Perceptions about the Relationship between Oral Health and Digestion: A Qualitative Study
Tooth loss can be closely associated with malnutrition and the risk of systemic diseases. This study evaluated the perceptions of patients with gastrointestinal diseases about the importance of teeth and their relationship with gastroenterological conditions. A total of 14 patients with gastrointestinal diseases were included to answer a script with 12 questions (qualitative study). The responses were transcribed and analyzed using Fernando Lefèvre’s methodological approach: “Discourse of the collective subject”. 71.42% (n= 9) of the volunteers felt some discomfort/pain when eating caused by problems with their mouth/prosthesis, and 28.57% (n= 3) responded that they were unable to eat any food they wanted due to problems with their mouth or limbs Teeth. The results show that only 28.57% (n=3) associate the loss of teeth with worsening chewing and digestion capacity. It can be concluded that most patients do not understand the association between tooth loss and the digestion process, causing gastroenterological alterations.
Introduction
Tooth loss cannot be considered just a consequence of poor oral health; it is also a reflection of socioeconomic factors and/or levels of health education [1]. In addition to being associated with low intake of nutritious foods, edentulous patients report problems and difficulties in chewing [2, 3, 4, 5, 6, 7, 8].
Nutritionists reinforce the concept that digestion starts in the mouth [9]. The nutrition of patients with impaired oral health status can be severely impacted, leading to important systemic changes [10]. Tooth loss can be closely associated with malnutrition and the risk of systemic diseases, resulting in a decline in oral health and chewing deficiencies [11, 12, 13]. When comparing fruit intakes in edentulous patients with those who received some natural teeth, it is observed that they consumed apples and pears less frequently than dentate ones [5, 14]. Concerning biochemical analytes found in fruits and vegetables, significant differences were found for plasma retinol, alpha-tocopherol, and vitamin C between the edentulous and the dentate in a national survey of older adults [15, 16].
The gastroenterology conditions of patients with missing teeth can lead to oral manifestations [17, 18]. In some inflammatory bowel diseases, non-specific oral manifestations include thrush, pyostomatitis vegetans, and diffuse gingival, buccal, or labial edema, which may precede intestinal symptoms [18]. As well as other negative impacts such as functional dyspepsia [19]. In addition, edentulous people with low masticatory capacity have lower plasma levels of vitamin C, which decreases antioxidant activity [20].
Although these issues are straightforward for health professionals, this reality differs for patients. The relationships between dental status, chewing behavior, eating attitudes, and nutrition are complex, and studies are necessary to understand better the impact of tooth loss on these patients’ eating and nutritional behavior [21]. Nowadays, few studies have investigated the association between tooth loss, nutritional status, and digestion; the knowledge of patients with gastrointestinal diseases about the importance of teeth and their relationship with oral health and the digestion process needs to be clarified. The aim of this study was to understand the knowledge about the relationship between oral health and digestion of patients with digestive system involvement.
Material and Methods
Study Design, Ethical Issues, and Eligibility Criteria
This study comprises individuals who affected with a gastrointestinal disease. The study was elaborated on the Consolidated Criteria for Reporting Qualitative Research (COREQ; Tong, Sainsbury & Craig, 2007) and was approved by the Institutional Ethics Committe (No: 3.508.352) All the participant’s identity remained anonymous in accordance with the Declaration of Helsinki.
A qualitative approach was used to search for a greater understanding of the issues that permeate the feelings and perceptions of patients about the relationship between oral health and digestion, further capturing the subjective experiences of individuals about their well-being. The focus was identification, in-depth description, and generation of explanations, in addition to seeking the meaning and intentionality of acts contemplating the purpose of this work.
Patients affected by gastrointestinal diseases affected by gastrointestinal diseases, being in medical care by the Clinical Hospital – Federal University of Minas Gerais Gastroenterology Service were included in this study. Exclusion criteria were cognitive impairment or the inability to understand. We offered no economic incentives to the participants, and none of the patients contacted refused to participate.
Interview Procedures
The 14 participants were asked to answer a script with 12 questions in order to identify the doubts, knowledge, and perceptions of the studied population about the importance of teeth and/or dental prostheses and their relationship with the digestive process.
Patient Interview Script a) About clinical aspects of teeth and prosthesis:
- Do you have any teeth present in your mouth? If not, do you know which and how many teeth are missing?
- If you currently use a prosthesis, do you know how to inform the type? Is it a fixed or removable prosthesis? Partial or total? b) On self-perception of discomfort or oral health problems
- Do you have any complaints about your oral health?
- Do you feel any discomfort/pain in eating due to problems with your mouth/dentures?
- Do you currently have any problems with your teeth (such as tooth mobility, decay, sensitivity) or gums? c) About the use of prosthesis
- If you lost any teeth, do you think it is essential to look for a dentist to have some dental prosthesis?
- If you use a prosthesis, is it old? How long have you been using this prosthesis? Do you think your prosthesis has retention problems (fixation)? d) About diet and chewing and your oral health
- Has your diet worsened because of problems with your mouth/dentures?
- If you have lost any teeth, do you think this loss has worsened your ability to chew or digest?
- Are you unable to eat any food you would like to eat? If yes, for what reason? Are there any problems related to oral health or other organs of the digestive system? e) Perceptions about the digestive system and oral health
- Do you think there is a relationship between your chewing and your digestive system?
- Do you think you can break the food into pieces small enough to swallow? If not, do you think this could cause any problems during the digestion of these foods?
The script was applied in the format of video interviews. A strategy was used to collect the data. It was conducted by just one interviewer who had not been directly involved in the treatment to reduce bias in the participant’s discourse.
The interviews were carried out individually and in a reserved place to minimize any discomfort to the volunteer. The interviewer read the questions with no time limit for answers.
Subsequently, the same researcher heard and transcribed the interviews verbatim in a Microsoft Word file. In order to protect the identity of the participants, original names were replaced by fictitious names. An analysis of these data was carried out using the methodological approach of Fernando Lefèvre [22]. In this approach based on the theory of social representations, called by the author “Collective subject discourse,” the analysis is done by grouping individual
| Percentage | ||
|---|---|---|
| Sex | Male | 21.43% |
| Sex | Female | 78.57% |
| Age | 19-29 | 14.28% |
| Age | 30-40 | 14.28% |
| Age | 41-51 | 21.42% |
| Age | 52-62 | 28.57% |
| Age | 63-73 | 14.28% |
| Age | 74-84 | 7.14% |
| Pathology | Erosive Esophagitis | 7.14% |
| Pathology | Esophageal Center | 14.28% |
| Pathology | Chagasic Megaesophagus | 14.28% |
| Pathology | Crohn’s Disease | 35.71% |
| Pathology | Oral and Stomach Cancer | 7.14% |
| Pathology | Bariatric Surgery | 7.14% |
| Pathology | Diverticulitis | 7.14% |
| Pathology | Leiomyoma | 7.14% |
Table 1: Medical characteristics of patients in the select study.
discourses with some similarity of ideas, thus forming a collective subject with social opinions. In this way, each answer was analyzed in detail, and the most relevant contents were selected, contemplating quantitative aspects.
Results
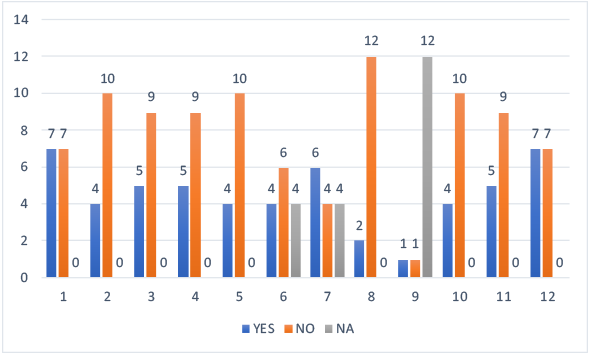
The 14 patients participated in the research, with a mean age of 49.1 years, ranging from a minimum of 19 to a maximum of 81 years; 11 were women and 3 were men (Table 1). The data obtained were synthesized in a table, in order to identify the main responses of the study participants (Figure 1).
Self-Perception of Oral Health and the Need for Treatment
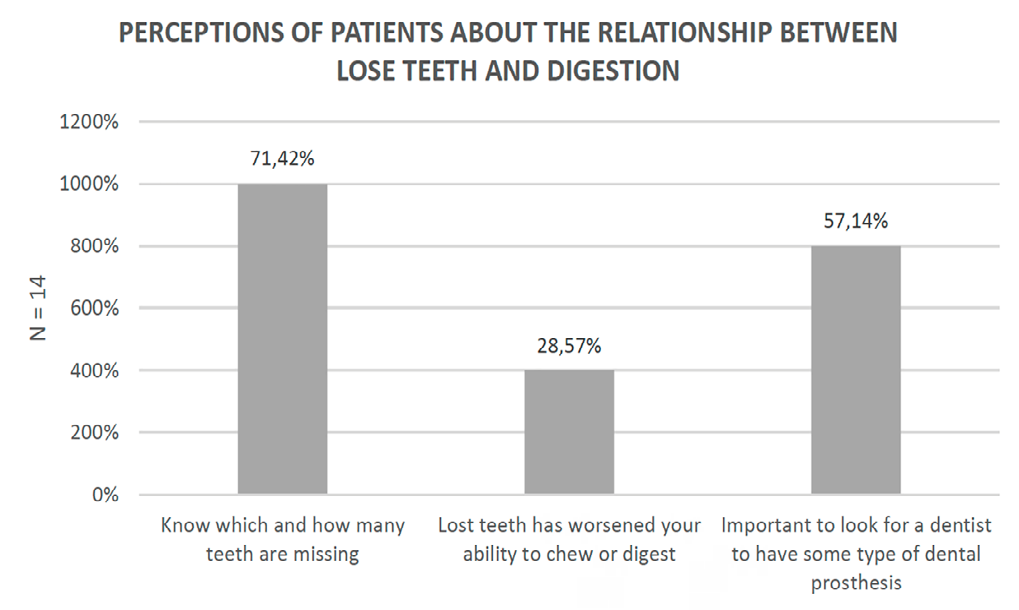
In this study, 71.42% (n= 9) of respondents did not have all their teeth in their mouths. 28.57% (n= 3) answered that lost teeth worsened the ability of chewing capacity or digestion, and 57.14% (n= 7) do not think it is essential to look for a dentist when you lose a tooth to have some dental prosthesis (Figure 2).
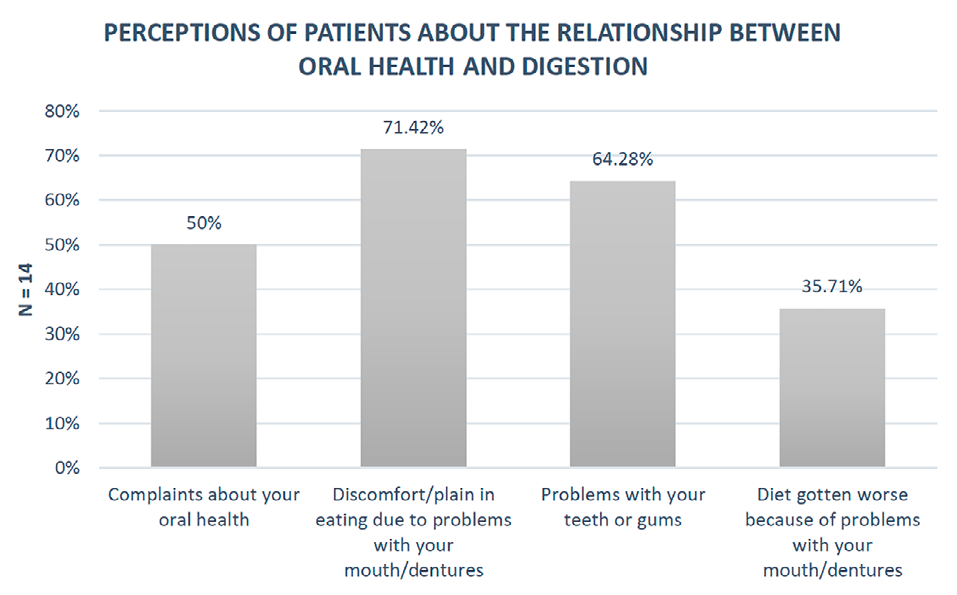
Figure 2: Patient responses related to: Do you have any teeth present in your mouth? If not, do you know which and how many teeth are missing? If you have lost any teeth, do you think this loss has worsened your ability to chew or digest? If you lost any teeth, do you think it’s important to look for a dentist to have some type of dental prosthesis?
Participants were asked if they lost any teeth and if they thought this loss worsened their oral health or digestion capacity:
“Oh, when I had my teeth, they all rotted, then it was worse to chew, right. Then later I went and sorted them all out and put the prostheses to eat better” (Mário);
“No, like normal. Good tooth” (Ana);
“No, because it has been a long time now because we used to go to the dentist in the past, and they ransacked everything. Formerly, the relief was to grind, and I started grinding my teeth when I was 18 years old; then, I gritted them all because I had some that hurt a lot. Then I said I would not feel it anymore; then the pain would start, I would pull it out instead of treating it; if it were today, there is good treatment, and that is it?” (Francisco).
Self-Perception of Feeding/Chewing/Digestion Difficulties due to Oral Health Condition
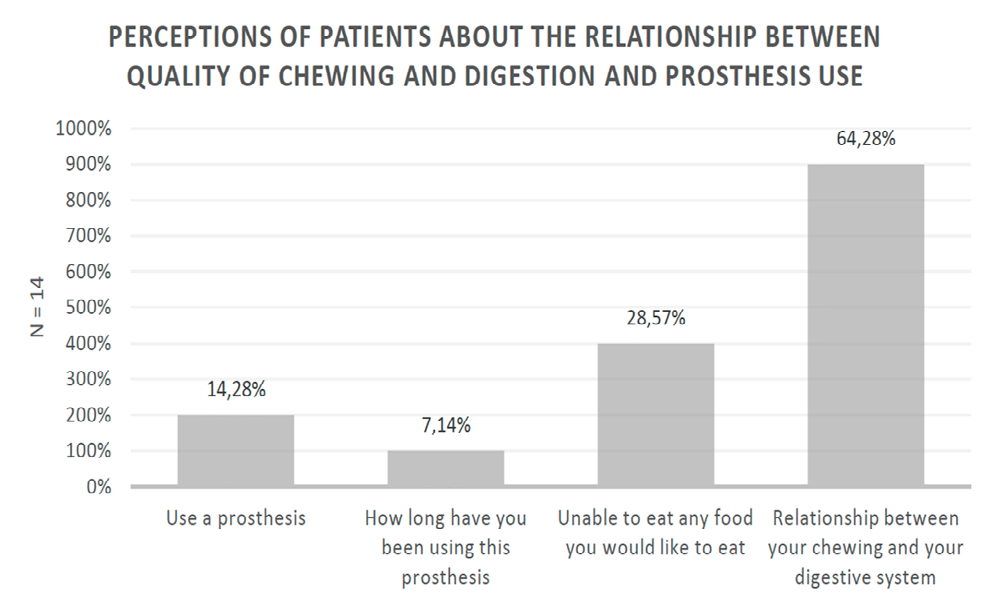
The results showed that 50% (n= 7) of respondents had any complaints about oral health, and 71.42% (n= 9) felt any discomfort/pain when eating due to problems with the mouth/prosthesis. 64.28% (n= 8) reported that they had no problems with their teeth or gums, and only 35.71% (n= 4) reported that there was a worsening in eating caused by mouth/prosthesis problems (Figure 3). Only 14.28% (n= 2) of respondents currently use some prostheses. Moreover, when asked about the state of the prosthesis retention, only 7.14% (n= 1) responded that they have problems. When asked if they could break the food into pieces small enough to be able to swallow, 50% answered that it was not possible. However, many of these volunteers lacked the posterior teeth and reported that they could chew correctly only with the anterior teeth.
Knowledge of the Relationship between Oral Health and Digestion
The results demonstrate that 28.57% (n= 3) answered that they could not eat any food they would like because of problems with their mouth or teeth. Regarding the relationship between chewing and the digestive system, 64.28% (n= 8) of patients answered that they thought there was no relationship between them (Figure 4).
When asked if they believe there is a relationship between their oral health and their digestive system, the answers found were:
“I do not think so; we chew depending, normal. I do not think I cheat, for me, I do not cheat at all. As you go, you will get used to it, not having those teeth” (Ana); “Of course, there is. I believe in many factors. First, when I return to feeding, my tooth will be essential because the more I have processed, chewed, and crushed the food, the better it is. For me, chewing is intrinsic to the process because the more torn the food is, the better it is for me because of the stomach and intestine. By the way, I feed baby food processed in a blender today. So, of course, there is a direct and proportional link as well” (Marina);
“If I eat something harder like that, it attacks the esophagus, then the food would come back a lot, you know, then I could not” (Mário); “There is a reason if the surgeon ordered it to be done, right? So must have. But I never thought the surgeon would talk to me before” (Francisco);
“Oh, I do not think so, because I chew normally, I go to the normal bathroom...” (Fátima);
“Oh, I do not think there is, because if it was like that I would feel burning, right, I do not feel anything” (Alice); “There is a lot” (Juliana);
“Oh yes, there is, because even our intestines have difficulty functioning, right. Sometimes we get stuck bowels, it is difficult...” (Rosane).
Discussion
This study exclusively examined the association between tooth loss and gastroenterology conditions among Brazilian adults aged 19-81 years. Oral health may also play a role in maintaining robust motility in the digestive tract by enhancing physiological gastric motion. In addition to this study demonstrating the relationship between chewing and the gastroenterology conditions, other studies point to the relationship between tooth loss and other systemic changes [13]. The associations between tooth loss and/or periodontal disease and cardiovascular disease were reported, too [16]. It was verified that edentulous persons (with or without prostheses) have more difficulty eating fruit, reflecting lower citrus fruit consumption and, therefore, lower vitamin C levels [16]. Low vitamin C levels are associated with cardiovascular disease [16]. The levels of biochemical analyte for nutrients found in fruits and vegetables were statistically significantly lower among denture-wearers. The serum beta carotene level among users of dentures was 1.7 times lower than that of fully dentate users [5, 23, 24]. However, this study shows that only 28.57% responded that tooth loss worsened their ability to chew or digest. The majority of patients interviewed are unaware of the association between tooth loss and gastroenterology conditions, demonstrating that they are unaware of the need to seek a dentist after tooth loss.
Okamoto, et al. [20] related that the maximum occlusal force decreased significantly with the number of teeth, consequently affecting the particle size. The comminution of food particles and their size affects gastric emptying time [25]. The delayed passage of inadequately chewed and larger-sized food particles through the stomach prolongs the period of gastric digestion with potentially detrimental consequences for the gastric mucosa. Thus, the altered gastric motor function shown by patients with decreased masticatory performance could be a possible cause of non- ulcerative functional dyspepsia [25]. On the other hand, it was shown that patients with impaired dental status produced a food bolus with a larger particle size than fully dentate patients. The solutions for compensating for missing teeth and restoring chewing function imply economic resources unavailable for most obese patients. The alternative to efficient mastication is artificial food comminution [21]. This study demonstrated that 71.42% felt any discomfort/pain when eating due to problems with the mouth/prosthesis.
Prosthetic rehabilitation was observed as the greatest need in patients undergoing bariatric surgery [17]. The replacement of lost dental elements is essential to minimize the postoperative side effects of changes in the digestive process, and it can be seen that many individuals are unaware of this relationship [17]. Obese subjects with impaired dental status could not produce a food bolus with the same particle size distribution as the fully dentate patients [21]. They could also not adapt their chewing activity to the food texture, and their mastication could have been more efficient [21]. Although only 28.57% of those interviewed in our study reported that tooth loss interferes with their chewing, it is possible to show that tooth loss directly interferes with food digestion. These findings corroborate those verified in this study since 64.28% believed there is no relationship between digestion and teeth.
The result found in our study can be explained by the patient’s lack of knowledge regarding the individual function of the teeth; 67.1% of patients reported that the missing teeth were posterior. Most patients mistakenly believe that the anterior teeth can grind food, justifying the lack of knowledge regarding the function of each tooth. It is essential to clarify that the absence of dental elements, especially the posterior ones, can generate overload and damage to other digestive system organs.
Many studies have qualitative methodology on this relationship between tooth loss and oral health-related quality of life [23, 24]. However, to our knowledge, this is the first qualitative study to investigate the experiences and perceptions of patients with gastrointestinal diseases about the importance of oral health and their relationship with the digestion process.
Oral health reflects the endpoint of a lifetime of dental disease and the individual’s history of (or absence of) dental treatment. Oral diseases are a significant global public health problem, having both high prevalence and significant negative impacts on individuals, communities, and society. In 2010, 158 million people, or 2.3% of the global population, were utterly edentulous (no natural teeth) [26]. Furthermore, tooth loss causes disorder in the quality of life of the individual, mainly when it affects their well-being, appearance, and nutritional status [27].
However, data on the population’s understanding of the relationship between tooth loss and the digestive process and the importance of oral rehabilitation for patients with gastrointestinal diseases are still scarce. The qualitative approach allowed an in-depth assessment of the participants. It revealed that most of them did not perceive a worsening in chewing and involvement of the digestive system after some tooth loss.
Most survey respondents (64%) responded that they believed there was no relationship between oral health and the gastroenterology conditions. In the meantime, dentists, doctors, nutritionists, and other health professionals must explain the critical relationship between mastication and the digestive process and guide the necessary oral health care. The relationships between dental status, chewing behavior, feeding attitudes, and nutrition are complex, and further studies are required to understand better the impact of chewing and the digestion process. Studies are cross- sectional, preventing definitive statements about the order of effects. We are, therefore, currently performing further prospective qualitative studies.
Participants needed to learn about the association between mastication and the gastroenterology conditions.
In addition, it is essential to report that most participants report tooth loss and believe it is unnecessary to look for a dental professional to rehabilitate. Most patients do not understand the importance of dental elements or a well- adapted prosthesis for good chewing and digestion, and it is necessary to think of strategies to clarify this population.
References
-
Souza JGS, Souza SE, Sampaio AA, Silveira MF, Ferreira EF, et al. (2016) Autopercepção da necessidade de prótese dentária total entre idosos brasileiros desdentados. Cienc Saude Colet 21(11): 3407-3415.
-
De Marchi RJ, Hugo FN, Padilha DMP, Hilgert JB, Machado DB, et al. (2011) Edentulism, use of dentures and consumption of fruit and vegetables in south Brazilian community-dwelling elderly. J Oral Rehabil 38(7): 533- 540.
-
Hutton B, Feine J, Morais J (2002) Is there an association between edentulism and nutritional state? J Can Dent Assoc 68(3): 182-187.
-
Parker ML, Thornton-Evans G, Wei L, Griffin SO (2020) Prevalence of and Changes in Tooth Loss Among Adults Aged ≥50 Years with Selected Chronic Conditions-United States, 1999–2004 and 2011–2016. MMWR Morb Mortal Wkly Rep 69(21): 641-646.
-
Nowjack-Raymer RE, Sheiham A (2003) Association of edentulism and diet and nutrition in US adults. J Dent Res 82(2): 123-126.
-
Ettinger RL (1998) Changing dietary patterns with changing dentition: How do people cope? Spec Care Dent 18(1): 33-39.
-
Slade GD, Spencer AJ, Locker D, Hunt RJ, Strauss RP, et al. (1996) Variations in the social impact of oral conditions among older adults in South Australia, Ontario, and North Carolina. J Dent Res 75(7): 1439-1450.
-
Locker D (1992) The burden of oral disorders in a population of older adults. Community Dent Health 9(2): 109-124.
-
Montenegro FLB, Marchini L, Brunetti RF, Manetta CE (2007) A importância do bom funcionamento do sistema mastigatório para o processo digestivo dos idosos. Kairós Gerontol 10(2): 245-257.
-
Kossioni AE (2018) The association of poor oral health parameters with malnutrition in older adults: A review considering the potential implications for cognitive impairment. Nutrients 10(11): 1709.
-
Felton DA (2016) Complete Edentulism and Comorbid Diseases: An Update. J Prosthodont 25(1): 5-20.
-
Müller F, Shimazaki Y, Kahabuka F, Schimmel M (2017) Oral health for an ageing population: the importance of a natural dentition in older adults. Int Dent J 67(Suppl 2): 7-13.
-
Kimura Y, Nomura M, Sawada Y, Muraoka N, Kohno N, et al. (2006) Evaluation of the effects of mastication and swallowing on gastric motility using electrogastrography. J Med Investig 53(3-4): 229-237.
-
Halling A, Bengtsson C, Lenner RA (1988) Diet in relation to number of remaining teeth in a population of middle- aged women in Gothenburg, Sweden. Swed Dent J 12(1- 2): 39-45.
-
Sheiham A, Steele JG, Marcenes W, Lowe C, Finch S, et al. (2001) The relationship among dental status, nutrient intake, and nutritional status in older people. J Dent Res 80(2): 408-413.
-
Lowe G, Woodward M, Rumley A, Morrison C, Tunstall- Pedoe H, et al. (2003) Total tooth loss and prevalent cardiovascular disease in men and women: Possible roles of citrus fruit consumption, vitamin C, and inflammatory and thrombotic variables. J Clin Epidemiol 56(7): 694- 700.
-
Silva ME de S e, Villaça ÊL, Magalhães CS de, Ferreira EF (2010) Impact of tooth loss in quality of life. Cienc Saude Colet 15(3):841-850.
-
Lourenço SV, Hussein TP, Bologna SB, Sipahi AM, Nico MM (2010) Oral manifestations of inflammatory bowel disease: A review based on the observation of six cases. J Eur Acad Dermatol Venereol 24(2): 204-207.
-
Monteiro MP, Carneiro FP, Felipe N de AP, Motta AR (2005) Mastigação e dispepsia funcional: um novo campo de atuação. Rev CEFAC 7(3): 340-347.
-
Okamoto N, Amano N, Nakamura T, Yanagi M (2019) Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: A cross-sectional study. BMC Oral Health 19(1): 110.
-
Godlewski AE, Veyrune JL, Nicolas E, Ciangura CA, Chaussain CC, et al. (2011) Effect of dental status on changes in mastication in patients with obesity following bariatric surgery. PLoS One 6(7): e22324.
-
Lefèvre F, Lefèvre AMC, Teixeira JJV (2000) The discourse of the collective subject: a new methodological approach in qualitative research. 1st (Edn.), Caxias do Sul: EDUCS.
-
Matthias RE, Atchison KA, Lubben JE, Jong FD, Schweitzer SO (1995) Factors Affecting Self‐ratings of Oral Health. J Public Health Dent 55(4): 197-204.
-
Locker D (1997) Clinical correlates of changes in self- perceived oral health in older adults. Community Dent Oral Epidemiol 25(3): 199-203.
-
Carretero D, Sánchez-Ayala A, Rodriguez A, Lagravere MO, Gonçalves TMSV, et al. (2011) Relationship between non-ulcerative functional dyspepsia, occlusal pairs and masticatory performance in partially edentulous elderly persons. Gerodontology 28(4): 296-301.
-
Peres MA, Macpherson LMD, Weyant RJ, Daly B, Venturelli R, et al. (2019) Oral diseases: a global public health challenge. Lancet 394(10194): 249-260.
-
Saintrain MVDL, De Souza EHA (2012) Impact of tooth loss on the quality of life. Gerodontology 29(2): e632- 636.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells