Analgesic Efficacy of Selective COX -2 Inhibitors in Post Endodontic Pain: A Systematic Review
Background: Endodontic treatment is considered a harrowing experience for patients in dental practice. COX-2 is a prime agent in inflammation and cell growth due to its relation with pro- inflammatory cytokines. Non -steroidal anti-inflammatory drugs are the most suited for treatment of post endodontic pain owing to their anti-inflammatory properties with the avoidance of cumbersome side effects such as nausea, vomiting, and respiratory problems associated with opioids. Aim: To assess the clinical efficacy of selective COX -2 inhibitors in comparison with other analgesics for managing postendodontic pain. Methods: This is an updated systematic review of studies between 2000 and 2023. Google Scholar, Web of science, Cochrane and PubMed databases were used to explore studies regarding our subject. The keywords included “selective COX-2 inhibitors; selective non- steroidal anti-inflammatory drug; endodontic pain; meloxicam; etoricoxib; metabolic complications” and were used in various combinations. In addition, original research reporting the clinical efficacy of selective COX -2 inhibitors in managing endodontic pain was evaluated. Full-text publications served as the inclusion criterion. Results: Among 100 articles were obtained, only nine met the inclusion criteria. All the studies were double-blinded randomized clinical trials. The study population was comprised of 1645 patients with endodontic pain. Conclusion: Selective COX -2 Inhibitors was an effective choice in managing endodontic pain. Celebrex was more effective than Celecoxib in relieving post-endodontic pain. When comparing Ibuprofen and Celecoxib, both were equally effective in relieving post-endodontic pain. Celecoxib was more effective than Naproxen in treating post-endodontic pain with minor gastrointestinal effects. Furthermore, etoricoxib considerably reduces post-endodontic pain with a single dosage.
Introduction
While pulpectomy removes endodontic pain, post- endodontic pain and discomfort are quite frequent endodontic side effects, affecting 25% to 40% of all endodontic patients [1]. The discomfort is partly hypothesized to be caused by the endodontic instrumentation’s periapical inflammatory reaction. Pre-endodontic and post-endodontic pain has a substantial link. Individuals with significant pre-endodontic pain have more severe post-endodontic pain than people who experience little or no pre-endodontic pain discomfort [2]. Prostaglandins (PGs) are key inflammatory mediators whose production is triggered by the release of arachidonic acid from damaged cell membranes. The most significant hyperalgesia and inflammatory mediators are most likely PGs. PGs enhance vascular permeability, increase chemotactic activity, produce fever, and increase pain receptor sensitivity to other active inflammatory mediators by sensitizing nerve terminals to bradykinins and histamines [3]. If the periapical inflammatory reaction significantly contributes to posttreatment pain, a nonsteroidal anti-inflammatory medication (NSAID) may be beneficial in its control. By reducing the activity of cyclooxygenase (COX) enzymes, NSAIDs appear to decrease inflammation and promote analgesia. COX enzymes are classified into two types: COX-1 and COX-2 [4, 5].
Nonselective NSAIDs such as ibuprofen, ketoprofen, aspirin, and naproxen block cytoprotective COX-1 enzymes and inflammatory COX-2 enzymes. As a result, extended use of these drugs has been linked to gastrointestinal tract damage, including stomach erosions, ulcers, and bleeding [6]. Medicines that precisely inhibit COX-2 enzymes while leaving cytoprotective COX-1 enzymes unaffected may give analgesic, anti-inflammatory, and antipyretic benefits while avoiding harmful effects on the gastrointestinal system, other organs, and platelets. According to studies utilizing postextraction animals, ibuprofen medication suppresses post-endodontic pain better than a placebo [7]. As a result, using an NSAID before root canal therapy may interfere with the inflammatory process before it begins, potentially lowering post-endodontic discomfort [8]. Rofecoxib is a nonsteroidal anti-inflammatory medication that can particularly inhibit the COX-2 enzyme [9]. Recent investigations employing oral surgery models revealed that the pain reduction and peak analgesic effects of rofecoxib and ibuprofen were almost equal. Unlike the shorter-acting ibuprofen (4- 6 hours), rofecoxib provided meaningful analgesia up to 24 hours after therapy [10].
If rofecoxib offers equivalent analgesic benefits to ibuprofen for managing acute pain but without the potential side effects, it may play an essential role in treating acute odontogenic pain. However, the effectiveness of rofecoxib in managing post-endodontic pain when provided before treatment has yet to be determined [11]. Rofecoxib’s efficacy to control postendodontic pain when provided prophylactically has not been studied. The goal of this systematic review is to investigate whether selective COX -2 inhibitor in comparison with other analgesics for post- endodontic pain might significantly reduce post endodontic pain. Another goal was to compare the clinical efficacy of selective COX -2 inhibitors with other analgesics for the management of post-endodontic pain.
Method and Search Strategy
This updated systematic review complies with the PRISMA checklist guidelines for systematic reviews and meta-analyses [12]. Google Scholar, Web of science, Cochrane and PubMed were the databases that were searched. The two databases were utilized to survey for studies on our main topic, “The clinical efficacy of selective COX -2 inhibitors in managing endodontic pain” The studies were published between 2000 and 2023. The search process involved using different keywords, including “selective COX-2 inhibitors; selective non-steroidal anti-inflammatory drug; endodontic pain; meloxicam; etoricoxib; metabolic complications”. In addition, the involved keywords were employed to collect all relevant articles. This initial exploration resulted in the revision of all titles.
Eligibility Criteria
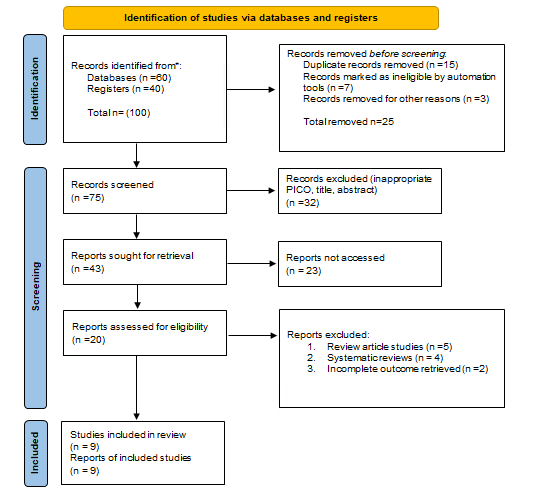
Only papers focusing on the clinical efficacy of selective COX-2 inhibitors in managing endodontic pain were excluded after reviewing the clinical efficacy of selective COX-2 inhibitors in managing endodontic pain before 2000. The second phase involved selecting only original, English-language studies reporting the clinical efficacy of selective COX-2 inhibitors in managing endodontic pain after evaluating the abstracts of the remaining articles. On the other hand, review articles and editor letters were not included. The final stage included original English-language articles discussing and evaluating the clinical efficacy of selective COX-2 inhibitors in managing endodontic pain. These articles were further examined to exclude duplicates, non-full-text articles, and articles with unsatisfactory content, such as overlapped or incomplete data. Figure 1 displays a detailed explanation of the search approach.
Data Reviewing and Analysis
The full text and abstracts of the articles were evaluated to extract the relevant data and transfer it to a pre-made excel sheet. The chosen data were then amended in the excel sheet, and the data were combined to summarize the data to facilitate data analysis.
Bias Risk Assessment
Using the “Risk of Bias” method for Cochrane reviews, assessments of the risk of bias were made for randomised controlled trials (RCTs). Because there is no agreement on how to use these measures in observational studies, they were not conducted; yet, we believe they are biassed and susceptible to confounding influences. Each study was assessed separately by the two reviewers. All differences of opinion were settled by consensus or by talking to the third author (RHGM).
Measurements of Treatment Effect
Two measuring methods for the interventional effect were utilized. For trials that exclusively assessed the effects of the MMC intervention, a proportional meta-analysis was carried out using Stats Direct (Stats Direct Ltd, Birkenhead, Merseyside, UK) software, version 3.0.121. To summarise dichotomous outcome data that was given as a proportion with their matching 95% confidence intervals (95%CIs), forest plots were created.
Results
This updated systematic review’s inclusion criteria were satisfied by eight studies [13, 14, 15, 16, 17, 18, 19, 20, 21]. The included studies were either published in Nekoofar MH, et al. [20], Mirzaie M, et al. [16], Krishna A, et al. [15], Madani ZS, et al. [18, 19], Sheikh A, et al. [21], Ashraf H, et al. [17], Abbas B, et al. [14], and Elnaghy AM, et al. [13]. All the studies were double- blinded randomized clinical trials. The study population was comprised of 1645 patients with endodontic pain. One study [13] investigated how oral premedication with meloxicam (selective COX-2 inhibitor), ketorolac, dexamethasone, and Ibuprofen affected the success rate of an inferior alveolar nerve block for patients with symptomatic irreversible pulpitis, and another study [19] compared the results of a single dose of two oral medications with a single visit root canal therapy in teeth with irreversible pulpitis. One study [15] investigated the effectiveness of Prophylactic use of Etoricoxib in Comparison with Ibuprofen on Postendodontic Pain. Another study [16] explored the effect of premedication with Celecoxib and Gelofen on reduction of post-endodontic pain, while one more study [20] evaluated Meloxicam (A Cox- 2 Inhibitor) for Management of Post Endodontic Pain.
One study determined the effectiveness of Celecoxib and Celebrex in pain and controlling endodontic pain [17], In addition, one study compared the efficacy of celecoxib versus naproxen [14] for managing post-endodontic pain. Etoricoxib provided significantly better pain relief than placebo and ibuprofen [15]. According to study [16], the use of Gelofen or Celecoxib before treatment reduces post- endodontic pain. Celecoxib and Gelofen can be prescribed before initiation of treatment as the effective agents for reduction of postendodontic pain. Celebrex was determined to be an appropriate choice for pain management following periodontal pain [17], given the lower rate of side effects associated with COX-2- specific inhibitors. Celebrex has been found to be more effective for treating post-endodontic pain. According to one study [13], premedication with meloxicam, ketorolac, dexamethasone, and Ibuprofen enhanced the effectiveness of inferior alveolar nerve blocks (IANB) in mandibular molars with symptomatic irreversible pulpitis. In addition, no significant differences between efficacy of meloxicam, piroxicam, and placebo, but a significant effect of the time factor in reducing post-endodontic pain in all treatment groups was observed [20]. In comparison to celecoxib and the placebo group, prophylactic Celebrex administration significantly decreased post-endodontic pain following the start of root canal therapy (RCT) [17].
When comparing Ibuprofen and Celecoxib, There was no statistically significant difference in the ability of Ibuprofen and Celecoxib to manage post-endodontic pain between the patient groups taking each medication [21]. While another study [14] discovered that, compared to Naproxen, Celecoxib was more effective in treating post-endodontic pain with minimal gastric symptoms. Compared to the other two groups, etoricoxib reduced post-endodontic pain by 10% more, which was clinically significant. In comparison to the other two groups, taken right after the RCT of teeth with irreversible pulpitis, a single dose of etoricoxib significantly decreased the post-endodontic pain [19]. When comparing etoricoxib and diclofenac, one study [18] demonstrated that both treatments were equally effective. Compared to diclofenac and placebo, etoricoxib treatment demonstrated a more significant reduction in the incidence and intensity of post-endodontic pain after third molar treatment [19].
Discussion
Endodontic treatment is considered a harrowing experience for patients in dental practice [22]. Pain is already present before initiation of root canal treatment. Instead, it is the presenting complaint compelling patient to seek advice. After successful completion of treatment, post- endodontic pain resolves in most cases; however, pain perception remains in some cases leading to an unsatisfactory experience for the patient. In the case of post-endodontic pain, the primary mechanism responsible for pain production is inflammatory, and patients are ambulatory day cases; therefore non -steroidal anti-inflammatory drugs are the most suited ones due to the possession of anti-inflammatory properties inferred by inhibition of the activity of cyclooxygenase enzyme thus leading to the cessation of prostaglandin production with avoidance of cumbersome side effects such as nausea, vomiting, and respiratory depression remarkably associated with opioids. They are principally divided into two groups based on the inhibition of cyclooxygenase enzymes (COX), such as non-selective cyclooxygenase 1 & 2 inhibitors (COX- 1, two and selective cyclooxygenase inhibitor (COX-2) [23].
COX-2 is a prime agent in inflammation and cell growth due to its relation with pro- inflammatory cytokines. The advent of COX-2 led to the emergence of analgesics such as celecoxib which provide analgesia without compromising renal and gastrointestinal safety [24]. In this systematic review, we aimed to assess the clinical efficacy of selective COX -2 inhibitors compared to other analgesics for managing post- endodontic pain. According to the present systematic review results, Celebrex was an appropriate choice for pain management following periodontal pain. Ashraf H, et al. [17] reported that in comparison to celecoxib and the placebo group, prophylactic Celebrex administration significantly decreased post-endodontic pain following the start of root canal therapy (RCT). When comparing Ibuprofen and Celecoxib, Sheikh A, et al. [21] reported no statistically significant difference in the ability of Ibuprofen and Celecoxib to manage post-endodontic pain between the patient groups taking each medication. While Abbas B, et al. [14] discovered that, compared to Naproxen, Celecoxib was more effective in treating post-endodontic pain with minimal gastric symptoms. Krishnaprasada L, et al. [19] found that etoricoxib reduced post-endodontic pain by 10% more, which was clinically significant. A single dose of etoricoxib significantly decreased the post-endodontic pain compared to the other two groups, taken right after the RCT of teeth with irreversible pulpitis. Krishna A, et al. [15] showed that Etoricoxib provided significantly better pain relief than placebo and ibuprofen. Additionally, Mirzaie M, et al. [16] reported that the use of Gelofen or Celecoxib before treatment reduces post-endodontic pain. Moreover, Nekoofar MH, et al. [20] found no significant differences between efficacy of meloxicam, piroxicam, and placebo, but a significant effect of the time factor in reducing post- endodontic pain in all treatment groups was observed.
Celecoxib is a selective COX-2 inhibitor indicated for the treatment of acute pain, osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, and primary dysmenorrhea. It should not be used in patients with hypersensitivity reactions, e.g., asthma, ischemic heart disease, cerebrovascular disease, or compromised renal function. Side effects experienced with celecoxib are raised blood pressure, headache, dizziness, sodium, and fluid retention [25]. Naproxen is a COX-1 &2- inhibitor indicated for treating acute pain, fever, and inflammatory diseases such as rheumatoid arthritis, ankylosing spondylitis, and primary dysmenorrhea. It exhibits its effects by inhibition of prostaglandins responsible for inflammation and pain. Side effects are heart burns, stomach pain, bruising, gastrointestinal bleeding, and cerebrovascular accidents [26]. Chao X, et al. [27] compared celecoxib with a placebo; a study suggested that celecoxib (200mg orally once daily) when compared with a placebo, results in more significant pain relief with acceptable adverse effects for treating orthodontic pain [27]. Pain and discomfort were significantly less severe in the Celecoxib group compared to the placebo group at 3-hour post-endodontic intervals [28].
When comparing etoricoxib and diclofenac, Madani ZS, et al. [18] demonstrated that both treatments were equally effective, while Krishnaprasada L, et al. [19] found that etoricoxib treatment demonstrated a more significant reduction in the incidence and intensity of post-endodontic pain after third molar treatment compared to diclofenac and placebo. Many studies have investigated the efficacy of COX-2 inhibitors for treating surgically induced dental pain but failed to show any clear therapeutic advantage over ibuprofen [29, 30]. It is reported that a single dose of 40 mg oral celecoxib mg), as a selective COX-2 inhibitor, had similar efficacy for post-endodontic pain relief compared to 40 mg ibuprofen [31].
Another study found that ibuprofen was just as efficient as rofecoxib for reducing immediate post-endodontic pain after third molar treatment [32]. However, in many studies, NSAIDs (selective or non-selective) were better than other analgesics, including opioids [33, 34]. The overall analgesic effectiveness of a single dosage of etoricoxib (120 mg) over 6 hours was proven to be superior to that of a single dose of oxycodone/acetaminophen (10/650 mg) in the treatment of acute post-endodontic dental pain. Etoricoxib had a rapid onset of action, and it has a peak analgesic effect similar to that of oxycodone/acetaminophen but with a longer duration. The administration of etoricoxib reduced the need for rescue opioid analgesia compared with the administration of oxycodone/acetaminophen [35].
Conclusion
This systematic review demonstrated that Selective COX -2 Inhibitors was an effective choice in managing post- endodontic pain. Celebrex was more effective than Celecoxib in relieving post-endodontic pain. When comparing Ibuprofen and Celecoxib, both were equally effective in relieving post- endodontic pain. Celecoxib was more effective than Naproxen
in treating post-endodontic pain with minor gastrointestinal effects. Furthermore, etoricoxib considerably reduces post- endodontic pain with a single dosage. Both etoricoxib and diclofenac had the same effectiveness in reducing pain; however, etoricoxib medication significantly reduced the incidence and severity of post- endodontic pain.
References
-
Galani M, Tewari S, Sangwan P, Mittal S, Kumar V, et al. (2017) Comparative Evaluation of Postoperative Pain and Success Rate after Pulpotomy and Root Canal Treatment in Cariously Exposed Mature Permanent Molars: A Randomized Controlled Trial. J Endod 43(12): 1953-1962.
-
Bagheri M, Khimani H, Pishbin L, Shahabinejad H (2019) Effect of Pulpotomy Procedures with Mineral Trioxide Aggregate and Dexamethasone on Post-endodontic Pain in Patients with Irreversible Pulpitis: A Randomized Clinical Trial. Eur Endod J 4(2): 69-74.
-
Korbut R, Guzik TJ (2019) Inflammatory Mediators and Intracellular Signalling. Nijkamp & Principles of Immunopharmacology, pp: 139-163.
-
Fokunang C, Fokunang ET, Frederick K, Ngameni B, Ngadjui B (2018) Overview of Non-Steroidal Anti- Inflammatory Drugs (nsaids) in Resource Limited Countries. Moj Toxicol 4(1): 5-13.
-
Rayar AM, Lagarde N, Ferroud C, Zagury JF, Montes M, et al. (2017) Update on COX-2 Selective Inhibitors: Chemical Classification, Side Effects and their Use in Cancers and Neuronal Diseases. Curr Top Med Chem 17(26): 2935-2956.
-
Sehajpal S, Prasad DN, Singh RK (2018) Prodrugs of Non- steroidal Anti-inflammatory Drugs (NSAIDs): A Long March towards Synthesis of Safer NSAIDs. Mini Rev Med Chem 18(14): 1199-1219.
-
Quesada-Bravo FJ, Garcia-Carricondo AR, Espin-Galvez F, Fernandez-Sanchez C, Fernandez-Gines D, et al. (2021) Comparative Study between the Combination of Dexamethasone and Bupivacaine for Third Molar Surgery Postoperative Pain: A Triple-Blind, Randomized Clinical Trial. J Clin Med 10(21): 5081.
-
Konagala RK, Mandava J, Pabbati RK, Anupreeta A, Borugadda R, et al. (2019) Effect of Pretreatment Medication on Postendodontic Pain: A Double-Blind, Placebo-Controlled Study. J Conserv Dent 22(1): 54-58.
-
Ahmadi M, Bekeschus S, Weltmann KD, Von Woedtke T, Wende K (2022) Non-steroidal Anti- Inflammatory Drugs: Recent Advances in the Use of Synthetic COX-2 Inhibitors. RSC Med Chem 13(5): 471-496.
-
Mohammadi Z, Farhad A, Khalesi M (2008) Pharmacological Strategies to Control Post-operative Endodontic Pain. Dental Research Journal 4(2): 61-68.
-
Smith EA, Marshall JG, Selph SS, Barker DR, Sedgley CM (2017) Nonsteroidal Anti- inflammatory Drugs for Managing Postoperative Endodontic Pain in Patients who Present with Preoperative Pain: A Systematic Review and Meta-Analysis. J Endod 43(1): 7-15.
-
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, et al. (2009) The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies that Evaluate Health Care Interventions: Explanation and Elaboration. BMJ 339: b2700.
-
Elnaghy AM, Elshazli AH, Elsaka SE (2023) Effectiveness of Oral Premedication of Meloxicam, Ketorolac, Dexamethasone, and Ibuprofen on the Success Rate of Inferior Alveolar Nerve Block in Patients with Symptomatic Irreversible Pulpitis: A Prospective, Double- Blind, Randomized Controlled Trial. Quintessence Int 54(2): 92-99.
-
Abbas B, Abbas S, Sattar M, Rahim S, Amir S (2020) Comparison of Efficacy of Celecoxib (Selective Non- Steroidal Anti Inflammatory Drug) Versus Naproxen (Non Selective Non-Steroidal Anti Inflammatory Drug) for Post Endodontic Pain. Pak Armed Forces Med J 70(4): 1133-1137.
-
Krishna A, Vedavathi B, Uppin V, Swapna DV (2012) Effectiveness of Prophylactic use of Etoricoxib in Comparison with Ibuprofen on Postendodontic Pain- randomized Double-Blind, Placebo-controlled Study: An in Vivo Study. World J Dent 2(3): 243-247.
-
Mirzaie M, Kavosi A, Atbaie A, Moazami F, Nooribaiat S (2011) Effect of Premedication with Celecoxib and Gelofen on Reduction of Post-Endodontic Pain. Journal of Dental Medicine 24(3):172-180.
-
Ashraf H, Bidabadi MM, Noghlachi T, Darmiani S (2018) Controlling Postendodontic Pain in Comparison to Placebo: A Randomized Double-blind Clinical Trial. Journal of Dentomaxillofacial 7(3): 103-108.
-
Madani ZS, Moghadamnia AA, Panahi A, Mir AP (2013) Analgesic Effect of Etoricoxib Compared to Ibuprofen on Post Endodontic Pain. Oral Health Dent Manag 12(3): 186-190.
-
Krishnaprasada L, Nambiar JM (2013) A Comparative Evaluation of the Efficacay of Two Oral Medication on Post-operative Pain following Single Visit Root Canal Therapy-An in Vivo Study. IOSR-JDMS 5(2): 1-4.
-
Nekoofar MH, Sadeghipanah M, Dehpour AR (2003) Evaluation of Meloxicam (A Cox-2 Inhibitor) for Management of Postoperative Endodontic Pain: A Double-blind Placebo-Controlled Study. J Endod 29(10): 634-637.
-
Sheikh A, Agwan MA, Amin M, Khan MA, Sheikh I, et al. (2014) Comparison of Ibuprofen and Celecoxib for Controlling Post Endodontic Pain. Journal of the Pakistan Dental Association 23(3).
-
Zhu X (2020) Efficacy of Preemptive Analgesia Versus Postoperative Analgesia of Celecoxib on Postoperative Pain, Patients’ Global Assessment and Hip Function Recovery in Femoroacetabular impingement Patients Underwent Hip Arthroscopy Surgery. Inflammopharmacology 28(1): 131-137.
-
Kianian F, Seifi B, Kadkhodaee M, Sajedizadeh A, Ahghari P (2019) Protective Effects of Celecoxib on Ischemia Reperfusion–Induced Acute Kidney Injury: Comparing between Male and Female Rats. Iran J Basic Med Sci 22(1): 43-48.
-
Solomon DH, Husni ME, Wolski KE, Wisniewski LM, Borer JS (2018) Differences in Safety of Nonsteroidal Antiinflammatory Drugs in Patients with Osteoarthritis and Patients with Rheumatoid Arthritis: A Randomized Clinical Trial. Arthritis Rheumatol 70(4): 537-546.
-
Shete PG, Shete NG, Kumbhakaran DN, Mane NS, Padole VS, et al. (2020) Review on Celecoxib: A Oral Cox-2 Inhibitor. Int J RPC 10(4): 382-389.
-
Garg U, Azim Y (2021) Challenges and Opportunities of Pharmaceutical Cocrystals: A Focused Review on Non- Steroidal Anti-Inflammatory Drugs. RSC Med Chem 12(5): 705-721.
-
Chao X, Ke G, Yalikun Y, Yanjie H (2016) Efficacy and Safety of Celecoxib Therapy in Osteoarthritis. A Meta- analysis of Randomized Controlled Trials. Medicine 95(20): e3585-e3594.
-
Nivethithan T, Raj JD (2015) Endodontic Pain-cause and Management: A Review. International Journal of Pharmaceutical Sciences and Research 6(7): 2723-2727.
-
Stiller CO, Hjemdahl P (2022) Lessons from 20 years with COX‐2 Inhibitors: Importance of Dose-Response Considerations and Fair Play in Comparative Trials. J Intern Med 292(4): 557-574.
-
Fokunang C, Fokunang ET, Frederick K, Ngameni B, Ngadjui B (2018) Overview of Non-steroidal Anti- inflammatory Drugs (nsaids) in Resource Limited Countries. Moj Toxicol 4(1): 5-13.
-
Fenton C, Lee A (2022) Manage Endodontic Pain with a Combination of Analgesics, Including Non-Steroidal Anti-Inflammatory Drugs. Drugs & Therapy Perspectives 38(3): 127-132.
-
Khan AA, Dionne RA (2002) COX‐2 Inhibitors for Endodontic Pain. Endodontic Topics 3(1): 31-40.
-
Pelletier JP, Martel-Pelletier J, Rannou F, Cooper C (2016) Efficacy and Safety of Oral NSAIDs and Analgesics in the Management of Osteoarthritis: Evidence from Real-life Setting Trials and Surveys. Semin Arthritis Rheum 45(4 Suppl): S22-S27.
-
Schjerning AM, McGettigan P, Gislason G (2020) Cardiovascular Effects and Safety of (Non-Aspirin) NSAIDs. Nat Rev Cardiol 17(9): 574-584.
-
Kis J (2023) Pharmacotherapy in Endodontics.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells