Role of Hysteroscopy in Evaluation of Infertility: A Retrospective Study of 100 Cases
Objective: To determine role of hysteroscopy in evaluation of infertility Method: This retrospective observational study was carried out at Gynaecology endoscopy unit, PSRI, DELHI, over a period of one year. 100 Infertile women were included in the study. Hysteroscopy was performed by using 2.9mm 300 BETTOCHI hysteroscope. Data was collected from the medical records department of the hospital. Results: Among 100 women, abnormal hysteroscopic findings were found in 56% women, majority of which (76.8%) were with primary infertility and 60.7% were of age ≥30 years. The most common uterine cavity abnormality was intrauterine adhesions, seen in 46.4% cases. Among these, majority of the adhesions were of grade I (65.4%). Endometrial polyp, subseptate uterus, submucous myoma, and unicornuate uterus was seen in 23.2%, 12.5%, 8.9%, and 1.7% cases respectively. Cervical lesions such as cervical polyp, cervical adhesions and cervical growth were seen in 5.3% of cases, where each of them constituted 1.7% of cases. Conclusion: This study suggests that since hysteroscopy was able to identify intrauterine pathologies in 56% of women with infertility, it should be considered as a routine investigation in evaluation of infertile woman.
Synopsis
During hysteroscopy, abnormal uterine cavity findings were found in majority of infertile woman, suggesting that hysteroscopy should be considered as routine investigation in infertility.
Introduction
Infertility is “a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse” according to WHO revised glossary of assisted reproductive technology (ART). It affects 10-15% of infertile couples [1].
Infertility related to uterine cavity abnormalities has been estimated to be the causal factor in as many as 10% to 15% of couples seeking treatment. Moreover, abnormal uterine findings have been found in 34% to 62% of infertile women [2]. These uterine pathologies result in structural and functional impairment of endometrium, thus making the endometrium unfit for implantation. Hence, assessment of uterine cavity should be included in work up of an infertile couple. The tools to assess uterine cavity are Transvaginal ultrasonography (TVS), Hysterosalpingography (HSG), Saline infusion sonography (SIS) and Hysteroscopy. Transvaginal ultrasonography (TVS) is the simplest imaging examination which is non-invasive, cost effective and has high clinical significance. It helps in evaluation of size, shape, volume and contour of the uterine cavity and determination of any intrauterine pathology. The overall sensitivity and specificity for TVS in the diagnosis of intra- uterine abnormality is 79% and 82% respectively [3]. However, TVS carries some limitations which are inability to detect the endometrial changes such as endometritis and synechiae, difficulty in differentiating between a polyp and a fibroid. Also, tubal patency cannot be assessed on transvaginal sonography. HSG is helpful in defining size and shape of uterine cavity. It can reveal congenital (unicornuate, septate, bicornuate uteri) and acquired uterine anomalies (polyp, sub mucous myoma, synechiae). All intrauterine pathology like polyp, myoma, synechiae or septa appears as a filing defect on HSG. To further differentiate these lesions either TVS or hysteroscopy is required to be done. So, HSG has a relatively low sensitivity (50 %) and positive predictive value (30%) for diagnosis of endometrial polyp and sub mucous myoma in infertile women [4]. SIS is a minimally invasive, cost-effective and acceptable diagnostic modality. It gives an excellent anatomic detail of the uterus and has been shown to be highly accurate in the diagnosis of polyp, endometrial hyperplasia, and various uterine anomalies. The pooled sensitivity of SIS in the detection of all intrauterine abnormalities was 88% with specificity of 94% [5]. Hysteroscopy is considered as gold standard in the diagnosis of intrauterine pathology. However, WHO recommends office hysteroscopy in females who are suspected of intrauterine abnormality on clinical basis or complementary exams (ultrasound, HSG) or after in vitro fertilization (IVF) failure. But many clinicians feel that direct view of the uterine cavity offers a significant advantage over other blind or indirect diagnostic methods, so even when no abnormality is found with these tools, hysteroscopy should be considered. Thus, this study is being done to determine role of hysteroscopy for evaluation of uterine cavity abnormalities in an infertile couple.
Material and Methods
This retrospective observational study was carried out at Gynaecology endoscopy unit, PSRI, DELHI, over a period of one year from March 2015 to March 2016. 100 Infertile women who underwent hysteroscopy were included in the study. After detailed clinical evaluation, all patients were informed regarding the procedure and written informed consent was taken. Hysteroscopy was performed in operation theatre by using 2.9mm 300 BETTOCHI hysteroscope with additional 1mm sheath and HD camera. No prior cervical dilatation was done. All procedures were done under general anaesthesia by same surgeon. Distension of uterine cavity was achieved with normal saline by pressure bag or Endomat. Hamou Endomat was used as fluid delivery system with inflow pressure of 150 mm Hg and outflow pressure of 0.5 bars. Endocervical canal followed by whole uterine cavity with all four walls and bilateral ostias were visualised. Endometrial biopsy was taken for histopathological examination under direct vision if required. If any pathology like intrauterine adhesions, polyp, myoma or septa was diagnosed, operative procedure was done at the same sitting. Video recording of each procedure was done for future reference. Data was collected from the medical records department of the hospital. Statistical analysis was done by using SPSS software. P value <0.05 was considered as significant.
Results
Hysteroscopy was performed in 100 infertile women, out of which 78 (78%) presented with primary infertility and 22 (22%) women were with secondary infertility.
Among 100 women with an age range of 20-48 years, 46% women were of age < 30 years while 54% women were of age ≥ 30 years. The mean age was 30.01 ± 5.48 years. The women with secondary infertility group were elder (31.1 ± 6.8 years) as compared to women with primary infertility (29.7 ± 5.01 years), however difference was statistically insignificant (p value 0.326). Among 22 women with secondary infertility, 12 (54.5%) women had parity ranging from 1 to 2, 12 (54.5%) women had history of one abortion, 6 (27.2%) had two abortions while only 1 (4.5%) women had history of three abortions. (Table 1) shows distribution of women undergoing hysteroscopy in primary and secondary infertility group. Normal intrauterine findings were found in 44 women. Majority of these women were of age less than 30 years (54.5%) and presented with primary infertility (79.5%). Abnormal Hysteroscopic findings were found in 56 women, of whom maximum women were with primary infertility (76.8%) and of age ≥30 years (60.7%), as shown in (Figure 1 & 2).
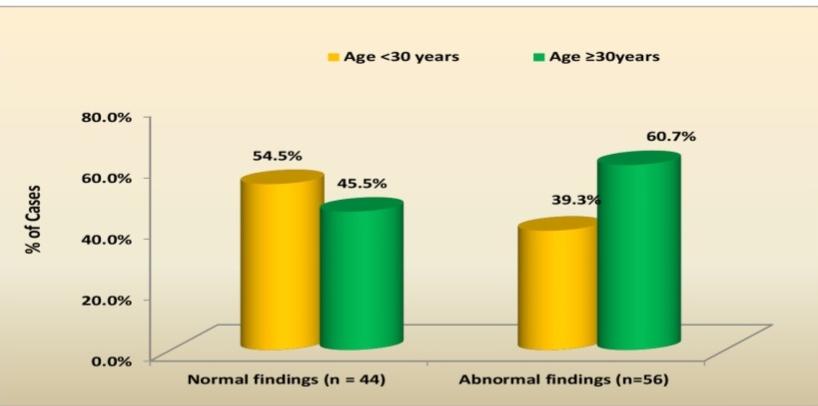
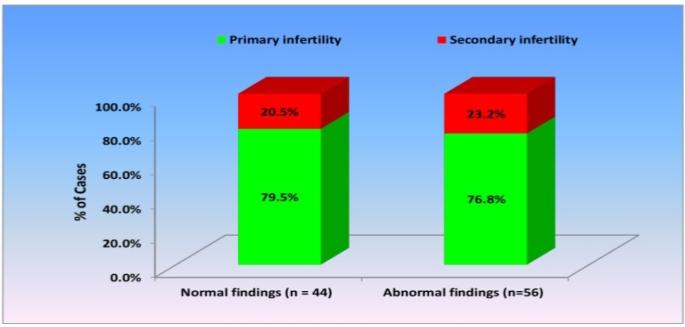
Figure 2: Bar diagram showing distribution of women with normal and abnormal hysteroscopic findings according to age. In primary infertility group, intrauterine pathologies were diagnosed in 43/78 (55.1%) women. The most common finding was intrauterine adhesions (41.8%) followed by endometrial polyp (25.5%), subseptate uterus (13.9%) and sub mucous myoma (11.6%). In group with secondary infertility, abnormal intrauterine pathologies were detected in 13/22 women (59.1%). The most common intrauterine pathology was intrauterine adhesions, seen in 36.4% women.
| Normal findings (n = 44) | Abnormal findings (n=56) | P value | |
|---|---|---|---|
| Primary infertility | 35 (79.5%) | 43 (76.8%) | 0.741 |
| Secondary infertility | 9 (20.5%) | 13 (23.2%) | |
| Age <30 years | 24 (54.5%) | 22 (39.3%) | 0.129 |
| Age ≥30 years | 20 (45.5%) | 34 (60.7%) |
Cervico-Isthmic abnormalities: Cervical adhesions was seen in 1% case only, seen in a women with primary infertility, with age < 30years. One case (1%) of endocervical growth was seen, who was 28 year old woman with primary infertility, which was later diagnosed as cervical adenocarcinoma on histopathology report. Cervical polyp was found in 1% case, who was women with secondary infertility, with age <30 years.
| Primary infertility (n=78) | Secondary infertility (n=22) | P value | |
|---|---|---|---|
| Cervical polyp | 0 (0%) | 1 (4.5%) | 0.22 |
| Cervical adhesions | 1 (1.3%) | 0 (0%) | 1 |
| Cervical cancer | 1 (1.3%) | 0 (0%) | 1 |
| Intrauterine adhesions | 18 (23.1%) | 8 (36.3%) | 0.758 |
| Grade I | 14 (17.5%) | 3 (13.6%) 3 (13.6%) 2 (9.1%) | 0.069 |
| Grade II | 2 (2.6%) | 0.209 | |
| Grade III | 2 (2.6%) | 0.209 | |
| Polyp | 1 (15.4%) | 1 (4.5%) | 0.287 |
| Myoma | 3 (3.84%) | 0 (0%) | 0.583 |
| Subseptate uterus | 6 (7.7%) | 1 (4.5%) | 0.22 |
| Unicornuate uterus | 0 (0%) | 1 (4.5%) | 0.22 |
| Ostia fibrosis | 2 (2.6%) | 1 (4.5%) | 0.53 |
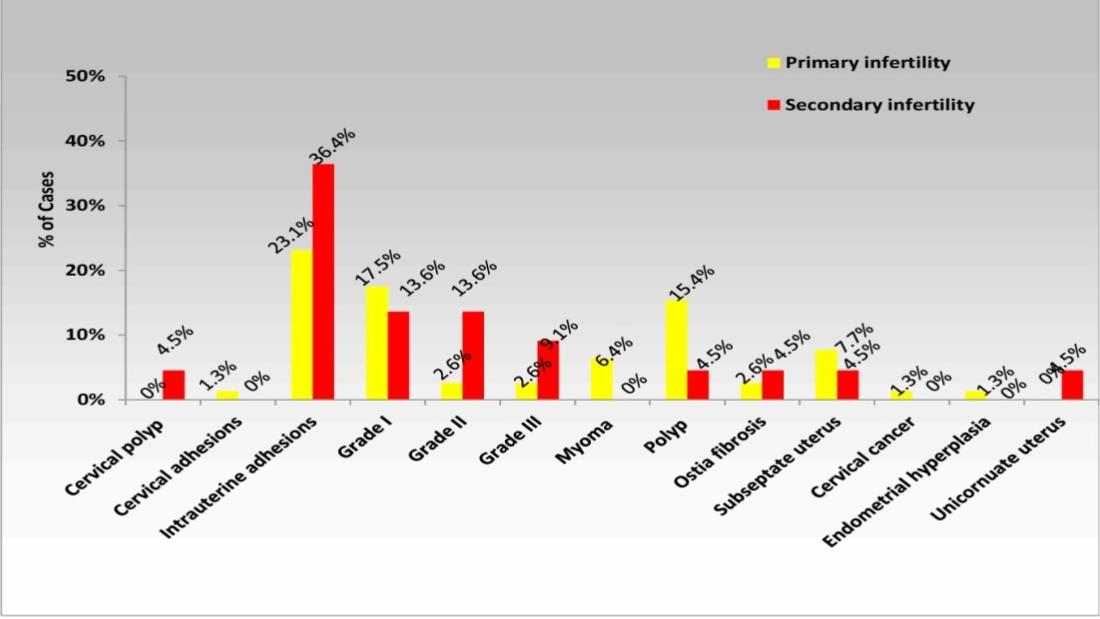
Table 2: Abnormal intrauterine pathologies in women with primary infertility and women with secondary infertility.
Uterine cavity abnormalities
Intrauterine adhesions (IUA): IUA were the most common intrauterine finding on hysteroscopy found in 26% of cases. In primary infertility group, 18/78 (23.1%) women were diagnosed with intrauterine adhesions while in women with secondary infertility, 8/22 (36.4%) women were found to have them, as shown in (Figure 3).
In most of the cases (65.4%), severity of adhesions were mild (grade I, obliteration of <1/3 of cavity, mostly singular and fundal adhesions). However, in 5/26 (19.2%) cases, grade II Asherman’s syndrome was found while another 4/26 (15.4%) cases, grade III Asherman’s syndrome i.e. more than 2/3rd of cavity was found to be obliterated.
Endometrial polyp: Endometrial polyp was the second most common finding on hysteroscopy, affecting 13% cases. In women with primary infertility, 12/78 (15.4%) women were found to have endometrial polyp, out of which in 10/12 (83.3%) cases, single polyp was diagnosed on hysteroscopy, while in 1/12 (8.33%) cases two polyps were found in each case and in another 1/12 (8.33%) case three endometrial polyps were found. In secondary infertility group, 1/22 (4.54%) women was found to have single endometrial polyp on hysteroscopy. Polypectomy was done in all cases at same sitting and diagnosis was confirmed on histopathology. Müllerian anomalies: Septate uterus was the third most common abnormality detected on hysteroscopy, seen in 7% cases. In all of these cases, partial septum was diagnosed. Maximum number of cases was diagnosed in women with primary infertility (6/7) (85.7%), while only one case (1/7) (14.3%) was seen in secondary infertility group. Hysteroscopic septoplasty was done in all cases. One case of unicornuate uterus (1%) was found, seen in women with secondary infertility, which had history of one abortion and was of age 32 years. Submucous myoma: It was found as intrauterine pathology in 3% of cases, all of which were detected in women with primary infertility. Majority of the myomas were single and of type 0 and type 1. In only one of these cases, multiple myomas [2] were detected. Myomectomy was done and specimen was sent for histopathological diagnosis. Ostial abnormalities: Ostial fibrosis was detected in 3% of cases, out of which 2/3 cases (66.7%) were seen in primary infertility group while 1 case (33.3%) was seen in women with secondary infertility. All three patients had partial tubal blockage. Complication of procedure was seen in only 1 (1%) case. Perforation of uterus occurred during resection of septum in women with primary infertility with subseptate uterus. It was managed conservatively and patient was well postoperatively.
Discussion
Evaluation of uterine cavity is one of the most important steps in the work up of infertile couple. Congenital and acquired disorders of uterine cavity can lead to impairment of endometrium and thus interfering in embryo implantation and growth of fetus [2]. Several investigations are available for evaluating the uterine cavity including TVS, HSG, SIS and hysteroscopy. Hysteroscopy is now days considered as most definite technique for evaluation of uterine cavity in infertility patients since it aids not only in diagnosing the pathology but also its simultaneous management [6]. In the present study out of 100 hysteroscopy performed, 78 were performed for evaluation of women with primary infertility, while 22 women had secondary infertility. Abnormal uterine findings included cervical adhesions, cervical polyp, cervical growth, intrauterine adhesions, endometrial polyp, submucous myoma, Ostial fibrosis, septate uterus and unicornuate uterus. 56% women who underwent hysteroscopy for infertility work up were found to have abnormal uterine cavity findings on hysteroscopy. The previously published data show large ranges of abnormal finding rates from one study to another (7.2% to 64%) [7, 8, 9, 10, 11, 12, 13, 14, 15]. These differences could be explained by the Hysteroscopic technique used, type of Hysteroscopic distension medium [16] , characteristics of the population including age of the population, ethnic factor, type of infertility (primary or secondary) and indications for hysteroscopy (infertility alone, hysterosalpingography abnormalities, prior to IVF). This proportion of abnormal uterine finding was found to be increased with age, ranging from 40% at age less than 30 years to 60% in women with age ≥30 years as seen in the present study. The results were comparable to study by Dicker D et al [7], who did a comparative study to determine role of hysteroscopy prior to in vitro fertilization-embryo transfer in elderly women. Hysteroscopy was done in 284 women, out of which uterine abnormalities was revealed in 29.9% of all patients and it was found that abnormal findings were significantly higher in the elderly women of age over 40 years in comparison to those of age less than 40 years (P <0.001). No significant difference in the rate of uterine pathology was found between women with primary (76.8%) and secondary infertility (23.2%). Complication occurred in only one case (1%), case of 34 year old woman with primary infertility, who was found to have incomplete septa on hysteroscopy. During resection of septum, perforation of uterine cavity occurred. The case was managed conservatively and patient was discharged on third day of surgery. No other complication was found during the study. Out of 56 women with abnormal intrauterine finding on hysteroscopy, the most common pathology found in the present study was intrauterine adhesions, seen in 26
women (46.4%). However, various studies has shown comparatively lower incidence of intrauterine adhesions ranging from 3-10% [17, 18, 19]. Grade 1 Asherman’s syndrome was found most commonly in 17/26 cases, with either fundal adhesions or singular fibrous adhesions or obliteration of cavity <1/3rd. Grade 3 Asherman’s syndrome was found in only 4/26 cases with obliteration of >2/3rd of cavity. Adhesiolysis was done mechanically with scissors in single or multiple sitting, depending on the grading of disease. Intrauterine device was inserted in grade 2-3 Asherman’s syndrome to prevent apposition of uterine wall and reformation of adhesions. Postoperatively patient was given high dose of estrogens along with progesterone. Risk of adhesions is positively correlated with uterine curettage done for missed abortion, incomplete abortion or post partum bleeding, thus more commonly seen in women with secondary infertility. However, No significant difference was found in incidence of intrauterine adhesions between women with primary and secondary infertility in our study. Similarly, Oliveira et al has found 10% intrauterine adhesions on hysteroscopy in women with repeated IVF failure without any prior history of uterine manipulation, thus bringing to conclusion that other factors also should be considered in pathogenesis of intrauterine adhesions. Endometrial polyp was diagnosed in 13 (21.8%) cases out of 56 cases of abnormal intrauterine pathology, of which no statistically significant difference was seen between primary and secondary infertility group. Shokeir TA et al [20] did a study to determine incidence of endometrial polyps on hysteroscopy in an infertile eumenorrheic population. Out of 244 women who underwent hysteroscopy, endometrial polyp was found in 36 (13.53%) patients. Also it was found that 50% pregnancy rate was achieved by Hysteroscopic polypectomy. Hence it was concluded that Diagnostic hysteroscopy should be used routinely in the work-up of infertile woman and persistent functional endometrial polyps, even if small, are likely to impair fertility so removal of such lesions should be done to improve subsequent reproductive performance. Developmental uterine anomalies have long been associated with pregnancy loss and obstetric complications, but the ability to conceive is generally not affected. Septate uterus is one of the common developmental intrauterine anomalies. In our study, it was seen in 7/56 cases (12.5%). The pooled data suggest that the prevalence of septate uterus is similar in infertile and fertile women (approximately 1%), but is significantly higher in women with recurrent pregnancy loss (approximately 3.5%) [21]. It is associated with various complications such as first trimester pregnancy loss, second trimester abortion and preterm delivery. Pregnancy outcomes dramatically improved after surgical correction. Previously, surgical correction of septate uterus was done by abdominal metroplasty, which was associated with increased morbidity and future pregnancy complications due to scarred uterus. Currently, the modern operative Hysteroscopic techniques have made it a relatively easy and brief day care procedure with low morbidity and prompt recovery. Therefore, hysteroscopy helps in not only diagnosing the septa but also its simultaneous resection. Uterine myoma was found in 5/56 (9%) women in the current study. Proposed mechanisms by which myoma might adversely affect fertility include dysfunctional uterine contractility interfering with ovum or sperm transport or embryo implantation, cornual myoma compressing the interstitial segment of the tube and poor regional blood flow resulting in focal endometrial attenuation or ulceration [22]. Donnez and Jadoul tried to address the issue of whether myomas influence fertility, by reviewing 106 relevant articles [23]. They concluded that they do influence fertility, mainly based on the favourable pregnancy rates obtained after Myomectomy. Furthermore, they concluded that submucous and intramural myomas distort the cavity, impairing implantation and pregnancy rates in women undergoing IVF. Hence, Hysteroscopy not only diagnose these pathologies, but also enables Myomectomy at same siting [24].
Conclusion
Authors here conclude that hysteroscopy should be considered as routine investigation in evaluation of women with primary and secondary infertility.
References
-
Pundir J, El Toukhy T (2010) Uterine cavity assessment prior to IVF. Womens Health (Lond Engl) 6(6): 841-848.
-
Brown SE, Coddington CC, Schnorr J, Toner JP, Gibbons W, et al. (2000) Evaluation of outpatient hysteroscopy, saline infusion hysterosonography and hysterosalpingography in infertile women: a prospective, randomized study. Fertil Steril 74(5): 1029-1034.
-
Maryam N, Hadieh H, Ahmadi F, Fatemeh N, Mohammad C (2012) Diagnostic Accuracy of Transvaginal Sonography in the Detection of Uterine Abnormalities in Infertile Women. Iran J Radiol 9(3): 139-144.
-
Soares SR, Barbosa dos Reis MM, Camargos AF (2000) Diagnostic accuracy of sonohysterography, transvaginal sonography, and hysterosalpingography in patients with uterine cavity diseases. Fertil Steril 73(2): 406-411.
-
Seshadri S, El-Toukhy T, Douiri A, Jayaprakasan K, Khalaf Y (2015) Diagnostic accuracy of saline infusion sonography in the evaluation of uterine cavity abnormalities prior to assisted reproductive techniques: a systematic review and meta-analyses. Hum Reprod Update 21(2): 262-274.
-
(2015) Practice committee of American Society for Reproductive Medicine. Diagnostic evaluation of the infertile female: a committee opinion. Birmingham, AL: American Society for Reproductive Medicine. Fertil Steril 103(6): e44-e50.
-
Dicker D, Goldman JA, Ashkenazi J, Feldberg D, Dekel A (1990) The value of hysteroscopy in elderly women prior to in vitro fertilization-embryo transfer (IVF- ET): a comparative study. Journal of In Vitro Fertilization and Embryo Transfer 7(5): 267-270.
-
Brusco GF, Arena S, Angelini A (2001) The role of diagnostic hysteroscopy in infertile women. Minerva Ginecologica 53(5): 313-316.
-
Preutthipan S, Linasmita V (2003) A prospective comparative study between hysterosalpingography and hysteroscopy in the detection of intrauterine pathology in patients with infertility. Journal of Obstetrics and Gynaecology Research 29(1): 33-37.
-
Pansky M, Feingold M, Sagi R, Herman A, Schneider D, et al. (2006) Diagnostic hysteroscopy as a primary tool in a basic infertility workup. JSLS 10(2): 231-235.
-
Taylor PJ, Lewinthal D, Leader A, Pattinson HA (1987) A comparison of Dextran 70 with carbon dioxide as the distention medium for hysteroscopy in patients with infertility or requesting reversal of a prior tubal sterilization. Fertility and Sterility 47(5): 861-863.
-
Magos A, Al-Khouri A, Scott P, Taylor A, Sharma M, et al. (2005) One stop fertility clinic. Journal of Obstetrics and Gynaecology 25(2): 153-159.
-
La Sala GB, Montanari R, Dessanti L, Cigarini C, Sartori F (1998) The role of diagnostic hysteroscopy and endometrial biopsy in assisted reproductive technologies. Fertility and Sterility 70(2): 378-380.
-
Shokeir TA, Shalan HM, El-Shafei MM (2004) Combined diagnostic approach of laparoscopy and hysteroscopy in the evaluation of female infertility: results of 612 patients. Journal of Obstetrics and Gynaecology Research 30(1): 9-14.
-
Campo R, Van Belle Y, Rombauts L, Brosens I, Gordts S (1999) Office mini-hysteroscopy. Human Reproduction Update 5(1): 73-81.
-
Silberstein T, Saphier O, van Voorhis BJ, Plosker SM (2006) Endometrial polyps in reproductive-age fertile and infertile women. Israel Medical Association Journal 8(3): 192-195.
-
Martin K, Jean-Luc M, Chadi Y, Serge U, Jacky N (2010) Office Hysteroscopy for Infertility: A Series of 557 Consecutive Cases. Obstet Gynecol Int 2010: 168096.
-
Seyam EM, Hassan MM, Mohamed Sayed Gad MT, Mahmoud HS, Ibrahim MG (2015) Pregnancy Outcome after Office Microhysteroscopy in Women with Unexplained Infertility. Int J Fertil Steril 9(2): 168-175.
-
Oliveira FG, Abdelmassih VG, Diamond MP, Dozortsev D, Nagy ZP, et al. (2003) Uterine cavity findings and hysteroscopic interventions in patients undergoing in vitro fertilization-embryo transfer who repeatedly cannot conceive. Fertil Steril 80(6): 1371-1375.
-
Shokeir TA, Shalan H, El-Shafei (2004) Significance of endometrial polyps detected hysteroscopically in eumenorrheic infertile women. J Obstet Gynaecol Res 30(2): 84-89.
-
Homer HA, Li TC, Cooke ID (2000) The septate uterus: A review of management and reproductive outcome. Fertil Steril 73(1): 1-14.
-
Vollenhoven BJ, Lawrence AS, Healy DL (1990) Uterine fibroids: A clinical review. Br J Obstet Gynaecol 97(4): 285-298.
-
Grimbizis GF, Camus M, Tarlatzis BS, Bontis JN, Devroey P (2001) Clinical implications of uterine malformations and hysteroscopic treatment results. Hum Reprod 7(2): 161-174.
-
Nagele F, O'Connor H, Davies A, Badawy A, Mohamed H, et al. (1996) 2500 outpatient diagnostic hysteroscopies. Obstet Gynecol 88(1): 87-92.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’