Orthodontic Treatment of an Ankylosed Maxillary Incisor Using a Combination of Surgical Luxation and Temporary Anchorage Device: A Case Report
When anterior tooth ankylosis happens before growth is completed, it leads to dentoalveolar vertical discrepancy which causes anterior openbite and aesthetic concerns. This case report presents a minimally aggressive approach for treatment of an ankylosed tooth in an adult patient using surgical luxation along with temporary anchorage device and vertical elastics. At the end of treatment, the anterior openbite was corrected with extrusion of the ankylosed incisor. The smile arc was significantly improved and the patient was satisfied with the results.
Introduction
External replacement resorption (ERR) also known as tooth ankylosis, is caused by fusion of cementum or dentin to the alveolar bone [1]. This problem could occur in both deciduous and permanent dentitions in different stages of tooth eruption [2]. The periodontal ligament (PDL) continuity disappears as a result of ankylosis. When 20% or more of the root surface is involved with , the physiologic tooth mobility is lost [3].
Ankylosis happens for multiple reasons including: trauma -especially severe luxation and avulsion- , metabolic disorders, local metabolic changes, periapical infections, chemical or thermal irritation, previous surgical procedures, and genetic predisposition [3, 4, 5, 6].
Complications of tooth ankylosis vary depending on tooth/alveolar developmental stage. If this occurs in growing patients, it causes infra-position of the tooth, tipping of adjacent teeth, dental midline shift to the ankylosed side, ridge deformity, and esthetic and occlusal problems. But if ankylosis happens after the growth is completed, it can be managed more easily by prosthodontics replacement [1, 7].
Various diagnostic signs, such as percussion (metallic sound) and radiographs (obliteration of the PDL), have been proposed to diagnose ankylosed teeth. However, in some studies lack of response to orthodontic force have mentioned as the most obvious one. As these teeth do not move by application of orthodontic force, they can complicate the orthodontic treatment [8, 9, 10].
Different treatment modalities have been suggested for treatment of patients with ankylosed teeth, including tooth extraction and replacement with prosthesis, orthodontic space closure, distraction osteogenesis (DO), and surgical luxation [9, 11, 12].
This case report describes surgical luxation of an ankylosed maxillary lateral incisor, followed by orthodontic force application using temporary anchorage devices (TADs).
Diagnosis
A 23-year-old woman was referred to orthodontic clinic with chief complaint of infra-occlusal left maxillary lateral incisor. She sought alignment of anterior teeth as well as a more attractive smile.
She had no special medical situation and mentioned no history of dental or facial trauma. Intraoral examination of the left lateral incisor revealed no physiologic mobility and the tooth had sharp metallic sound on percussion. There was a 4 mm vertical discrepancy relative to adjacent central incisor.
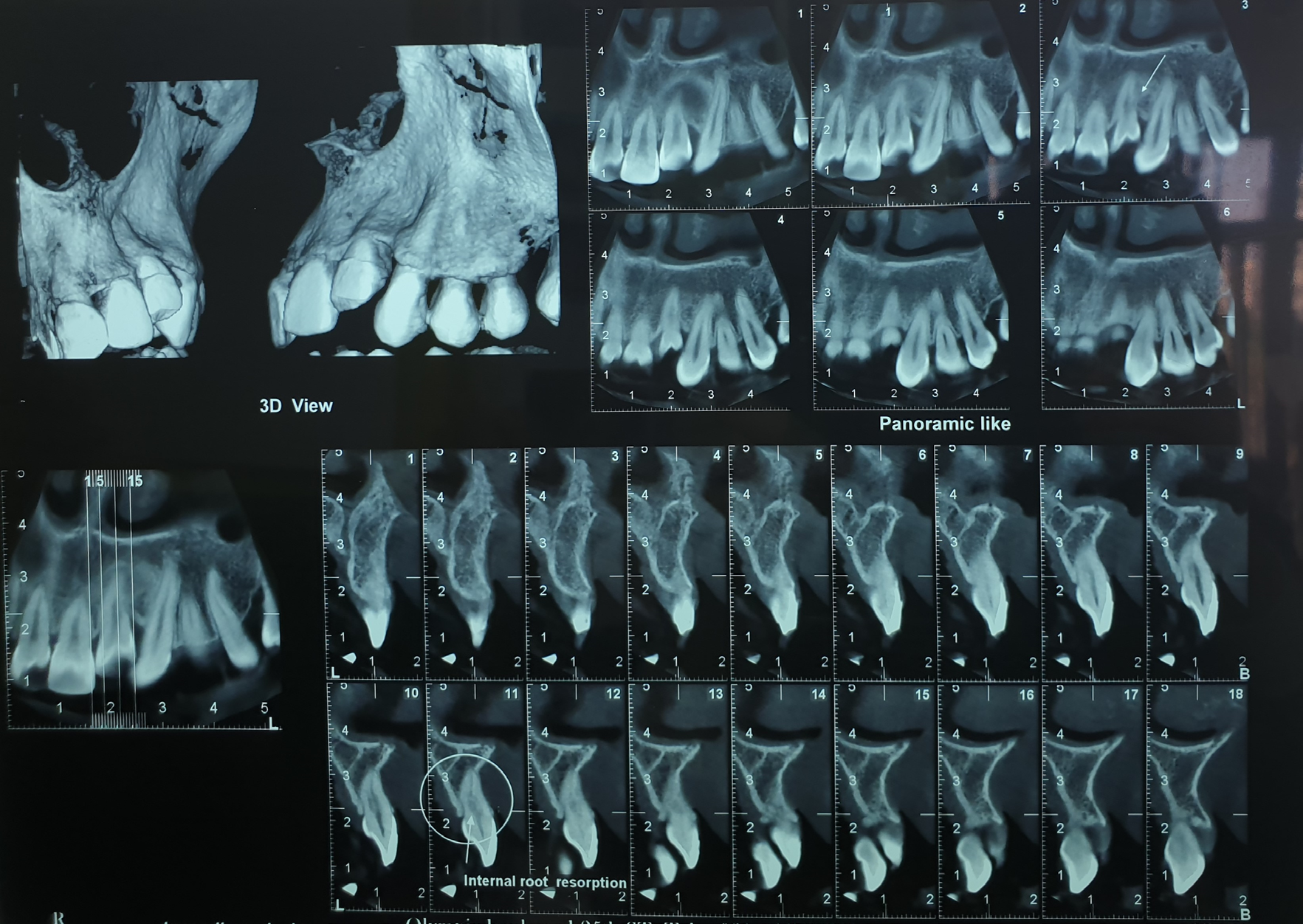
A CBCT with a small field of view was prepared for further investigation. It clearly revealed internal root resorption (IRR) of the left lateral incisor (Figure 1).
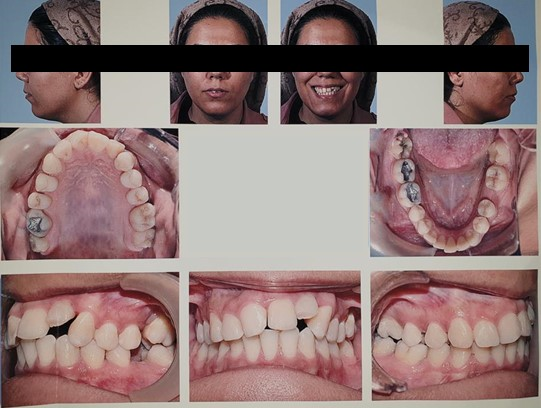
Clinical evaluation showed a convex profile with a relatively shallow mentolabial sulcus and increased height of lower face. A non-consonant smile arc and 3 mm shift of lower midline to right side were noted. Intraoral examination showed impaired dental system. Teeth number 3, 14, 19, and 29 were already extracted. Canine relationship was cl I in left and cl II in right side. Overjet was appropriate, while a remarkable 4 mm anterior open bite in left lateral incisor region was apparent (Figure 2).
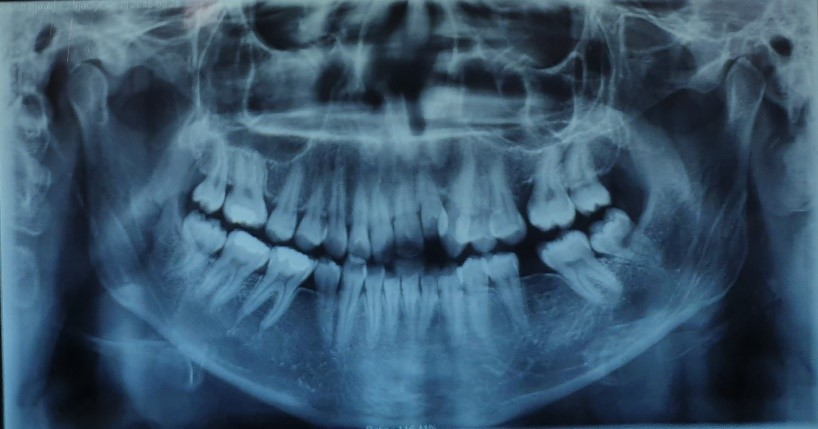
Cephalometric analysis revealed a class I anteroposterior skeletal relationship as well as long face tendency with counterclockwise rotation of maxilla (Figures 3 and 4). Cephalometric data are summarized in Table 1.
| Parameter | Patient value | Norm |
|---|---|---|
| SNA | 82.6 | 82±2 |
| SNB | 80.1 | 80±2 |
| ANB | 2.5 | 2±2 |
| wits | -1 | 0.82±2.1 |
| Facial angle | 84.5 | 82-95 |
| Basal angle | 38.3 | 27±4 |
| Saddle angle | 121.6 | 125±5 |
| Articular angle | 146.8 | 140±6 |
| Gonial angle | 129.7 | 128±7 |
| Sum of Bjork | 398.1 | 396±20 |
| SN-GoGn | 34.8 | 32±4 |
| FMA | 34.2 | 26±4.5 |
| IMPA | 97.5 | 90±5 |
| U1 to SN | 121 | 102-105 |
| U1 to FH | 124.8 | 111±5 |
| L1 to NB distance | 8.2 | 8.36±2.63 |
| U1 to NA distance | 8.4 | 9.258±3.67 |
| Interincisal angle | 103.5 | 135±5 |
Table 1: Cephalometric analysis data.

Treatment Objectives
The treatment objectives were to (1) endodontic treatment of maxillary left lateral incisor to prevent the progression of IRR (was performed based on endodontist consultation), (2) alignment of the other teeth and space opening for ankylosed tooth, (3) alignment and levelling of left lateral incisor, (4) levelling of gingival margins if needed, and (5) improvement of smile arc.
Treatment
Several treatment modalities have been suggested for patients with ankylosed anterior tooth as follows: 1. Tooth extraction and ridge augmentation for prosthetic tooth replacement
2. Decoranation and esthetic space maintenance 3. Tooth extraction and orthodontic space closure 4. Corticotomy in order to separate a bone block and allow rapid movement of the tooth followed by distraction osteogenesis 5. Surgical luxation of the ankylosed tooth to break the fusion between tooth and bone and immediate orthodontic force application to level the tooth In this case, since the patient’s growth was completed, decoronation was not applicable, and orthodontic space closure was also excluded as patient had CL I malocclusion. In addition, due to huge size and high gingival margin level of canine, substitution of canine for lateral was expected to cause esthetically unsatisfying results.
Because the ankylosed tooth did not undergo extensive root resorption, we considered the last two options which both required preliminary alignment of other teeth and space opening for lateral incisor. Since the patient was not eager to undergo aggressive procedures, and due to her preference for more economic options, we decided to try the less aggressive method, surgical luxation, first. The patient agreed that in case this method fails, she needs to undergo corticotomy and DO.
Treatment Progress
At first step, the patient was referred to department of endodontics, and endodontic treatment for prevention of progress in IRR was performed.
After root canal therapy, maxillary teeth were bonded with preadjusted 0.022 × 0.028 MBT Brackets. Alignment started with 0.014 inch NiTi archwire and progressed to 0.016 inch and 0.018 inch NiTi arch wires. The left lateral incisor (tooth number 10) was not engaged in the arch wires in this stage. After initial alignment was completed, NiTi compressed coil spring was used on 0.018-inch SS arch wire to open space for the left lateral incisor. After enough space was opened in upper arch, the surgical luxation was performed by an oral surgeon. A miniscrew (1.6mm × 8 mm) was inserted in alveolar process of lower arch between teeth 22 and 23.
Immediately after luxation, 1/4 light interarch elastic was used for traction between miniscrew and tooth 10. Patient was asked to use the elastic fulltime, and remove it just for eating and brushing. Elastic was replaced by the patient every 24 hours. The patient was visited every week for three weeks and was noticed to call us in case of abnormal pain, mobility, or bleeding. After the first week, the elastic was changed to 3/16 medium to apply a heavier force. In that appointment patient informed us that she has just realized that she is two months pregnant and she is willing to undergo a single jaw orthodontic treatment. We consulted with patient’s gynecologists, and based on her advises, there was no problem for continuing the treatment. In addition, patient was informed that in case posterior occlusion is disturbed, two jaw treatment would be inevitable. Eight weeks later, 0.014 inch NiTi overlay wire was engage to tooth 10, to produce continuous light force and elastic was continued engaging teeth 9, 10, 11 and the TAD (Figure 5).

Treatment Results
The anterior openbite was corrected with extrusion of left lateral incisor. The smile arc was significantly improved and the patient was satisfied with the results. Fixed retainer was applied between upper incisors to prevent re-intrusion of left lateral incisor.
Since orthodontic treatment for lower arch was not performed due to patient’s pregnancy and her desire, the lower midline and canine relationship remained uncorrected (Figure 6).

Periapical image of tooth 10 at the end of the treatment showed successful endodontic treatment with no evidence of increase root resorption (Figure 7).

Discussion
Traumatic injuries (especially severe luxation and avulsion injuries) have been accused as the primary cause of tooth ankylosis. However, other possible reasons exist. Since the maxillary incisors are highly accident prone, they could easily be ankylosed in different stages of development [13, 14]. Considering these teeth are located in the esthetic zone, it can turn to a more challenging problem affecting both esthetics and self-confidence. Several methods such as decoronation, prosthetic replacement, single tooth block corticotomy, distraction osteogenesis, and surgical luxation have been reported to address this problem [13, 15].
When ankylosis occurs, two main issues should be considered in treatment planning: whether the patient is growing [16], and how much of the root is involved with external root replacement [17].
When ankylosis occurs in growing patients, it causes progressive vertical alveolar discrepancy, so treatment should be aimed to reduce the need for ridge augmentation in adult life [18]. Decoronation has been suggested in children and adolescents to preserve alveolar ridge width, and apposition of bone on buried root which improves vertical aspect of ridge [19, 20]. However, when we encounter a tooth that has been ankylosed several years ago and vertical discrepancy is already evident, this approach is not efficient [10]. In this sitations, one solution is surgical luxation of the tooth and immediate orthodontic force application, provided the tooth have enough root length and has not been replaced by bone extensively. If successful, this method will have aesthetic results without the need for prosthetic treatment and related complications and costs [17]. It has been assumed that if ankylosed tooth is moved enough, it can break the fusion area, while periapical blood supply is maintained and the inflammatory reaction will generate new periodontal ligament [21]. In this case report we used surgical luxation followed by immediate traction with miniscrew assisted anchorage which provids three dimensional force vector control and versatility [22]. Since in this patient the vertical growth was completed, we levelled the tooth 10 with the adjacent teeth. In younger patients that vertical growth is remained, overcorrection of vertical position of ankylosed tooth is sensible [23].
One limitation of this approach is patient’s cooperation. If the tooth does not move immediately after luxation, it will be re-ankylosed during healing procedure, although in some cases the tooth becomes ankylosed again despite the orthodontic force is applied timely [24].
The second limitation of this method is miniscrew stability. Many factors cause miniscrew failure including Incorrect surgical procedure, Bone characteristics, Soft tissue thickness, Poor oral hygiene, and screw breakage. The length and shape of the miniscrew also influence the success rate [25].
Although several case reports have introduced osteotomy and distraction osteogenesis in ankylosis cases with vertical discrepancy, it was not the treatment of choice in this patient [15, 26, 27, 28]. This approach is more aggressive and costly with more challenging three dimensional control of bone block. However, it can be successfully used in cases with severe root resorption, or when root fracture is speculated.
Conclusion
Surgical luxation of ankylosed lateral incisor combined with TADs mechanic resulted in a successful single jaw orthodontic treatment. It improved patient`s smile arc and closed the anterior open bite using a less aggressive and less costly approach in comparison to alternative methods such as distraction osteogenesis, tooth extraction and ridge reconstruction for prosthetic replacement.
References
-
Chae JM, Paeng JY (2012) Orthodontic treatment of an ankylosed maxillary central incisor through single- tooth osteotomy by using interdental space regained from microimplant anchorage. Am J Orthod Dentofacial Orthop 141(2): e39-e51.
-
Proffit WR, Fields WH, Sarver DM (2007) Contemporary Orthodontics. St Louis: Mosby Co..
-
Patel S, Saberi N (2018) The ins and outs of root resorption. Br Dent J 224(9): 691-699.
-
Biederman W (1962) Etiology and treatment of tooth ankylosis. Am J Orthod 48(9): 670-684.
-
Susami T, Matsuzaki M, Ogihara Y, Sakiyama M, Takato T, et al. (2006) Segmental alveolar distraction for the correction of unilateral open-bite caused by multiple ankylosed teeth: a case report. J Orthod 33(3): 153-159.
-
Vd P, Primo L (2007) Development of Ankylosis in permanent incisors following delayed replantation and severe intrusion. Dent Traumatol 23(6): 390-391.
-
Peretz B, Absawi-Huri M, Bercovich R, Amir E (2013) Inter-relations between infraocclusion of primary mandibular molars, tipping of adjacent teeth, and alveolar bone height. Pediatr Dent 35(4): 325-328.
-
Lim WH, Kim HJ, Chun YS (2008) Treatment of ankylosed mandibular first permanent molar. Am J Orthod Dentofacial Orthop 133(1): 95-101.
-
Isaacson RJ, Strauss RA, Bridges-Poquis A, Peluso AR, Lindauer SJ (2001) Moving an ankylosed central incisor using orthodontics, surgery and distraction osteogenesis. Angle Orthod 71(5): 411-418.
-
Sapir S, Shapira J (2008) Decoronation for the management of an ankylosed young permanent tooth. Dent Traumatol 24(1): 131-135.
-
Mullally B, Blakely D, Burden D (1995) Ankylosis: an orthodontic problem with a restorative solution. Br Dent J 179(11): 426-429.
-
Razdolsky Y, El-Bialy TH, Dessner S, Buhler Jr JE (2004) Movement of ankylosed permanent teeth with a distraction device. J Clin Orthod 38(11): 612-620.
-
Mohadeb JVN, Somar M, He H (2016) Effectiveness of decoronation technique in the treatment of ankylosis: A systematic review. Dent Traumatol 32(4): 255-263.
-
Patel S, Ford TP (2007) Is the resorption external or internal? Dent Update 34(4): 218-229.
-
Tocolini DG, Silva PdO, Grabowski I, Carelli J, Morais ND, et al. (2019) Orthodontic Treatment of Ankylosed Maxillary Incisor through Osteogenic Distraction and Simplified Biomechanics. Case Rep Dent 2019: 8152793.
-
Campbell KM, Casas MJ, Kenny DJ (2005) Ankylosis of traumatized permanent incisors: pathogenesis and current approaches to diagnosis and management. J Can Dent Assoc 71(10): 763-768.
-
Takahashi T, Takagi T, Moriyama K (2005) Orthodontic treatment of a traumatically intruded tooth with ankylosis by traction after surgical luxation. Am J Orthod Dentofacial Orthop 127(2): 233-241.
-
Lin S, Schwarz-Arad D, Ashkenazi M (2013) Alveolar bone width preservation after decoronation of ankylosed anterior incisors. J Endod 39(12): 1542-1544.
-
Malmgren B (2013) Ridge preservation/decoronation. J Endod 35(2): 164-169.
-
Zilberman U, Zagury A (2015) Autotransplantation of a premolar to the maxillary anterior region in young children-how long should the donor root be? A case report. World J Stomato 4(4): 141-145.
-
Albers DD (1986) Ankylosis of teeth in the developing dentition. Quintessence Int 17(5): 303-308.
-
Aizenbud D, Hazan-Molina H, Cohen M, Rachmiel A (2012) Combined orthodontic temporary anchorage devices and surgical management of the alveolar ridge augmentation using distraction osteogenesis. J Oral Maxillofac Surg 70(8): 1815-1826.
-
Şenışık NE, Koçer G, Kaya BÜ (2014) Ankylosed maxillary incisor with severe root resorption treated with a single-tooth dento-osseous osteotomy, vertical alveolar distraction osteogenesis, and mini-implant anchorage. Am J Orthod Dentofacial Orthop 146(3): 371-384.
-
Turley PK, Crawford LB, Carrington KW (1987) Traumatically intruded teeth. Angle Orthod 57(3): 234- 244.
-
Maino BG, Pagin P, Di Blasio A (2012) Success of miniscrews used as anchorage for orthodontic treatment: analysis of different factors. Prog Orthod 13(3): 202-9.
-
Chang HY, Chang YL, Chen HL (2010) Treatment of a severely ankylosed central incisor and a missing lateral incisor by distraction osteogenesis and orthodontic treatment. Am J Orthod Dentofacial Orthop 138(6): 829- 38.
-
Ohkubo K, Susami T, Mori Y, Nagahama K, Takahashi N,et al. (2011) Treatment of ankylosed maxillary central incisors by single-tooth dento-osseous osteotomy and alveolar bone distraction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 111(5): 561-7.
-
Shahroudi AS, Golmohammadi S (2020) Miniscrew assisted single tooth distraction osteogenesis to align an ankylosed infraoccluded maxillary central incisor A case report. J Orthod 47(4): 345-53.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells