The Reduction of Surgical Site Infections in Cesarean Section Deliveries by Implementation of a Surgical Care Pathway
Caesarean section deliveries are an important surgical procedure that is used to improve both maternal and fetal outcomes in complicated pregnancies. In recent times however the convenience of the surgery for both mother and surgeon has resulted in an increasing global trend of C-section deliveries which according to the World Health Organization has now reached pandemic proportions. The nature of the surgery makes it a high risk procedure and the incidence of infection have been increasing in both well and under-resourced countries. Since the entire process is not limited to a single hospital department, a multi-disciplinary approach is needed to minimize the risk of infections. For this study a surgical care pathway was introduced as part of a performance improvement project to a private hospital in South Africa which resulted in C-section infection rates decreasing from 5.12 ± 0.82 % to 0.23 ± 0.15 % (p
Introduction
Caesarean section (CS) deliveries are on the rise not only in high income countries (HIC) but low and middle income countries (LMIC) too. This global trend has now reached “epidemic proportions” according to the 2010 report released by the World Health Organization (WHO) with many countries far exceeding the 15% recommended limit [1]. A cross-sectional survey from 57 LMIC spanning 4 different regions conducted by Benova et al. showed that C-section deliveries accounted for 4% of all deliveries in Sub-Sharan Africa, 23% in North Africa/West Asia/Europe, 10% in South/Southeast Asia and 24% in Latin America & Caribbean [2]. Betran et al. showed that countries with the highest CS rates in each region are as follows: Latin America & Caribbean (Brazil - 55.6% and Dominican Republic - 56.4%), Africa (Egypt -
51.8%), Asia (Iran -47.9% and Turkey - 47.5%), in Europe (Italy - 38.1%), Northern America (United States -32.8%) and Oceania (New Zealand -33.4%) [3]. In both studies it was shown that rate of CS deliveries were significantly higher in the private sector compared to public sector health care facilities. In South Africa, the overall national CS rate is 22.7% in district hospitals [4] however many public hospitals far exceed the national average, with one district hospital even reporting a 42.4% rate of CS deliveries [5]. The figures released by the South African Council for Medical Schemes however show a very different picture in that almost 70% of all births in the private hospital sector are by means of CS deliveries with some hospitals having up to a 90% CS delivery rate [6]. Like many countries across the world these elective CS deliveries are based on convenience rather than medical necessity. Besides the huge cost implications, CS rates are also associated with significant perinatal and maternal morbidity and mortality. A significant portion of maternal morbidity and mortality is attributed to surgical site infections (SSI). Although credible data on SSI associated with CS deliveries are lacking, the 2011 WHO bulletin showed that approximately 38% of obstetrics & gynaecology procedures are complicated by infections in Africa [7]. A multi-country study conducted in Sub-Saharan Africa reported a 7.3% incidence of SSI’s during CS deliveries [8] while Jjuuko and Moodley (2002) showed that abdominal wound sepsis was 11.9% at a district hospital in South Africa [9]. According to the Centers for disease control and prevention (CDC), as surgical site infection is described as an infection that manifests in that part of the body undergoing an invasive surgical procedure and may occur with 30 days post-operatively or up to 1 year later in the case of an implant [10]. The CDC further classifies SSI’s as follows. Superficial SSI’s are when an infection occurs within 30 days of the surgical procedure and is confined to the skin and superficial layers around the incision [10]. A deep SSI either occurs within 30 days if no implant is in situ or within a year with implant related surgery and manifests in the deep tissues of the incision [10]. An organ space SSI also occurs within 30 days if no implant is used or within a year for implant surgery and affects any anatomical site other than the incision which was opened or manipulated during the procedure [10].
The study in Sub-Saharan Africa from Doctors without Borders (Medicine’s Sans Frontiers) reported that the median length of stay in hospital, for women undergoing a CS delivery without SSI was 7 days compared to 21 days for those women that acquired an SSI (p < 0.001) [8]. These extended lengths of stay have significant financial impacts on both the patient and the hospital. In the public sector, most of the cost of an infection is absorbed by the hospital itself and the increased bed-days also means decreased throughput and more pressure on the hospital because of the growing patient base. In the private sector, on the other hand, patients are billed for an infection but medical insurance funders are becoming more reluctant to pay for hospital acquired infections resulting in a rise of medical malpractice lawsuits. All in the entire patient and the hospital faces a huge financial liability with the incidence of an SSI. The purpose of this study was to reduce the burden of SSI at a private hospital in South Africa by implementing a performance improvement project.
Methods
Auditing of the Existing Surgical Process
During week one (August 2015), five elective C-section procedures were audited without any interference. The aim was to identify whether the guidelines and protocols for minimizing SSI’s as recommended by the CDC (1999) were followed by the medical team [10]. The audit was performed by means of a modified checklist, adapted from the “Guidelines to prevent SSI’s, 1999”. Each of the five patient’s surgical journey was monitored from admission to discharge and compared to the recommendations of the CDC [10]. The observations were made pre-operatively for compliance with hand hygiene practices, preoperative antiseptic showering, preoperative hair removal, blood glucose control and antimicrobial prophylaxis. During the intraoperative phase, observations focused on patient skin preparation in the operating room, the control of the operating room environment, the surgical attire and drapes used, verification on the sterility of the surgical instruments and supplies, aseptic techniques and the surgical technique. In the post-operative phrase the maintenance of normothermia and wound management was observed. Adherence to the recommended practices were scored between 0 & 4 where 0 indicated non-compliance, 1 indicated slight compliance, 2 indicated average compliance, 3 indicated almost compliant and 4 indicated compliant. The compliance percentage was calculated as the (Hospital Score / Maximum Score) x 100. All
processes with a percentage of 50 % and below were chosen as areas for improvement.
Performance Improvement Protocol
Following an audit of the existing surgical process, the key areas for improvement were identified. A report was generated to address and discuss the areas of concerns with the infection control team. The team included the infection control manager, the clinical facilitator, the operating room manager, central services and sterilization department supervisor and the maternity ward manager. Emphases for performance improvement were driven by quality education programs by means of lectures, hands on practical work and online programs. The entire medical team associated with the C-section procedure including the ward nurses, theatre nurses, CSSD operatives and surgeons were encouraged to participate in the program. These education modules enabled us to map out the patients journey and highlight the key areas for possible infections. Improvements of these areas were enforced by means of a check list that accompanied the patient from admission to discharge.
Sample Population
All women undergoing both emergency and elective CS deliveries, between 1 September 2015and 31 August 2016 were considered for this study (n=566).
Identification of a Surgical Site Infection.
Figure 1 represents the results from the audit of the surgical process before the implementation of the performance improvement project. The hospital scored >50% in 13 of the 20 areas of concern along the patient’s surgical pathway. The 7 areas that scored below 50% were as follows: pre-warming (25%), hair removal (35%), verification of instrument sterility (45%), traffic control (45%), patient skin preparation (50%), postoperative glucose control (50%) and post-operative wound management (50%).
All the SSIs were identified by surgeons, using the Centre’s for Disease Control and Prevention (CDC) standardized criteria [11]. SSIs are classified as incisional or organ/space. Incisional SSIs are divided into those involving skin and subcutaneous tissue (superficial incisional) and those involving deeper soft tissue of surgical incision (deep incisional SSIs). Organ/space SSIs involve any part of the anatomy other than incised body wall layers that were opened or manipulated during an operation.
Retrospective Data Collection
Retrospective data on CS deliveries conducted at Louis Pasteur Private Hospital was obtained from the hospital’s infection control manager. The data included all women undergoing CS deliveries from January 2015 to August 2015. The information was kept anonymous and only included the age of the patient, the SSI rate and the type of microbe that was cultured from the septic surgical site. The age of the patients are expressed as the mean ± SEM. The rate of SSI is calculated as follows: (number of SSI per month / number of CS deliveries per month) X 100.
Statistical Analysis
All data was subjected to statistical analysis using the GraphPad Instat stasistical software package (V.06).
Ethical Considerations
Ethical approval was obtained from the hospital’s clinical education department. All patient information remained anonymous throughout the duration of the study.
Results
Audit of the Existing Surgical Process
0 10 20 30 40 50 60 70 80 90 100
Percentage (%)
Retrospective Data Collection
Figure 2 represents the rate of SSI versus CS deliveries at Louis Pasteur Private Hospital between January 2015 and August 2015. The data was collected from 566
Implementation of the Performance Improvement Protocol
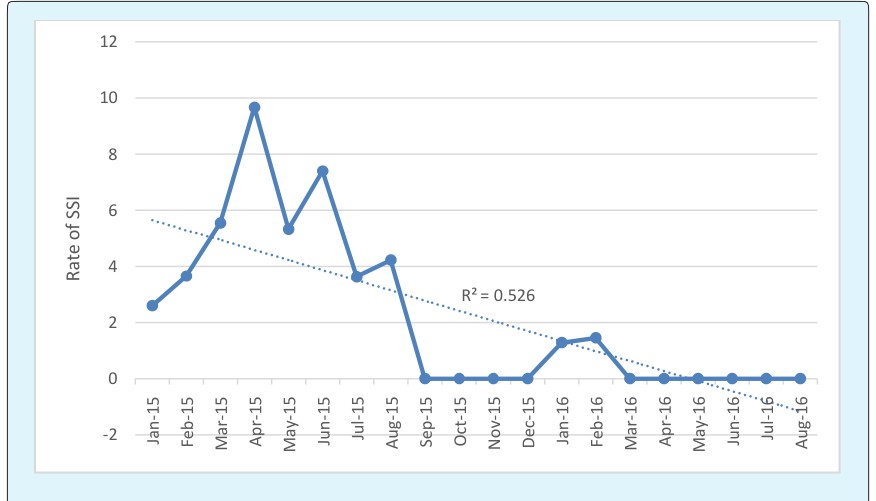
Preoperative Hair Removal: All women undergoing elective CS deliveries were advised not to remove their own pubic hair at home. Hair removal was performed by trained personnel at Louis Pasteur private hospital using an electric clipper (3M Surgical Clippers, St Paul, Minnesota). Hair removal was performed on the day of surgery, outside of the operating room as recommended by the CDC (1999). Patient Skin Preparation: The surgical skin preparation regime was changed from prepping with a CHG-alcohol combination (HIBISCRUB® cutaneous solution, BCM Ltd, UK - chlorhexidine gluconate 4% w/v (40mg/ml) as chlorhexidine digluconate solution; isopropyl alcohol) to an iodine povacrylex-alcohol solution (DuraPrepTM, 3M, St. Paul, Minnesota - Iodine povacrylex [0.7% available Iodine]; 74% isopropyl alcohol w/w). Iodine povacrylex has previously been reported to dry up to form a water- insoluble film on the surface of the patient’s skin hence resisting fluid wash-off by irrigating solutions and body fluids [12]. In addition it has also been shown to provide continuous antimicrobial protection for up to 48 hours post-application under suitable wound dressing [13]. Theatre staff was given comprehensive training on the application of the solution according to the AORN guidelines for the “paint-on” technique on a distended abdomen. Operating Room Traffic Control: The number of individuals allowed into the operating room was kept to a minimum. No disturbances were entertained by the surgical team for the duration of the procedure. Verification of Instrument Sterility: This was a collaborative effort involving the central services and sterilization department (CSSD) and the theatre staff. The CSSD staffs were educated on the necessity to include a chemical indicator (ComplyTM Chemical Integrator, 3M - St Paul, Minnesota) in every pack that was to be used for the CS delivery. The theatre staffs were trained not to accept any surgical pack without the accompaniment of this chemical indicator. This was done in accordance with the WHO surgical safety checklist and performed during the “time-out” phase The chemical indicator was then attached to the patients file for record purposes. Postoperative Glucose Control: A postoperative blood glucose level was routinely monitored for 24 hours with blood glucose strips and a glucometer (Accucheck Active, Roche Diagnostics, Indiana, USA). Intensive glycemic control was maintained in patients with diabetes mellitus and postoperative hyperglycemia with a target blood glucose of <139 mL/dL [14] however a range of 108 -180 mg/dL was excepted [15]. Postoperative wound Management: The postoperative wound dressing regimen was improved by the introduction of a unique all-in-one sterile dressing (3M™ Tegaderm plus pad) which is a non-adherent absorbent pad, centred on a breathable film that only requires changing when clinically indicated or every 3rd day as per the product recommendation. This dressing provides a bacterial and viral barrier thus preventing external contaminants from entering the site. Staff and patient education was continuously provided to prevent the unnecessary changing of dressings and wound exposure. Number of SSI after Implementation of the Performance Improvement Protocol: The performance improvement protocol was initiated on the 1st of August 2015. The data was collected from 503 patients. Figure 3 represents the number of SSI from January 2015 till August 2016. The graph depicts an immediate decrease in SSI from August 2015 to September 2016 which directly correlates to the implementation of the performance improvement protocol. The trend line shows a sharp decrease in SSI over the test period (R2 = 0.5266). In the pre-performance improvement phase there was a 5.12 ± 0.82 % rate of SSI. In the post-performance improvement phase the rate of SSI significantly decreased to 0.23 ±0.15 % (p<0.0001).The values were subjected to a non- parametric Mann-Whitney two-tailed t test.
Discussion
Caesarean section deliveries are an important surgical procedure that saves millions of lives each year. It is for this reason that it has been recognized by the WHO as one of the 29 recommended surgical procedures that must be accessible to all women irrespective of financial background [1, 8]. Global trends indicate a rise in CS deliveries, with more and more healthy pregnancies opting for elective CS deliveries. Since it is a major, invasive surgical procedure the risk for developing an SSI is great. The incidence of SSI at Louis Pasteur Private Hospital during CS deliveries was on the rise. In light of this, a drastic intervention program was needed to curb the increase. The intervention involved an audit of their existing surgical protocol using a modified checklist as recommended by the CDC (1999). Studies show that the biggest source of microorganisms capable of producing an SSI comes from the patient’s own skin [16]. It was reported that approximately 60% of all SSI’s is caused by the patient’s own skin flora. The next biggest source of microorganisms come from the hospital staff and is responsible for approximately 30% of all SSI’s. Lastly, the contaminant in the air is responsible for approximately 10% of all SSI’s. It is no wonder that most of the interventions aimed at reducing SSI’s as prescribed by the CDC focuses on protecting the patient from their own flora, followed by minimizing bacterial transmission from the medical staff to the patient and finally an emphasis on air quality in the operating room. From the audit 7 areas of the patient’s surgical pathway required intervention. The 7 areas that scored below 50% were as follows: pre-warming the patient (25%), hair removal (35%), verification of instrument sterility (45%), traffic control (45%), patient skin preparation (50%), post-operative glucose control (50%) and post-operative wound management (50%). In most of the elective CS cases observed at Louis Pasteur Private Hospital, the women opted to remove their own pubic hair at home. It is reasonable to assume that many of them removed hair by shaving with a razor blade although others could have possibly used depilatory creams. In the emergency CS cases hair removal was done inside the operating room with the use of a razor blade. Although pubic hair removal is not totally necessary when making a pfannenstiel cut, its close proximity to the incision site often warrants removal. The 2011 Cochrane review of preoperative hair removal reported that patients are at an increased risk for developing a postoperative infection when shaving with a razor [17].
The report included three trials which all conclusively showed an increased risk of SSI when hair was shaved as opposed to clipped (RR 2.09; 95% CI, 1.15-3.80) [17]. The risk for infection is attributed to microscopic epidermal injuries that are caused by shaving which either acts as a portal of entry for transient skin flora or serve as an ideal incubator for bacterial growth. For this reason, if hair removal is deemed necessary immediately prior to surgery, the use of clippers is preferred over’s having. Since there is compelling evidence to suggest an increased risk of SSI when shaving with a razor, in all elective CS cases, the women were advised not to remove pubic hair at home. They were reassured that there are qualified nursing personnel trained for proper hair removal with electrical clippers (3M Surgical Clippers, St Paul, MN). Human skin is densely populated with bacteria. It is documented that skin bacterial density can range anywhere from 100 to 100000 microorganisms per square centimeter. Skin bacterial density has been shown to be the highest in the axilla, inguinal fold and the perineum. Patient skin preparation is therefore an age old technique for reducing the incidence of infections by reducing skin bacterial density. The FDA recommends that any prepping solution must cause a 2-3 log reduction in skin flora in order to be effective. Unfortunately most skin preparations cannot resist fluid wash-off nor do they have a persistent antimicrobial activity. Since logarithmic reduction of bacteria is a time-related event, the decreased contact time between the solution and the skin minimizes the antimicrobial effect. Recent reports show that pooling of CHG-alcohol solutions is associated with perineal chemical burns and is not recommended for prepping epithelial linings. Hence iodine based solutions are preferred for C-Section deliveries [12, 13]. Unfortunately not all iodine based solutions are the same. Both aqueous and alcoholic preparations are easily washed off especially if they are not allowed the maximum drying time. Iodine povacrylex however, is a unique polymer coupled to iodine which optimizes its effect by drying up to form a water-insoluble on the surface of the patient’s skin. This film resists fluid wash-off and therefore provides antimicrobial protection for the duration of the surgical procedure and even up to 48 hours under a suitable dressing. Due to the nature of a CS procedure especially with the large amount of fluids, either amniotic or irrigation solutions and the incisions site’s close proximity to the inguinal folds and perineum which are densely populated with microorganisms, this ranked as one of the greatest improvements to their protocol. Contaminated instruments are a major risk factor for SSI. Even if the surgical team adheres to all the recommended protocols with strict compliance, if the instruments used for the procedure is contaminated then the patients risk for an SSI escalates exponentially. Instrument decontamination and device reprocessing has therefore been identified as a major arm of the infection prevention pathway. International infection prevention organizations emphasize the need for a scientific approach towards sterilization of medical equipment with strict measures to ensure quality assurance of these instruments. During the time-out phase of the WHO Surgical Safety Checklist there is a question addressed to the nursing team regarding whether the sterility of the instruments have been verified by means of a chemical indicator. A “passed” chemical indicator provides the surgical team with confidence that the instruments are sterile and therefore eliminates a major component from the root causes of an SSI. Preoperative hypoglycemia and postoperative hyperglycemia are both associated with increased risk for developing SSI during surgery. Hypoglycemia is associated with decreased immunity whereas hyperglycemia has been shown to cause inflammation, oxidative stress, endothelial dysfunction and tissue ischemia [18]. The postoperative range for blood glucose in a non-diabetic patient is 6-10 mM (108 -180 mg/dl) [15]. Since there is strong evidence pointing towards a correlation between postoperative hyperglycemia and SSI, patient’s blood glucose levels were taken every hour post-surgery for the first 12 hours and every 3 hours thereafter for the next 12 hours. Hyperglycemic patients were given metformin as per the doctor’s instruction when blood glucose levels exceeded the tolerable limit. Post-operative wound management also contributes to SSI reduction. The less interference with the wound post operatively the less likelihood there is of infection. It is therefore imperative that an appropriate wound dressing be applied to the wound after suturing. The makings of a good dressing are that they are hypoallergenic, non-toxic and breathable. It must also allow for the quick evaporation of moisture, the absorption of exudates and most importantly have good adhesion to the skin. This will allow the dressing to remain on the skin for 7-10 days post incision. In South Africa, traditional herbal remedies still form an integral part of the indigenous culture and often herbal decoctions are applied to the wound to “accelerate” healing. The disadvantage is that if they are not prepared aseptically, then it too can be a source of infection. Patient education and the use of superior wound dressings played a huge role towards minimizing this threat of infection. The performance improvement project caused the infection rate to decrease from 5.12 ± 0.82 % to 0.23 ± 0.15 % (p<0.0001). It is interesting to note that the 2 infections reported post PIP were a hematoma and the other was as a result of secondary suturing. In essence they are not classified as SSI’s. These results may be slightly obscured as not all patients were able to be contacted 30 days post-surgery however this number is rather miniscule.
Conclusion
The significant decrease in SSI’s during CS deliveries at Louis Pasteur Private Hospital as a result of implementing a surgical care pathway bares testimony to the fact the HAI’s can be reduced through a conscious effort made by the hospital and its staff. The exceptional result obtained from this performance improvement project certainly warrants the investigation of implementing similar surgical care pathways in other disciplines of surgery to help reduce the incidence of SSI’s.
References
-
World Health Organization (2010) World health statistics 2010. WHO Library Cataloguing-in- Publication Data.
-
Benova L, Macleod D, Footman K, Cavallaro F, Lynch CA (2105) Role of the private sector in childbirth care: cross-sectional survey evidence from 57 low- and middle-income countries using Demographic and Health Surveys. Tropical Medicine and International Health 20(12): 1657-1673.
-
Betrán AP, Ye J, Moller AB, Zhang J, Gülmezoglu AM, et al. (2016) The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990- 2014. PLoS ONE 11(2): e0148343.
-
Massyn N, Peer N, Padarath A, Barron P, Day C (2015) District Health Barometer 2014/15. Durban: Health Systems Trust.
-
Makhanya V, Govender L, Moodley J (2015) Utility of the Robson Ten Group Classification System to determine appropriateness of caesarean section at a rural regional hospital in KwaZulu-Natal, South Africa. S Afr Med J 105(4): 292-295.
-
Smith (2014) The guardian.
-
Bagheri Nejad S, Allegranzi B, Syed SB, Ellis B, Pittet D (2011) Health-care-associated infection in Africa: a systematic review Bull World Health Organ 89(10): 757-765.
-
Chu K, Maine R, Trelles M (2015) Cesarean Section Surgical Site Infections in Sub-Saharan Africa: A Multi-Country Study from Medecins Sans Frontieres. World J Surg 39(2): 350-355.
-
Jjuuko G, Moodley (2002) Abdominal wound sepsis associated with gynaecological surgery at King Edward VIII Hospital, Durban. S Afr J Surg 40(1): 11- 14.
-
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR (1999) Guideline for the prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infection control & Hospital epidemiology 20(4): 250-278.
-
Horan TC, Andrus M, Dudeck MA (2008) CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 36(5): 309- 332.
-
Hemani ML, Lepor H (2009) Skin Preparation for the Prevention of Surgical Site Infection: Which Agent Is Best? Rev Urol 11(4): 190-195.
-
Reichman DE, Greenberg JA (2009) Reducing Surgical Site Infections: A Review. Rev Obstet Gynecol 2(4): 212-221.
-
Al-Niaimi AN, Ahmed M, Burish N, Chackmakchy SA, Seo S, et al. (2015) Intensive postoperative glucose control reduces the surgical site infection rates in gynecologic oncology patients. Gynecol Oncol 136(1): 71-76.
-
Sebranek JJ, Lugli AK, Coursin DB (2013) Glycaemic control in the perioperative period. British Journal of Anaesthesia 111(S1): i18-i34.
-
Garvin KL, Urban JA (2003) Total hip infections in Musculoskeletal Infections. J Hos Infect pp: 241-293.
-
Tanner J, Norrie P, Melen K (2011) Preoperative hair removal to reduce surgical site infection. Cochrane Database Syst Rev 11: CD004122.
-
Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP, et al. (2004) Management of diabetes and hyperglycemia in hospitals. Diabetes Care 27(2): 553- 591.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’