Complex Crown Fracture Presenting 5 Hours Post Trauma in a General Dental Practice
Paediatric dental trauma presentation is a common occurrence which dentists are faced with in a general dental practice setting. Most dental traumas are related to the anterior teeth and emergency care must be to a high standard when dealing with such incidences. A thorough and accurate diagnosis as well as a comprehensive treatment plan is essential. Furthermore, good communication for consent, giving explanations and providing treatment options is a prerequisite for clinical treatment. This case report describes a clinical case of complicated crown fractures of the UR1 and UL1 in a 10-year-old patient, where both incisors were directly pulp capped with Calcium Hydroxide and original fragments reattached. Following from this, four months later the UR1 attained another trauma and was treated elsewhere but re-presented with pain and infection. The UR1 was treated with root canal treatment while the UL1 remained vital and asymptomatic, till this date.
Introduction
Dental trauma is relatively common in paediatric patients with a prevalence of 11% for trauma to permanent teeth in children aged 6-18 years [1]. Furthermore, studies have shown that maxillary central incisors, particularly in children, are the most frequently affected teeth by trauma, with a 96% prevalence [2]. Several methods exist for managing complicated crown fractures, including direct pulp capping, partial pulpotomy, cervical pulpotomy and pulpectomy [3, 4]. Partial pulpotomy is the removal of inflamed coronal pulp while leaving the uninflamed underlying deeper pulpal tissue [5]. Partial pulpotomy was the chosen treatment method in this case.
The choice of material to directly cap the pulp has been much debated in recent years, between two main materials.
Calcium Hydroxide is a long-standing dental material and was the “gold standard” for decades for direct pulp capping [6]. It has a high pH which help to stimulate fibroblasts and has excellent antibacterial properties. It also promotes healing and repair of pulpal tissue, stops internal resorption in teeth and is generally inexpensive and easy to use [7]. Due to these qualities, Calcium Hydroxide can be sought as an ideal material for pulp capping. On the other hand, some disadvantages of Calcium Hydroxide include that it has increased risk of solubility and marginal leakage after one year of placement [8].
Mineral Trioxide Aggregate (MTA) is a more recently discovered direct pulp cap material, being made up from tricalcium silicate, dicalcium silicate, and tricalcium aluminate [9]. The key advantages of MTA are that it is biocompatible and has good ability to set even when there is lack of moisture control present. It is also reported to provide a good seal to the tooth structure [10]. Recent evidence also supports MTA in giving a higher clinical success rate compared to Calcium Hydroxide [11]. However, some drawbacks to consider before using MTA are that it has a prolonged setting time, is a lot more expensive and has a possible risk of tooth discoloration as compared to Calcium Hydroxide [12].
It is important to consider the benefits and limitations of these materials in the context of a general practice setting before their use. This case report describes the management, journey and follow-ups of traumatised mature teeth UR1 and UL1, with the diagnosis of complicated crown fractures.
Case Report
A 10-year-old patient attended our surgery at around 3pm in the afternoon. The child was accompanied by his parents and had sustained a football injury earlier that morning. The child had his broken tooth fragments which the parents had kept in dry tissue.
The medical history was checked and there was no systemic disease history. There were also no extra oral lacerations or bruises present. However, intra oral examination revealed complicated crown fractures of the UR1 and UL1. Both UR1 and UL1 had normal sensibility testing, normal percussion testing and no mobility.
Periapical radiographic examination (Radiograph 1) showed an intact periodontal ligament space, complete root formation and no root fracture for both teeth. There was no active bleeding however there was evident pulpal involvement of both central incisors which was clinically visible as pulpal exposures (Figures 1 & 2).

Radiograph 1: Initial periapical view, showing closed apicies, with no evident periapical pathology/radiolucent area.


Partial pulpotomy using a setting Calcium Hydroxide, Dycal® (Dentsply) was carried out on both incisors after local anaesthetic administration and placement of Optragate® (Ivolcar Vivadent) retraction isolation. <1mm pulpal tissue were gently removed by using a slow round head sterile bur, with saline wash. Minimal haemorrhage was controlled with sterile cotton pellets and saline. Shortly after pulpal bleeding stopped, Dycal® was placed (without any pressure) to cover the exposed parts of the pulpal area (Figure 3).

The decision to use Calcium Hydroxide rather than MTA was strongly influenced by the stock availability in the practice. One of the key factors which cannot be overlooked is we had to act fast to have better prognosis of the teeth. The cost of MTA, being 24 times more expensive per gram than its counterpart Calcium Hydroxide [7], with the possibility of tooth darkening with MTA [13] is a significant disadvantage considering the teeth are anterior, causing an aesthetic concern which may require further restorative treatment to address. Calcium Hydroxide is still a good quality pulp cap material and has shown favourable clinical outcomes over a long-term period [5] hence, it was used here.
The broken enamel fragments were washed and hydrated in a cup of saline for 20-25 minutes. Hydrating the tooth fragments in saline before reattachment has shown better fracture resistance in the longer term [14]. Both teeth and the fragments were acid etched, bonded and reattached to UR1 and UL1 using flowable composite, accordingly (Figure 4).

It was decided to stabilise the reattached fragments with a flexible splint palatally (Figure 5) for two weeks. This was important as it gave the patient confidence to use their anterior teeth. The patient was advised to have a soft diet for 2 weeks, avoid participation in contact sports, brush around the teeth using a soft toothbrush after every meal and use a chlorhexidine mouth rinse; providing has no allergies, as per the International Association for Dental Traumatology (IADT) guidelines. This will aid in healing of the traumatic injury and ensure stability of the reattached fragment [15].



Radiograph 2: Post-operative periapical view.
Parents were also informed to monitor the teeth for any signs of discolouration, pain, infection or swelling as this will indicate possible complications post the trauma and a need for root canal treatment [16] (Figure 6, Radiograph 2).
The patient’s follow-up after two weeks demonstrated good stability, with the ability to bite on the front teeth without any symptoms. Sensibility testing of both upper central incisors was performed, with no abnormal results noted. A review radiograph revealed no concerning periapical areas. The splint was removed, and teeth were polished accordingly.
Another follow-up visit was conducted one month later (Figure 7), showing good progress. A new periapical radiograph (Radiograph 3) showed no abnormalities or periapical areas. The pulp capping was still present and holding strong.

Radiograph 3: 1 month review periapical view.
After a period of four months, the patient came back with symptoms specifically related to the UR1, experiencing pain and tenderness to touch.
Upon further questioning and probing, it was discovered that the patient had sought emergency dental treatment elsewhere two weeks prior. The child had attained yet another dental trauma to the UR1 where the pulp cap had been breached.
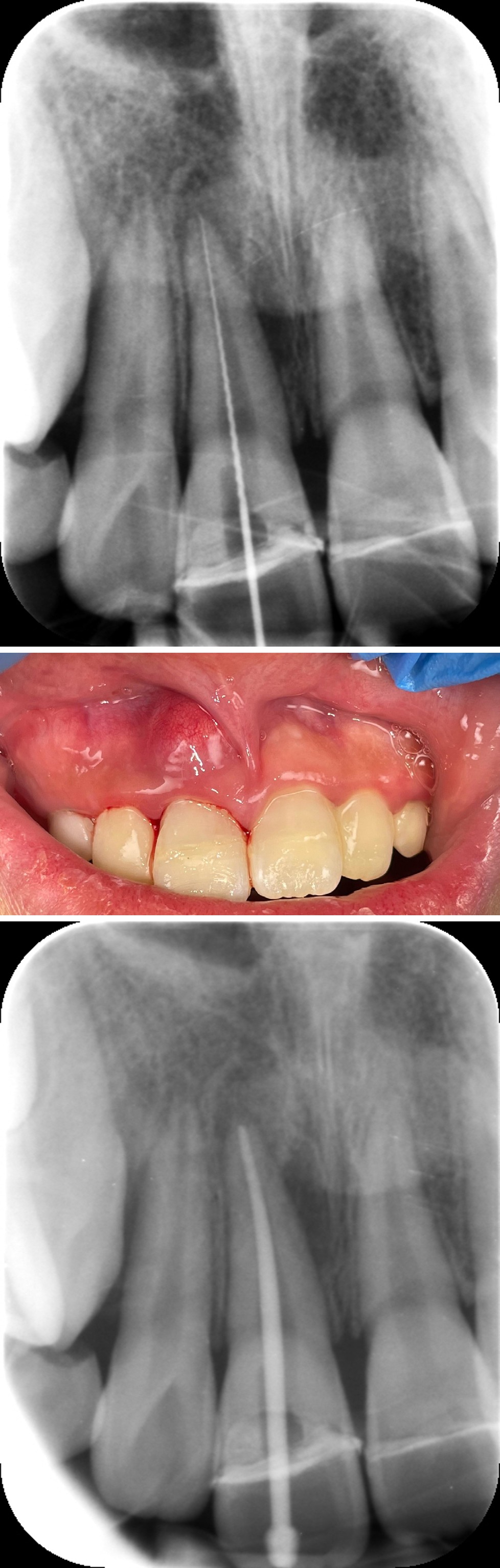
In the emergency treatment the UR1 fragment was reattached without addressing pulp cap. A new periapical radiograph showed a new periapical radiolucent area around UR1, and the original Calcium Hydroxide pulp cap appear to be breached. No abnormality was observed on the UL1 (Radiograph 4).
Radiograph 4: 4 months review periapical view, showing new periapical radiolucent area and break in pulp cap seal on UR1.
UR1 was non-responsive to Endofrost® (Roeko) and was Tender to Percussion (TTP), while UL1 responded normally and was not tender.
At this stage, after further discussion and treatment options given, both parents opted for a specialist treatment on the UR1, which would require a referral for root canal treatment to stabilise. Although it is too early to conclude the prognosis of UL1 and its vitality, the current results are promising.
They parents were fully informed of the potential waiting times of specialist referral, which could significantly impact the prognosis of the UR1. Teeth that have had traumatic injuries previously are at a higher risk of external inflammatory resorption [17]. This is when an inflammatory response is initiated within the periodontal ligament and characterised by a radiolucent area involving the periodontal ligament and adjacent bone showing loss of tooth substance [18]. External inflammatory resorption is caused by 2 factors: an infected root canal system and loss of cementum (for example, damage by trauma) [18]. External inflammatory resorption can aid towards periapical periodontitis [19] which is a local inflammatory response due to the presence of microorganisms within an infected root canal system [20].
Three months later (seven months since the original pulp cap breach), the patient with parents, returned to the dental clinic expressing disappointment in not having received a response from the referral pathway. Consequently, they made the decision to proceed root canal treatment with us in practice. Regrettably, during this time, the patient had developed a periapical abscess (Figure 8).
In light of this concerning development, a comprehensive discussion was undertaken with the parents, outlining the prognosis of the tooth and the diminished success rate associated with the presence of both a periapical area and the newly formed abscess lesion. Academic references indicate that such cases have a success rate ranging from 60- 70% [21].
After obtaining informed consent, an incise and drain procedure was performed, and the actual root canal treatment was postponed.
The tooth was isolated using a rubber dam (ColteneWhaledent, Alstatten, Switzerland) and an access cavity was drilled beneath the fragment reattachment line palatally, ensuring an optimal seal, which was further reinforced using a block-out gel as needed. To streamline the treatment process, it was decided to complete the treatment in a single visit; as supported by literature that: single or multi visit treatment regimen is not more effective than the other [22].
Radiograph 5: Working length view.
Radiograph 6: Master cone fit view.
Coronal flaring was completed initially, however the apex locator readings were inconclusive, so a working radiograph with size 10 k-file® was used to accurately determine the working length (Radiograph 5) before proceeding with the rest of the canal preparation. Utilising the WaveOne gold® primary - Red 025, 7% variable taper file, the canal was carefully shaped while employing continuous irrigation with sodium hypochlorite 3% Calasept® (Directa). Thorough canal cleansing was followed by drying. For the obturation phase, a WaveOne gold® Conform Fit GP -red- was employed to achieve a precise master cone fit (Radiograph 6), resulting in a satisfactory radiographic outcome. The final obturation was accomplished using a cold lateral compaction technique along with AH Plus Bioceramic® sealer, ensuring an optimal obturation result (Radiograph 7).

Radiograph 7: Post obturation view.
Finally, the access cavity on the UR1 was restored using a composite restoration (Radiograph 8). The UL1 remains responsive and vital when assessed 15 months on, the patient’s last visit, as well as complete healing of the radiolucent area on UR1 (Figure 9, Radiograph 9).
Radiograph 8: Final post-operative view.
Radiograph 9: 7 months post-operative view, showing complete healing of the periapical area associated with UR1 and clear periapical area on UL1.
Conclusion
For a successful pulp cap, it is essential that a good seal is present to aid healing of pulpal tissue. This is evident within this case report as the UL1 pulp cap remained successful because there was no disruption to the Calcium Hydroxide seal. However, the UR1 became symptomatic following a second trauma injury, which resulted in a breach in the pulp cap and subsequently in bacterial ingress causing a periapical abscess. In general dental practice, the use of Calcium Hydroxide can give favourable results however, the sufficiency of the pulp cap seal is crucial to clinical success.
Reflection
Considering that Calcium Hydroxide pulp capping is a traditional procedure and readily available in general dental practices, unlike alternative materials such as MTA, it was the chosen material in this case. Although literature reports an 80% success rate in preserving pulp vitality with Calcium Hydroxide, this is contingent upon accurate diagnosis and achieving an optimal seal. On the other hand, recent studies have demonstrated a 96% success rate with MTA [21], indicating its superiority as a medicament for pulp capping compared to Calcium Hydroxide [22]. Though MTA has an increased success rate when compared to Calcium Hydroxide, it is not readily available in general dental practices due to being more expensive. Nevertheless, it is essential to acknowledge this information and general dental practitioners should consider incorporating MTA into the surgical armamentarium in future.
Authors Contributions
HA carried out all clinical aspects and drafted the manuscript. BP and ST reviewed and helped with the write up process. The final product was refined by HA through several rounds of discussion.
References
-
Kaba AD, Maréchaux SC (1989) A fourteen-year follow- up study of traumatic injuries to the permanent dentition. ASDC J Dent Child 56(6): 417-425.
-
Andreasen JO, Bakland LK, Matras RC, Andreasen FM (2006) Traumatic intrusion of permanent teeth. Part 1. An epidemiological study of 216 intruded permanent teeth. Dent Traumatol 22(2): 83-89.
-
Raut AW, Mantri V, Shambharkar VI, Mishra M (2018) Management of Complicated Crown Fracture by Reattachment Using Fiber Post: Minimal Intervention Approach. J Nat Sci Biol Med 9(1): 93-96.
-
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K (2008) Outcome of primary root canal treatment: systematic review of the literature -- Part 2. Influence of clinical factors. Int Endod J 41(1): 6-31.
-
Cvek M (1978) A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. J Endod 4(8): 232-237.
-
Accorinte MLR, Loguercio AD, Reis A, Muench A, de Araújo VC (2005) Response of human pulp capped with a bonding agent after bleeding control with hemostatic agents. Oper Dent 30(2): 147-155.
-
Hilton TJ (2009) Keys to Clinical Success with Pulp Capping: A Review of the Literature. Operative Dentistry 34(5): 615-625.
-
Ba Hattab R, Al-Jamie M, Aldreib H, Alessa L, Alonazi M (2016) Calcium Hydroxide in Endodontics: An Overview. Open Journal of Stomatology 6(12): 274-289.
-
Camilleri J (2008) Characterization of hydration products of mineral trioxide aggregate. Int Endod J 41(5): 408- 417.
-
Ferk Luketić S, Malcić A, Jukić S, Anić I, Segović S, Kalenić S (2008) Coronal microleakage of two root-end filling materials using a polymicrobial marker. J Endod 34(2): 201-203.
-
Zhu C, Ju B, Ni R (2015) Clinical outcome of direct pulp capping with MTA or calcium hydroxide: a systematic review and meta-analysis. Int J Clin Exp Med 8(10): 17055-17060.
-
Mineral Trioxide Aggregate-an overview.
-
Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS (2003) Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: a preliminary report. Int Endod J 36(3): 225-235.
-
Suresh M, Mallikarjun SB, Babu G, Zareena MA (2020) Fracture Resistance of Reattached Hydrated Fragment of Fractured Incisors. Int J Clin Pediatr Dent 13(5): 476- 480.
-
Robinson A (2013) Dental Trauma Guidelines.
-
Practitioners’ Toolkit.
-
Zaid Al-Momani, Peter J Nixon (2013) Internal and external root resorption: aetiology, diagnosis and treatment options. Restorative Dentistry 40(2): 102- 112.
-
Abbott P (2016) Prevention and management of external inflammatory resorption following trauma to teeth. Aust Dent J 61(1): 82-94.
-
Fernandes M, de Ataide I, Wagle R (2013) Tooth resorption part II - external resorption: Case series. J Conserv Dent 16(2): 180.
-
Abbott PV (2004) Classification, diagnosis and clinical manifestations of apical periodontitis. Endodontic Topics 8(1): 36-54.
-
Roudsari RV, Jawad S, Taylor C, Darcey J, Qualtrough A (2016) Modern endodontic principles part 8: the future of endodontics. Dent Update 43(5): 430-441.
-
Hilton TJ, Ferracane JL, Mancl L, Baltuck C, Barnes C, et al. (2013) Comparison of CaOH with MTA for Direct Pulp Capping. J Dent Res 92(7): 16-22.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells