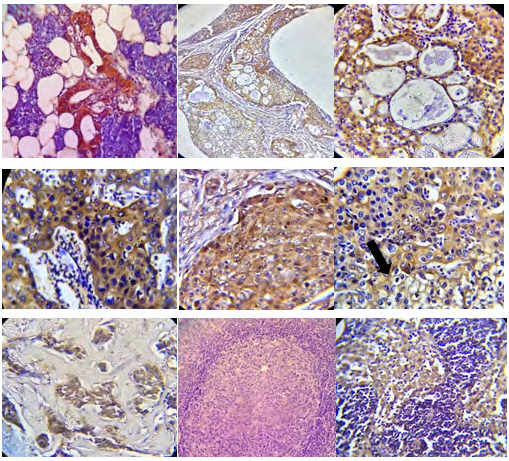
Figure 1: Maspin expression in salivary mucoepidermoid carcinoma. A: normal ductal epithelium in tissue adjacent tumor, showing positive maspin immunoreaction (20x); B: low grade MEC showing macrocystic spaces >25% (20x); C: Higher magnification of the previous case, revealing high cytoplasmic level of maspin (40x); (D): high grade MEC, cytoplasmic and secreted maspin (40x); E: high grade MEC with a solid area showing both nuclear and cytoplasmic pattern of maspin expression (40x); F: maspin expression localizes cell membrane (arrow) of mucous-secretory cells (40x). G: small nest of tumor cell express maspin in high grade MEC (20x). H: lymph node metastasis of MEC (20x). I: maspin overexpression in lymph node associated to MEC (20x).
Discussion & Conclusion
In the present study, we found no significant correlation between maspin immunoreactivity and clinical parameters like patient’s age, sex, and tumor location (major & minor salivary glands). This finding was in agreement with previous studies [26, 27, 28, 29]. In addition, no statistically significant correlation was found between maspin and both clinical stage and lymph node metastasis. This finding was in accordance with a previous report achieved by Ghazy, et al. [30] who found no significant correlation between maspin expression and lymph node involvement and/or postoperative metastasis in salivary gland MEC. However, this observation disagrees with Schwarz, et al. [31], who found that negative expression of maspin protein was mainly localized to the nucleus, and that loss of maspin was significantly associated with advanced stage and lymph node metastasis in common salivary gland tumors. These controversial results may be derived from the small size sample included in this study. Moreover, the analysis of Schwarz, et al. for maspin expression was restricted to salivary gland carcinoma types of intermediate malignancy grade. Additionally, in the aforementioned studies, authors discriminate between nuclear and cytoplasmic maspin expression, of which different biologic behavior may be observed [30, 31]. However, in the present study, we found that maspin was expressed with variable levels and cellular localization, which is similar to the findings of previous reports [30]. To our knowledge, little, if anything is known about the relation of maspin expression to salivary MEC categorized by Auclair and Brandwein methods. Our results indicated that maspin expression was statistically correlated with histologic grade of tumors classified according to Auclair system compared to that graded by criteria of Brandwein system. This finding is in harmony with another recent study [32]. Moreover, high grade MEC is usually demonstrated low maspin expression which could indicate loss of its activity to inhibit tumor invasion, metastasis and angiogenesis [33]. Evidence of both nuclear and cytoplasmic maspin expressions were detected in low grade MEC. This finding denotes that maspin cellular localization has a critical role as a tumor suppressor gene [11, 34]. Furthermore, the relationship of maspin immunoexpression to the tumor grade was evaluated in salivary gland malignancies, and it is found that maspin is overexpressed in low grade salivary MEC, and decreases as the histological malignancy rises regardless of the grading system applied. However, this finding was coincident with previous results [35]. In conclusion, our study showed that maspin is a valuable biomarker to predict the tumor aggressiveness in MEC, and its expression was significantly correlated with tumor grade, especially when tumors are categorized by Auclair system.
References
-
Barnes L, Eveson JW, Reichart P (2005) World Health Organization Classification of Tumors. Patho and Gene of Head and Neck Tumors, Lyon: IARC, pp: 219-220.
-
Luna MA (2006) Salivary Mucoepidermoid Carcinoma: Revisited. Adv Anat Pathol 13(6): 293-307.
-
OI Ahmed, LM Al Azzawi (2020) Salivary mucoepidermoid carcinoma, auclair vs brandwein grading system: A histopathological comparative study. J Baghdad College of Dentistry 32(3): 14-18.
-
Eveson JW, Nagao T (2009) Surgical Pathology of Head and Neck. Informa health care. Barnes pp: 546-552.
-
Ahmed OI, AL Azzawi LM (2019) MTA1 Expression in Salivary Mucoepidermoid Carcinoma: with Special Emphasis on Grading Systems. Journal of International Dental and Medical Research 12(4): 1253-1257.
-
Seethala RR, Bennett A, Arrosi AA, et al. (2008) Reproducibility of grading in salivary gland mucoepidermoid carcinoma and correlation with outcome: does system really matter? Mod Pathol 21: 241.
-
Seethala RR (2009) An update on grading of salivary gland carcinomas. Head Neck Pathol 3(1): 69-77.
-
Hussain QA, Al-Azzawi LM (2014) BAX In situ hybridization and proliferating cell nuclear antigen immunohistochemical expressions in salivary gland tumours. Journal Baghdad College Dentistry 26(1): 112- 120.
-
Auclair PL, Goode RK, Ellis G (1992) Mucoepidermoid carcinoma of intraoral salivary glands: evaluation and application of grading criteria in 143 cases. Cancer 69(8): 2021-2030.
-
Brandwein MS, Ivanov K, Wallace DI, Hille JJ, Wang B, et al. (2001) Mucoepidermoid carcinoma. A clinicopathologic study of 80 patients with special reference to histological grading. Am J Pathol 25(7): 835.
-
Bass R, Fernandez A, Ellis V (2002) Maspin inhibits cell migration in the absence of protease inhibitory activity. J Biol Chem 277(49): 46845-46848.
-
Bailey C, Khalkhali EZ, Seftor E (2006) Biological functions of maspin. J Cell Physiol 209(3): 617-624.
-
Berardi R, Morgese F, Onofri A, Mazzanti P, Pistelli M, et al. (2013) Role of maspin in cancer. Clin Transl Med 2(1): 1-8.
-
Chen EI, Yates JR (2006) Maspin and tumor metastasis. IUBMB Life 58(1): 25-29.
-
Zhang M, Volpert O, Shi Y (2000) Maspin is an angiogenesis inhibitor. Nat Med 6(2): 196-199.
-
Cher ML, Biliran HR, Bhagat S, Meng Y, Che M, et al. (2003) Maspin expression inhibits osteolysis, tumor growth and angiogenesis in a model of prostate cancer bone metastasis. Proc Natl Acad Sci 100(13): 7847-7852.
-
Yu M, Zheng H, Tsuneyama K, Takahashi H, Nomoto K, et al. (2007) Paradoxical expression of maspin in gastric carcinomas: correlation with carcinogenesis and progression. Human Pathol 38(8): 1248-1255.
-
Wu Y, Alvarez M, Slamon DJ (2010) Caspase 8 and maspin are downregulated in breast cancer cells due to CpG site promoter methylation. BMC Cancer 10:1-32.
-
Lovric E, Gatalica Z, Eyzaguirre E (2020) Expression of maspin and glutathionine-S-transferase-pi in normal human prostate and prostatic carcinomas. Appl Immunohistochem Mol Morphol 18(5): 429-432.
-
Shams TM, Samaka RM, Shams ME (2006) Maspin protein expression: a special feature of papillary thyroid carcinoma. J Egypt Natl Canc Inst 18(3): 274-280.
-
Maass N, Hojo T, Ueding M, Luttges J, Kloppel G, et al. (2001) Expression of the tumor suppressor gene Maspin in human pancreatic cancers. Clin Cancer Res 7(4): 817.
-
Kim J, Jang KT, Kim KH, Park JW, Chang BJ, et al. (2010) Aberrant maspin expression is involved in early carcinogenesis of gallbladder cancer. Tumor Biol 31(5): 471-476.
-
Lockett J, Yin S, Li X (2006) Tumor suppressive maspin and epithelial homeostasis. J Cell Biochem 97(4): 651- 660.
-
Solomon LA, Munkarah AR, Schimp VL, Arabi MH, Morris RT, et al. (2006) Maspin expression and localization impact on angiogenesis and prognosis in ovarian cancer. Gynecol Oncol 101(3): 385-389.
-
Mazurkiewicz KD, Narkiewicz J, Milczek T (2009) Maspin overexpression correlates with positive response to primary chemotherapy in ovarian cancer patients. Gynecol Oncol 113(1): 91-98.
-
Lee MJ, Suh CH, Li ZH (2006) Clinicopathological significance of maspin expression in breast cancer. J Korean Med Sci 21(2): 309-314.
-
Osama MG, Lehadh MAl-A, Wisam AH (2015) Immunohistochemical expression of Cyclin D1 in mucoepidermoid and adenoid cystic carcinoma of the salivary glands. Journal Baghdad College Dentistry 27(3): 64-69.
-
Jun LO, Tong J, Wen JY (2008) The expression of maspin in mucoepidermoid carcinoma of salivary gland and its clinical significance. China J Oral Maxillofacial Surg 6: 374.
-
Omer IA, Lehadh MAl-A (2019) MTA1 Expression Correlates Significantly with Histologic Grade in Salivary Mucoepidermoid Carcinoma. Diyala Journal of Medicine 16(1): 1-9.
-
Ghazy ES, Helmy IM, Baghdadi HM (2011) Maspin and MCM2 immunoprofiling in salivary gland carcinoma. Diagn Pathol 6: 89.
-
Schwarz S, Ettl T, Kleinsasser N, Hartmann A, Reichert TE, et al. (2008) Loss of maspin expression is a negative prognostic factor in common salivary gland tumors. Oral Oncol 44(6): 563-570.
-
Taghavi N, Khozestani PK, Baghban A (2017) Clinicopathologic Significance of P63, Maspin and MMP- 2 Expression in Mucoepidermoid Carcinoma. JIDAI 29(1): 21-28.
-
Tarakji B, Ashok N, Sheirawan MK, Altamimi MA, Alenzi F, et al. (2014) Maspin as a Tumour Suppressor in Salivary Gland Tumour. J Clin Diagn Res 8(12): 05-07.
-
Sood AK, Fletcher MS, Gruman LM, Coffin JE, Jabbari S, et al. (2002) The paradoxical expression of maspin in ovarian carcinoma. Clin Cancer Res 8(9): 2924-2932.
-
Sahar MElS, Amani NAEl L (2014) Mapsin expression in mucoepidermoid carcinoma and adenoid cystic carcin. Am J Life Sci 2(3): 182-189.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells