Diagnostic Dilemma in a Rare Jaw Metastasis: A Case Report
Malignant tumors that have metastasized to the oral and maxillofacial region from distant sites account for only 1% of all malignancies of the jaw. These metastasize most often to the mandibular molar region. The commonest primary sources of metastatic tumors found in the oral and maxillofacial region are the lung, kidney and prostate gland for the males, and the breast, genital organs and kidneys for females. Uterine cervix cancer is the second most common female cancer and the third most common cause of female cancer mortality. The tumor spreads into the surrounding tissues by direct infiltration, but hematogenous dissemination is relatively unusual and the involvement of oral and maxillofacial region is extremely rare in gynecological cancer. Here a case of a 45-year-old woman is presented, who had a lesion of sunburst type appearance radiographically and poorly differentiated squamous cell carcinoma histologically involving the maxillofacial region, which metastasized from uterus cervix.
Introduction
Metastatic malignancies found in the oral and maxillofacial region are rare and account for only 1% of all malignancies of the jaw [1, 2, 3, 4, 5, 6, 7, 8, 9, 10]. In 22% to 30% of cases, the oral presentation of metastasis is the first sign of malignant disease [3, 5, 6] in about 67% of cases, metastatic lesions are detected at the same time as the primary lesion [3]. Carcinomas metastasize to the oral region more commonly than sarcomas [3]. The jaw bones are involved more frequently than the oral soft tissues [1, 4, 5]. The mandibular molar region is the most often affected area. Uterine cervix cancer affects about 500,000 women worldwide per year. It is the second most common female cancer and third most common cause of female cancer mortality [11]. The tumor usually spreads into the surrounding tissues by local extension and lymphatic dissemination and the commonest sites are pelvis and abdomen [12, 13, 14]. Hematogenous dissemination is relatively unusual, and most commonly involves distant regions, such as lungs, bones, liver, and extrapelvic lymph nodes. Rare metastases to brain, breast, thyroid, skin spinal cord, kidney, adrenal gland and oral and maxillofacial region have also been reported [13, 14, 15, 16]. They are usually seen late in the course of the disease and have poor prognosis [17, 18]. Oral cavity metastases from cervix uterine cancer seem to be an extremely rare event.
A 45-year-old woman reported to the department of Oral Medicine and Radiology in January 2015 complaining of pain in the left upper and lower back tooth region with associated swelling in the left mid facial region since 20 days. The pain was dull and intermittent when it started and aggravated since few days. There was trismus present which increased during the period of 20 days. Also patient gave history of taking some medications which relieved the pain temporarily with no reduction in swelling. Patient also tried moist heat foamentation to reduce the swelling but to nil effect. When questioned about her symptoms, she reported weakness, breathlessness, but no fever, cough or dyspnea and was unsure of any weight loss. Her medical history revealed that she was diagnosed with poorly differentiated squamous cell carcinoma of cervix 3 years back for which she was treated with course of chemotherapy (4 cycles for 1 year). According to the FIGO classification [19], tumor was defined as IIIb. After 1 year of completion of chemotherapy course patient was diagnosed with recurrence of the carcinoma cervix, following which radiotherapy (50 Gy/25 fractions – Intracavitary radiation therapy) was given for 2 months. Patient had a habit of chewing betel nut for around 15 years which she stopped 3 years back after being diagnosed with carcinoma of cervix. Cranial nerve examination demonstrated no abnormality. Extraoral examination revealed gross facial asymmetry with a solitary diffuse swelling seen over the left middle and lower third of the face, concentrated over the left parotid and masseter muscle attachment, approximately 6 x 5 cm in size, ovoid in shape, skin overlying the swelling appeared stretched with no change in color, and elevation of the ear lobe was noted. Swelling anteroposteriorly extended from the outer canthus of eye beyond the posterior border of ramus of the mandible; superoinferiorly from the ala tragus line to inferior border of the mandible. On palpation all the inspectory findings were confirmed with mild local rise in temperature, firm, tender, pinch-able overlying skin. 2 left submandibular lymph nodes were palpable, firm, mobile, ovoid and enlarged. Mouth opening was reduced to 15mm (Figure 1). Due to limited mouth opening, the intraoral extent of swelling couldn’t be seen. All the teeth were present except 28 and 48. 27, 37 and 38 were tender on percussion. Deep periodontal pocket was present in 37 and 38; grade 1 mobility in 38. No tooth caries was present in the concerned area. Generalized attrition was present and salivary flow was normal from the left Stenson’s duct. Differential diagnosis of metastatic jaw tumor, minor salivary gland tumor, primary intraosseous tumor, mesenchymaltumors and nerve sheath tumors were considered. Blood investigations revealed 10.8gm% hemoglobin and raised ESR (64mm). Patient was negative for HIV and HBsAg. A panoramic view was advised which revealed an ill defined destructive lesion involving the left mandibular angle, ramus, condyle, coronoid process, articular tubercle, maxillary tuberosity with multiple bone remnants seen in condylar region, also the posterolateral wall of the maxillary sinus couldn’t be appreciated. Loss of lamina dura was seen with a band like radiolucency in distal root of 38 (Figure 2a). A slight deviation towards left side was seen due to destruction of left condyle. Later a posteroanterior skull (PA) view was advised which revealed a diffuse soft tissue shadow on the left side with an ill-defined destructive lesion involving the angle and condyle; a sunburst type periosteal reaction could be seen over the angle of the mandible on the same side (Figure 2b). A computerized tomographic (CT) scan was arranged and showed an osteolytic lesion involving condyle, coronoid process, portion of ramus of mandible on left side with lamellar osteogenesis with sunburst configuration. A large soft tissue component measuring 5.5 x 5cm was noted causing cortical thinning at posterolateral wall of maxillary antrum, medially involved the pterygoid muscle, encroaching the parapharyngeal space and laterally involving the masseter muscle and parotid gland, posteriorly extending upto the styloid process. Radiographic differential diagnosis of, secondary metastatic tumor, osteosarcoma and chondrosarcoma were given (Figure 3). Also, a chest radiograph posteroanterior (PA) view revealed a solitary pulmonary nodule at right mid zone (Figure 4). Ultrasonography abdomen was advised which revealed secondaries in liver. Following this, an incisional biopsy was done from the retromolar area under local anaesthesia. Results of the histologic examination showed poorly differentiated squamous cell carcinoma. Histological sections stained with hematoxylin and eosin revealed infiltrative tumor islands within the fibrovascular connective tissue stroma, highly pleomorphic tumor cells with cellular and nuclear atypia, large areas of necrosis and hemorrhage, infiltration into the muscle bundles, chronic inflammatory infiltrate predominantly of lymphocytes and numerous vessels lined by epithelium with engorged RBCs(Figure 5) So the final diagnosis of maxillofacial metastatic squamous cell carcinoma of uterine cervix was given.

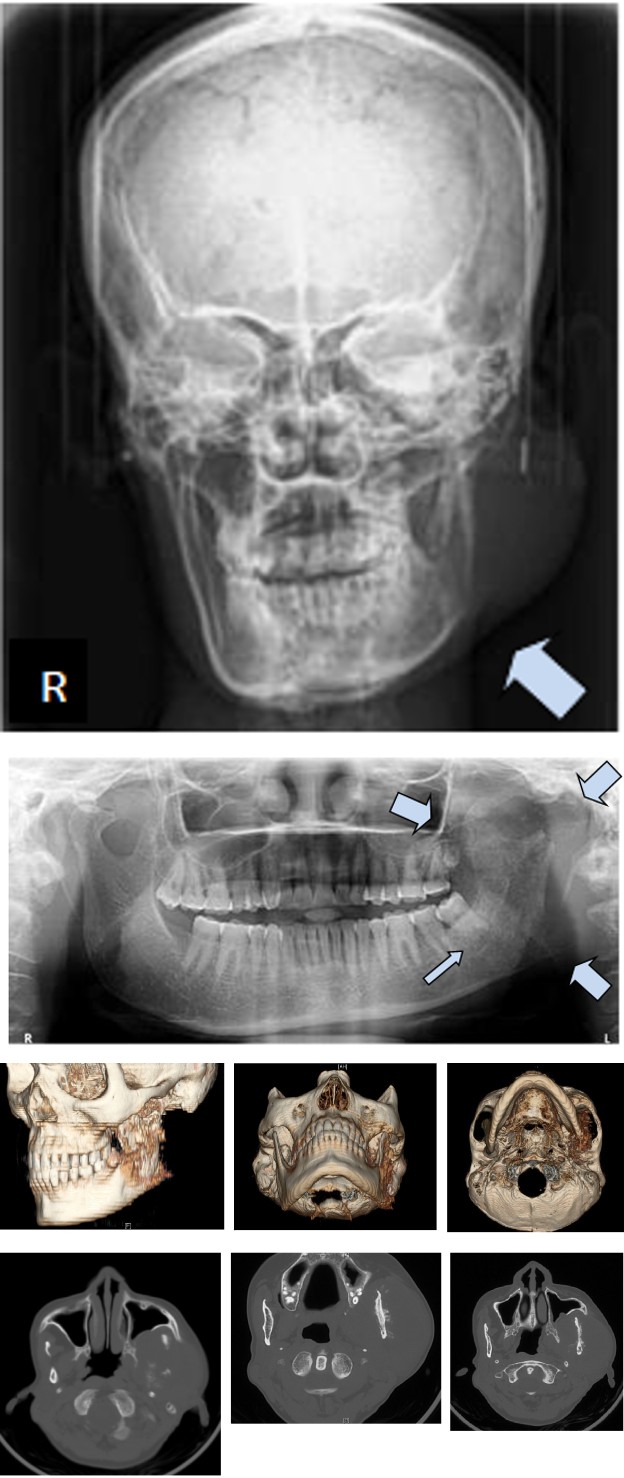
Figure 2A: Panoramic view showing destructive lesion involving the left mandibular angle, ramus, condyle, coronoid process, articular tubercle, maxillary tuberosity with multiple bone remnants seen in condylar region, the posterolateral wall of the maxillary sinus is involved, loss of lamina dura seen with a band like radiolucency in distal root of 38 suggestive of an intraosseous malignant tumor. A slight deviation towards left side was seen due to destruction of left condyle (blank arrows).
Figure 2B: Posteroanterior skull (PA) view revealing a diffuse soft tissue shadow on the left side with an ill defined destructive lesion involving the angle and condyle; a sunburst type periosteal reaction could be seen over the angle of the mandible on the same side (blank arrows).
Figure 3: A computerized tomographic (CT) showing an osteolytic lesion involving condyle, coronoid, portion of ramus of mandible on left side with lamellar osteogenesis with sunburst configuration (red oval). A large soft tissue component measuring 5.5 x 5cm can be noted causing cortical thinning at posterolateral wall of maxillary antrum, medially involving the pterygoid muscle, extending upto the parapharyngeal space and laterally involving the masseter muscle and parotid gland, posteriorly extending upto the styloid process (blank arrows).

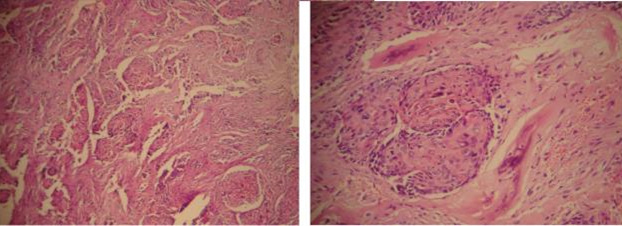
Figure 5: Histological sections stained with hematoxylin and eosin (40x) revealing fragments of a bony tissue stroma infiltrated by cells arranged in lobules and nests. The cells forming the nests exhibited pleomorphism, increased mitosis and squamous differentiation. Few of the islands showed peripherally, palisaded basaloid cells. Also cluster of cells exhibiting stratified and clear cytoplasm were seen (100x).
Discussion
Metastasis is potentially inherent in any malignant tumor. These tumors most often involve regional lymph nodes rather than distant organs [3]. Metastasis is the result of a multistage process in which the proliferating cells detach themselves from the primary tumor, move into the vascular or lymphatic vessels until they lodge in a capillary bed, following which, the cells penetrate the blood vessel walls, enter the surrounding tissues and proliferate within the recipient site [1, 4]. The oral and maxillofacial region metastasis may occur by way of Batson’s plexus, bypassing the filtering capabilities of the lungs. These tumors occur more frequently in the jaw bones than in the oral soft tissues, and in people in their 5th to 7th decade. The mean age (45 years) of patients with metastases to the jawbones is lower than that (54 years) of those with metastases to the oral soft tissues [1]. These metastases occur most often (82% to 85%) in the mandibular molar region, followed by the premolar region, but rarely in the condyle [1, 5, 6, 8, 10]. The primary sites for metastasis to the oral and maxillofacial region for men are the lung, kidney and prostate gland, and for women, the breast, genital organs and kidneys [1, 3, 5, 8]. According to the English literature (1928-2012) only 20 cases of uterus cervix were reported metastasizing to the oral cavity (Table 1). In the uterus, the most common site was the endometrium, and the present case is the oral metastasis from cervix uteri.
| Age (years) | Site | Oral site | Histologic type | |
|---|---|---|---|---|
| Holland (1953) | 61 | Uterus, cervix | Mandible | Carcinoma |
| Salman and Langel (1954) | 64 | Uterus, unspecified | Mandible | Carcinoma |
| Uhler, et al. (1972) | 41 | Uterus, cervix | Mandible | Carcinoma |
| Orlian (1977) | 62 | Uterus, endometrium | Maxilla | Adenocarcinoma |
| Kaziro (1981) | 59 | Uterus, unspecified | Dorsum tongue | Leiomyosarcoma |
| Tsounias (1988) | 67 | Uterus, unspecified | Mandible | Leiomyosarcoma |
| Davidson and Moyo (1991) | 44 | Uterus, cervix | Gingiva | Carcinoma |
| Maxymiw, et al. (1991) | 63 | Uterus, endometrium | Mandible | Carcinoma |
| Baden, et al. (1992) | 78 | Uterus, endometrium | Tongue | Carcinoma |
| Allen, et al. (1993) | 65 | Uterus, unspecified | Lower lip | Leiomyosarcoma |
| Saiz, et al. (1998) | 49 | Uterus, unspecified | Floor of the mouth, parotid gland | Leiomyosarcoma |
| Galen (1998) | 55 | Uterus, endometrium | Mandible | Adenocarcinoma |
| Persson, et al. (1998) | 55 | Uterus, unspecified | Tongue | Leiomyosarcoma |
| Dosortez, et al. (1999) | 71 | Uterus, endometrium | Mandible | Adenocarcinoma |
| Rocha, et al (2000) | 67 | Uterus, endometrium | Mandible | Adenocarcinoma |
| Medina et al. (2001) | 67 | Uterus, corpus | Gingiva | Angiosarcoma |
| Vora e Levin (2003) | 62 | Uterus, unspecified | Tongue | Leiomyosarcoma |
| Bodner, et al. (2006) | 75 | Uterus, unspecified | Mandible | Adenocarcinoma |
| Kim, et al. (2009) | 56 | Uterus, unspecified | Gingiva | Leiomyosarcoma |
| Carvalho, et al. (2012) | 72 | Uterus, cervix | Palate | Carcinoma |
| Present case | 45 | Uterus, cervix | Mandible, maxilla, masseter and pterygoid muscles, parotid gland | Carcinoma |
Table 1: Oral site & Histologic type.
In the present case, the intraoral findings were not much appreciable but radiographic examination (Panoramic, PA skull, CT) revealed an osteolytic lesion involving condyle, coronoid process, portion of ramus of mandible on left side with lamellar osteogenesis with sunburst configuration, cortical thinning at posterolateral wall of maxillary antrum, medially involving the pterygoid muscle, encroaching the parapharyngeal space and laterally involving the masseter muscle and parotid gland, posteriorly extending upto the styloid process. Also, a chest radiograph posteroanterior (PA) view revealed a solitary pulmonary nodule at right mid zone and USG abdomen revealed the secondaries in liver; confirming that the metastatic route was hematogenous and through the liver and lung.. The present case is also rare as it shows extensive involvement of maxilla and mandible along with the muscles and a gland.
The number of metastases is a significant factor in the treatment of malignant tumors that have metastasized to the maxillofacial region [20]. If the lesion in the maxillofacial region seems to be controlled and if other metastatic foci have been ruled out, surgical excision of the metastatic oral lesion is the preferred treatment if the patient’s general health allows the procedure [20]. In 22% to 30% of cases, metastasis to the oral and maxillofacial region may be the first sign of malignant disease, and investigations like bone scans done after the detection of tumors of unknown origin that have foci in this region are very significant [3, 5, 6]. However, metastases to oral and maxillofacial region are usually evidence of widespread disease and indicate a poor prognosis [1, 10]. The majority of patients die some months after the appearance of an oral lesion. And even in cases of advanced malignant disease, it is essential to provide palliative treatment for the control of pain, bleeding and mastication impairment to improve the patient’s quality of life [1].
The patient was referred to regional oncology centre for further investigations and treatment. At the time of writing the manuscript patient is on palliative treatment and the prognosis is poor.
Conclusion
Correlation and critical evaluation of history, clinical picture, radiographic findings and histopathology is necessary as in this case the radiological ‘sunburst’ appearance was suggesting osteosarcoma, whereas histopathological report was directing towards poorly differentiated squamous cell carcinoma. But the medical history and aforementioned features together pointed out to a metastatic lesion from cervix to maxillofacial region. A squamous cell carcinoma of uterine cervix metastasizing to maxillofacial region is very rare and to the best of our knowledge, this is the first report of this kind of presentation.
References
-
Hirshberg A, Buchner A (1995) Metastatic tumors to the oral region. An overview. Eur J Cancer B Oral Oncol 31(6): 355-360.
-
Vähätalo K, Ekfors T, Syrjänen S (2000) Adenocarcinoma of the pancreas metastatic to the mandible. J Oral Maxillofac Surg 58(1): 110-114.
-
Scipio JE, Murti PR, Al-Bayaty HF, Matthews R, Scully C, et al. (2001) Metastasis of breast carcinoma to mandibular gingiva. Oral Oncol 37(4): 393-396.
-
Vieira BJ, Aarestrup FA, da Fonseca EC, Dias EP (2001) Bilateral gingival metastasis of lung adenocarcinoma: report of a case. J Oral Maxillofac Surg 59(10): 1224- 1225.
-
Fukuda M, Miyata M, Okabek K, Sakashita H (2002) A case series of 9 tumors metastatic to the oral and maxillofacial region. J Oral Maxillofac Surg 60(8): 942- 944.
-
Willard CC, Weber CR, Buche W (2002) Metastatic esophageal adenocarcinoma involving the maxilla. J Oral Maxillofac Surg 60(12): 1496-1499.
-
Smolka W, Brekenfeld C, Büchel P, Iizuka T (2004) Meta- static adenocarcinoma of the temporomandibular joint from the cardia of the stomach: a case report. Int J Oral Maxillofac Surg 33(7): 713-715.
-
Lim SY, Kim SA, Ahn SG, Kim HK, Kim SG, et al. (2006) Metastatic tumors to the jaws and oral soft tissues: a retrospective analysis of 41 Korean patients. Int J Oral Maxillofac Surg 35(5): 412-415.
-
Jordan RC, Daniels TE, Greenspan JS, Regezi JA (2002) Advanced diagnostic methods in oral and maxillofacial pathology. Part II: Immunohistochemical and immunofluorescent methods. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 93(1): 56-74.
-
Miles BA, Schwartz-Dabney C, Sinn DP, Kessler HP (2006) bilateral metastatic breast adenocarcinoma within the temporomandibular joint: a case report. J Oral Maxillofac Surg 64(4): 712-718.
-
Monk BJ, Willmott LJ, Sumner DA (2010) Anti- angiogenesis agents in metastatic or recurrent cervical cancer. Gynecol Oncol 116(2): 181-186.
-
Jamshed A, Khafaga Y, El Husseiny G, Gray AJ, Manji M, et al. (1995) Pericardial metastasis in carcinoma of the uterine cervix. Gynecol Oncol 61(3): 451-453.
-
Dimitrakopoulos I, Ntomouchtsis A, Iordanidis F (2011) Infratemporal fossa metastasis from carcinoma of the uterine cervix. Oral Maxillofac Surg 15(2): 121-125.
-
Park SH, Ro DY, Park BJ, Kim YW, Kim TE, et al. (2010) Brain metastases from uterine cervical cancer. J Obstet Gynaecol Res 36(3): 701-704.
-
Challagalla JD, Smith R, Mitnick R, Breining D, Wadler S, et al. (1999) Carcinoma of the uterine cervix metastatic to behind the zygomatic arch: a case report. Am J Otolaryngol 20(3): 195-197.
-
Mohanty A, Dutta D, Das S, Samanta D, Senapati S, et al. (2010) Skull metastasis from carcinoma of the cervix: a rare case and review of the literature. J Obstet Gynaecol Res 36(2): 441-443.
-
Van der Waal RI, Buter J, van der Waal I (2003) Oral metastases: report of 24 cases. Br J Oral Maxillofac Surg 41(1): 3-6.
-
Hirshberg A, Shnaiderman-Shapiro A, Kaplan I, Berger R (2008) Metastatic tumors to the oral cavity - pathogenesis and analysis of 673 cases. Oral Oncol 44(8): 743-752.
-
Kosary CL (1994) FIGO stage, histology, histologic grade, age and race as prognostic factors in determining survival for cancers of the female gynecological system: an analysis of 1973-87 SEER cases of cancers of the endometrium, cervix, ovary, vulva, and vagina. Semin Surg Oncol 10(1): 31-46.
-
Hashizume A, Nakagawa Y, Nagashima H, Ishibashi K (2000) Rectal adenocarcinoma metastatic to the masseter muscle. J Oral Maxillofac Surg 58(3): 324-327.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells