Full Term Pregnancy after Recurrent Borderline Epithelial Ovarian Tumor
Incidence of borderline ovarian tumours (BOTs) ranges from 10-15% of all ovarian tumours. They affect a younger age group than the ovarian carcinoma and have a much better prognosis. Over the last decades, the management of borderline ovarian tumors has changed from radical surgery to more fertility oriented therapy. Fertility-sparing surgery is defined as surgery with complete staging, but where the uterus and at least a part of one ovary are preserved
Introduction
Incidence of borderline ovarian tumours (BOTs) ranges from 10-15% of all ovarian tumours. They affect a younger age group than the ovarian carcinoma and have a much better prognosis. Over the last decades, the management of borderline ovarian tumors has changed from radical surgery to more fertility oriented therapy. Fertility-sparing surgery is defined as surgery with complete staging, but where the uterus and at least a part of one ovary are preserved. It presents a good option in young patients with early-stage disease or in selected cases with noninvasive implants, since long-term survival does not seem to be negatively influenced by conservative surgery [1, 2]. There is still a debate regarding the optimal conservative treatment for both serous and mutinous borderline ovarian tumour (BOT), also, whether to give ovarian stimulation in case of recurrence or not.
Case
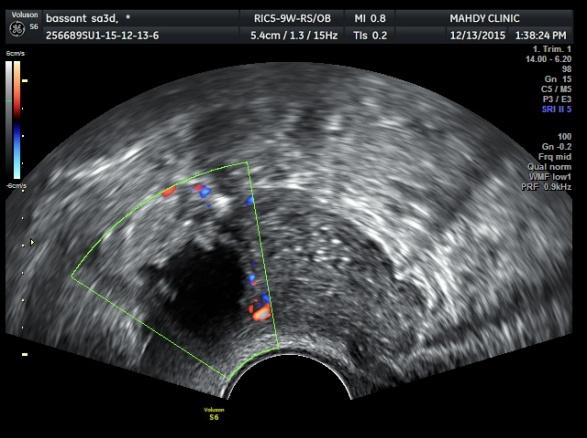
Peritoneal wash was obtained. Adhesiolysis was done left adnexectomy and right ovarian cystectomy was done. Histopathological examination revealed bilateral serous borderline epithelial ovarian tumor with predominant micro papillae without invasion or peritoneal involvement. Follow up of the patient was every 3 month and was completely free. After one year away from follow up due to marriage, recurrence of multilocular complex ovarian mass on the right ovary was detected by ultrasound and associated by elevated CA125 which was 249. Doppler ultrasound showed vascular thick wall with low resistance (Figure 1).
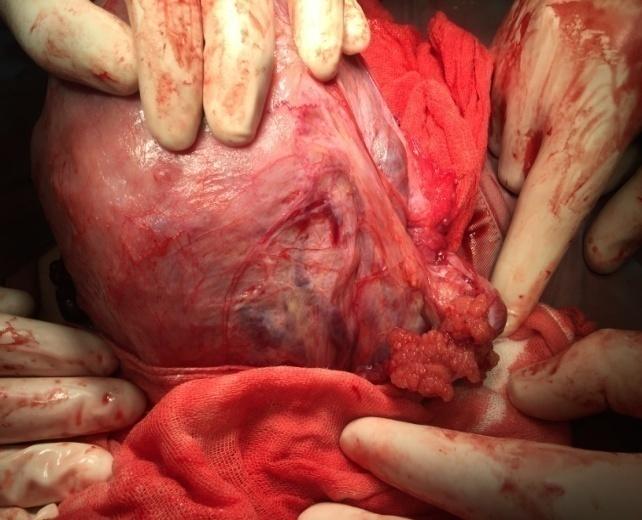
Decision of ICSI was discussed with the couple. ICSI was started after investigations which showed very low ovarian reserve parameters; AMH less than 0.1. ICSI through stop agonist protocol was started. Midluteal pituitary down regulation by Triptorelin was started. After complete pituitary down regulation, GnRH agonist was stopped and stimulation started by 450 IU FSH and HMG. After 11 days of stimulation 4 follicles reached 19, 19, 20 and 21 mm and serum E2 level was 928 and serum level of P4 was 0.8. Ovum pick up was done after 34 hours of ovulation triggering by 10000 IU of HCG and revealed 3 mature oocytes without puncturing the cystic structure. After 3 days of sperm injection and incubation 2 good quality embryos were transferred to the uterus under ultrasound guidance. Luteal phase support in the form of vaginal, intramuscular progesterone and thrombophylaxis. After 17 days of embryo transfer serum BHCG was 475 and after that intrauterine sac was identified inside the uterus after 24 days of ET. The complex ovarian cystic structure was present as it was before ICSI. Follow up of pregnancy till 38 weeks of gestation. Decision of Cesarean section was taken. After extraction of the fetus the right ovary was explored and showed solid and cystic lesion (Figure 2). Excision of the lesion was done with good hemostasis and sent for histopathological examination (Figure 3). Histopathology revealed picture of atypical proliferative serous tumor (borderline serous tumor).

Discussion
The management of borderline ovarian tumors varies according to the age and reproductive status of the female. Cystectomy in unilateral serous BOT is significantly associated with a higher recurrence rate, without impact on survival. Unilateral salpingo opherectomy is advisable in the case of mucinous BOT. On the contrary, a more conservative approach bilateral cystectomy should be definitively favored in bilateral BOT, which is almost always serous, because no significant difference is seen in terms of recurrence rate when compared to USO+CC [3]. Fertility-sparing surgery is well tolerated not only in patients with early-stage BOTs but also in patients with advanced-stage BOTs with noninvasive extra ovarian implants, if these implants can be rejected completely [2]. Also, for young women with stage I epithelial ovarian cancer desiring fertility preservation, fertility-sparing surgery is a reasonable alternative treatment [4]. The risk of recurrence is higher after fertility preservation surgery compared with radical surgery; however, no influence on ovarian reserve was observed. This was because most of the patients relapsed as BOT. Fertility preservation is justified in young patients with serous borderline tumors [5]. After fertility-sparing surgery, pregnancy outcomes are promising and most pregnancies are achieved spontaneously. There are few complications associated with pregnancy, and subsequent pregnancy seems to have little impact on disease course.
Fertility drugs are well tolerated in patients with infertility after fertility-sparing surgery for early-stage BOTs. In cases of extensive tumor involvement of both ovaries, FPS can't be done instead oocyte, and ovarian tissue freezing can be used [2]. So, borderline ovarian tumors aren’t an obstacle for fertility in young women wishing fertility.
Fertility-sparing surgery in borderline ovarian tumours Akush Ginekol (Sofiia) 54(1): 21-26.
3. Vasconcelos I, de Sousa Mendes M (2015) Conservative surgery in ovarian borderline tumours: a meta-analysis with emphasis on recurrence risk. Eur J Cancer 51(5): 620-631.
4. Schlaerth AC, Chi DS, Poynor EA, Barakat RR, Brown
CL (2009) Long-term survival after fertility-sparing surgery for epithelial ovarian cancer. Int J Gynecol Cancer 19(7): 1199-1204.
5. Vancraeynest E, Moerman P, Leunen K, Amant F,
Neven P, et al. (2016) Fertility Preservation Is Safe for Serous Borderline Ovarian Tumors. Int J Gynecol Cancer.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’