Cysts of Oral Cavity: Odontogenic Keratocyst; A Rare Case Report with a 6-Year Follow-Up
Aim: Odontogenic keratocyst is one of the rare odontogenic cyst, commonly affecting the mandible. It has a special mention in the field of oral surgery due to its varied presentation and high recurrence rate. There have been a few cases reported of outcomes of treatment of odontogenic keratocysts. The aim of this report was to illustrate the case of OKC in a patient and to describe the follow-up information and successful treatment of its. Methods: A 18-year-old Turkish girl was referred by her dentist to the periodontology clinic of the Faculty of Dentistry in November 2017, for the treatment of cyst in the mandibulary incisor region. The diagnosis of odontogenic keratocyst suggested clinically and radiographically was confirmed by the histopathological study. Treatment consisted of oral hygiene instruction, periodontal-endodontic treatment and resection of cyst. Results: Four weeks after surgery healing was occurred and six years later area of the lesion appeared completely normal as clinical and radiographically. There were no signs of local recurrence after a 6-year follow-up. Conclusion: The odontogenic keratocyst was treated successfully by surgical periodontal treatment
Introduction
There have been a few nomenclature and classifications of odontogenic cysts and tumours since 1869. Since the first odontogenic tumours and jaw cysts classification of the World Health Organization (WHO) in 1971, Odontogenic keratocysts (OKC) have been regarded as a special lesion. In recent classification, one of the most significant changes in 2017 was that “keratocystic odontogenic tumor” was moved from the neoplastic category (2005) back into the cyst category (2017), and listed as OKC in the 2017 classification of developmental odontogenic cysts [1, 2, 3]. Although most research on classification of odontogenic cysts has been based on histopathological features and some clinical considerations, there is no international consensus on the question of the OKC’s nature.
OKC is the one of the sparse developmental odontogenic lesion, which attracts many researchers due to its unique characteristics, such as high mitotic rate, high recurrence rate, tendency to invade adjacent tissues, association with genetic and chromosomal abnormalities (i.e. p53 gene, PTCH gene, Nevoid Basal Cell Carcinoma Syndrome) [3]. It is an enigmatic lesion that reflects aggressive clinical behavior. The aggressive nature of OKC has been attributed not only to the presence of matrix metalloproteins (MMP 2 and 9) as well as interleukin-1 alpha and parathyroid hormone related protein but also to the presence of antiapoptotic proteins (B cell lymphoma 2; Bcl-2) and cytokeratin 10, leading to the rate of recurrence [4]. The incidence of recurrence of OKC was reported up to 62% after surgical treatment. Theoretically, the frequent recurrence of OKC is related with multiple factors including size and location of the lesion, therapy modalities, timing, duration of follow-up period, cooperation, surgery experience and presence of Nevoid Basal Cell Carsinoma Syndrome, etc. [5].
OKC originates from the dental lamina remnants and basal cells of overlying epithelium. It is a rare most notorious cyst and make up around 19% of jaw cysts [2], but it may be asymptomatic and encountered incidentally on dental radiographs. If symptoms can arise, they are due to infection or expansion of bone [6].
Odontogenic keratocyst (OKC) was first defined in 1876. Since then, there have been a few cases report of outcomes of treatment of OKC. Therefore, the aim of this report was to illustrate the case of OKC in a patient and to describe the follow-up information and successful treatment of its. This case has been reported in accordance to the SCARE criteria [7].
Case Report
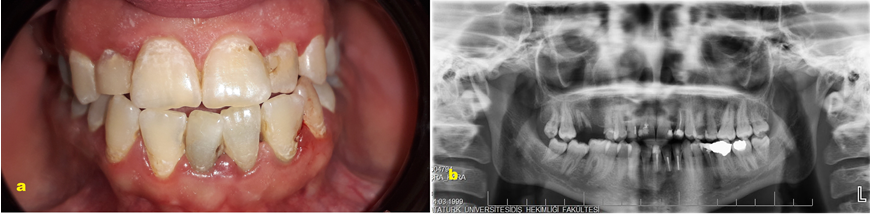
A 18-year-old Turkish girl was referred by her dentist to the periodontology clinic of the Faculty of Dentistry in November 2017, for the treatment of cyst in the mandibular incisor region. The patient had reported with a chief complaint of sensitivity in the lower front teeth for five months. The patient reported that the lesion was discovered as an incidental finding by her dentist during the radiographic examination (Figure 1a). The patient denied pain or any other symptoms. The patient’s medical history was non-contributory, he did not take any medications, had no known allergies, and was non-smoker.
Extra-oral examination showed no alterations including asymmetry, discharge or sinus tract (Figure 1b). On palpation of the lower chin, no tenderness was present.
On intra-oral examination, there was a painless slightly yellowish swelling on muco-gingival junction with no sinus tract observed on the mandibular incisor region (Figure 1c). Also, there was a slightly gingival bleeding and gingival reddish associated with accumulation of dental plaque. Other findings included a mild supra-gingival calculus around her teeth, presence of carious lesions and filling teeth, and tooth mal-positioning of mandibular incisor teeth. The expansion of bone was not detected in the associated region (Figure 1d). Three teeth adjacent to the lesion were sensitive to percussion but not mobile. The teeth were found to be vital to electric pulp testing.

A panoramic radiography revealed radiolucent, a well- circumscribed, unilocular lesion, located in the mandibular incisor region, between the roots of the lower incisors (#31, #32, #41), measuring about 20×20mm in diameter. Loss of lamina dura surrounding the adjacent teeth was observed. Resorption of adjacent teeth was absent. In addition, a slight divergence of the roots of the teeth was observed (Figure 1a). It was provisionally diagnosed as an OKC of developmental origin.
Treatment protocol planned was endodontic treatment followed by periodontal surgery (Figure 2a). Before the endodontic treatment of teeth for 32, 31 and 41, the patient underwent scaling, root planning, and crown polishing. The patient was educated regarding good oral hygiene maintenance practices. Written informed consent was obtained from the patient after all treatment procedures had been fully explained.
Surgical Procedure
Periodontal surgery was done under strict aseptic conditions using local anesthesia& (&Ultracaine DS Forte®, Hoechst Roussel, Frankfurt, Germany). A crevicular incision was made around the labial surfaces of the mandibular right first- and left-incisors, and a vertical incision was made the mesial aspect of teeth, a full-thickness flap was elevated to expose the bone. Cystic lining was separated from the bone and dissected from the underlying mucosa. Apicectomy and retrograde filling was done with glass ionomer cement with respect to 32, 31 and 41. Curettage of cystic lesion was done within the cystic cavity followed by sharp bony margins were reduced by means of bone bur and rotary instruments with copious saline irrigation and the socket was debrided with Povidone-Iodine§ (§Glividon®, Bikar Drug Ltd., Turkey) and saline solution. The specimen was immersed in 10% formaldehyde and sent for histological analysis (Figures 2b and 2c). The flap was sutured with 3-0 non-resorbable silk suture and covered with periodontal dressing (Figure 2d). Histopathological examination showed the typical features of an OKC (Figure 2e). After having undergone clinical and radiographical examinations and laboratory evaluation in the pathology department, she was diagnosed as having OKC.
The patient was prescribed analgesics (Naproxen£ 550mg, every 12 hours, 5 days, £Apranax®, Abdi İbrahim Drug Ltd., Istanbul, Turkey) and instructed to rinse twice daily with 0.12% chlorhexidine rinse¶ (¶Kloroben®, Drogsan Drug Ltd., Istanbul, Turkey) for 2 weeks postoperatively and to avoid trauma or pressure at the surgical site. Toothbrushing activities in the operated sites were discontinued during this time. The sutures were removed 10 days after surgery, home care instructions were given. Professional prophylaxis was done weekly for the first month and then at 6-month interval.
Clinical Observations and Follow-up
Four weeks following surgery, the affected area had completely healed, and there were no complications. The patient’s plaque control was good, although moderate tooth staining was apparent (Figure 2f and 2g).

Figure 2: a) View of the panoramic radiograph after endodontic treatment; b) Clinical view at the time of surgery phase; c) Photograph showing macroscopic aspects of the lesion; d) Immediate postoperative view following surgery; e) Histopathological view of the lesion. (×100 magnification, HE staining); f and g) Postoperative clinical and occlusal view four weeks after surgery.
The patient was periodically observed until six years after our treatment began. Follow-up of the case, showed uneventful recovery and spontaneous regeneration of bone in panoramic radiography (Figure 3a and 3b). Because of the high recurrence rate OKC, periodic follow-up for the next five years has been advised to the patient at least twice a year.
Discussion
The differential diagnoses of radiolucencies that occur in the jaw bones include a broad spectrum of cysts and tumors of odontogenic and non-odontogenic. Odontogenic cysts are one of the most common lesions, which are best classified as inflammatory origin and developmental origin [1, 2, 3]. The lesions are often discovered on routine radiographic examination, since pain or other clinical symptoms have seldom been reported, as was observed in this case.
The OKC is a sparse developmental odontogenic cyst, which develops in the jaws bone. Most OKCs are located in the posterior mandible (65%), followed by the maxilla and gingival/alveolar mucosa. The lesion has a slight predilection for males, which are in the second to fourth decades of life [8, 9, 10]. The case described here demonstrates that an adolescent female patient has an OKC in the anterior mandible.
Radiographs of the OKC show a well-circumscribed radiolucent area, usually with a cortical border, sometimes curved internal septa may be present. The lesion may have a smooth, round or oval shape, identical to that of other cysts, or it may have a scalloped outlined. Loss of lamina dura and periodontal ligament space may be noted. Divergence of the roots is a common, occasionally displace, and resorption of adjacent teeth has be documented [11, 12, 13, 14, 15, 16]. An important characteristic of OKC is its propensity to grow along the internal aspect of the jaws, causing minimal bone expansion. In the present case, radiographic features of an OKC was observed.
While thorough clinical and radiographic assessments are necessary, the diagnosis of OKCs is ultimately dependent on histopathologic findings [3, 6]. It’s histopathologic findings incorporate an uniform parakeratinized stratified squamous epithelium of 5-10 cell layers, secured by a thin ridged layer of parakeratin characteristic palisaded pattern with uniform nuclei are seen in the basal cell layer (like a tombstone appearance). The fibrous cyst wall is relatively thin and usually lacks inflammatory cell infiltrate [10, 11, 12]. There have been reports of lesions clinically diagnosed as corresponding to developmental cysts, but which were found to be malignant lesions in the histological study [5, 12]. This illustrates the importance of histopathological evaluation. Therefore, histopathological examination was done in our case.
The differential diagnosis of OKC includes gingival cyst, radicular cyst, and lateral periodontal cyst. The gingival cyst is a rare soft tissue odontogenic cyst that presents similar epidemiological features to the OKC. In contrast, there are no radiological findings for the gingival cysts [6, 16]. In most cases the differential diagnosis must be established with radicular cysts, in view of their high frequency. These lesions are characterized by necrosis of the affected teeth, as a result of which vitality testing proves negative [2, 3]. In the present case, detailed clinical and radiographic exams were carried out.
In the case presented here, treatment of the OKC was done surgical therapy. Several treatment approaches for OKCs have been suggested in the literature, which are conservative and aggressive approaches. The conservative approach includes simple enucleation and marsupialization of cysts. Enucleation is the most commonly used treatment method and is associated with a high recurrence rate. Aggressive approach includes chemical curettage with Carnoy’s solution, peripheral osteotomy, and bone resection [4, 5, 6]. It is showed that lesion’s enucleation plus chemical cauterization with Carnoy’s solution, significantly reduced the recurrence rates to about 8% [13, 16]. Eventually, there is no evidence in the literature that would guide surgeons in selecting the best treatment options. Hence, treatment of the present case was planned and made with endodontic therapy followed by periapical surgery (apicectomy) and retrograde filling.
Conclusion
The OKC was treated successfully by surgical periodontal treatment. The clinical, radiographic and histopathological evaluations are essential for this lesion, since it is the only way to discard a malignant process and further complications such as highly aggressive and high recurrence rate. Long term periodic follow-up is needed to identify recurrences at the earliest.
References
-
Kramer IR, Pindborg JJ, Shear M (1992) The WHO Histological Typing of Odontogenic Tumours. A commentary on the Second Edition. Cancer 70(12): 2988-2994.
-
Philipsen HP, Reichart PA (2006) Classification of odontogenic tumours. A historical review. J Oral Pathol Med 35(9): 525-529.
-
Soluk-Tekkeşin M, Wright JM (2018) The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2017 (4th) Edition. Turk J Pathol 34(1).
-
Zhong WQ, Chen G, Zhang W, Ren JG, Wu ZX, Zhao Y, Liu B, Zhao YF (2015) Epithelial-mesenchymal transition in keratocystic odontogenic tumor: possible role in locally aggressive behavior. Biomed Res Int 2015: 168089.
-
Ye P, Wei T, Gao Y, Zhang W, Peng X (2021) Primary intraosseous squamous cell carcinoma arising from an odontogenic keratocyst: case series and literature review. Med Oral Patol Oral Cir Bucal 26(1): 49-55.
-
Prashanth BR, Vidhya MS, Karale R, Kumar GV (2020) Is odontogenic keratocyst an endodontic enigma? A rare case report of management of odontogenic keratocyst in anterior mandible. J Oral Maxillofac Pathol 24(1): 7-10.
-
Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler AJ, Orgill DP; SCARE Group (2018) The SCARE 2018 statement: Updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg 60: 132-136.
-
Lunawat SD, Kunte VR, Bhoosreddy AR, Gade LP, Patil RS (2020) Odontogenic Keratocyst: A Rare Presentation in Anterior Maxilla. J Coll Physicians Surg Pak 30(11): 1226-1229.
-
Rodrigues BT, Israel MS, de Moura KL, Pinheiro GL, Carlos R, et al. (2020) Peripheral odontogenic keratocyst: Report of two new cases and review of the literature. J Clin Exp Dent 12(10): 1005-1010.
-
Khan AA, Qahtani SA, Dawasaz AA, Saquib SA, Asif SM, et al. (2019) Management of an extensive odontogenic keratocyst: A rare case report with 10-year follow-up. Medicine (Baltimore) 98: e17987.
-
Kolár Z, Geierová M, Bouchal J, Pazdera J, Zboril V, et al. (2006) Immunohistochemical analysis of the biological potential of odontogenic keratocysts. J Oral Pathol Med 35(2): 75-80.
-
Wysocki GP (1981) The differential diagnosis of globulomaxillary radiolucencies. Oral Surg Oral Med Oral Pathol 51(3): 281-286.
-
Johnson NR, Batstone MD, Savage NW (2013) Management and recurrence of keratocystic odontogenic tumor: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol 116(4): 271-276.
-
Vijayarangan S, Baskara Pandian V (2019) Management of the Odontogenic Keratocyst - Six Cases with Conservative Management Supported by Chemical and Electrochemical Cauterization. Cureus 11(11): 6260.
-
Nayak MT, Singh A, Singhvi A, Sharma R (2013) Odontogenic keratocyst: What is in the name? J Nat Sci Biol Med 4(2): 282-285.
-
Stoelinga PJW, Slusarenko da Silva Y (2020) The significance of recurrent odontogenic keratocysts in bone grafts. Int J Oral Maxillofac Surg 50(6): 746-749.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells