Transvaginal Sonography in Unexplained Infertility: A Study
Introduction: Infertility is a devastating disease. Its victims are affected at a very basic level, the ability to reproduce, to leave a legacy. This can be divisive to the couple involved, their relatives and friends. The sphere of influence this disease has can be immense. Attendant to the medical consequences of infertility are the psychological sequelae. Afflicted patients and their families can suffer loss of esteem, disappointment and depression. Aim of the Study: To determine the applicability of uterine biophysical profile (UBP) scoring by transvaginal sonography with chances of pregnancy in a cohort of females with unexplained infertility. Also to determine the applicability of individual parameters in predicting a positive pregnancy outcome. Materials and Methods: This prospective observational study was conducted at department of radiodiagnosis, g r medical college and J A group of hospitals during the period of 2015 to 2016. The study subjects included 50 infertile females (primary /secondary infertility) in the age group of 20-40 years. Results and conclusion: By predicting the positive pregnancy outcome, the possible advantages are medical, psychological, economical and emotional. With available previous studies, we also analysed the uterine biophysical profile by transvaginal Sonography in the patients, to predict the outcome.
Som Biswas1* and Srirupa Biswas2
GRMC, Gwalior, India, Email: somviswas1@gmail.com
has can be immense.
can suffer loss of esteem, disappointment and depression.
individual parameters in predicting a positive pregnancy outcome.
females (primary /secondary infertility) in the age group of 20-40 years.
profile by transvaginal Sonography in the patients, to predict the outcome.
Equipments; Endometrial; Myometrial
Introduction
Infertility is a devastating disease. Its victims are affected at a very basic level, the ability to reproduce, to leave a legacy. This can be divisive to the couple involved, their relatives and friends. The sphere of influence this disease has can be immense. Attendant to the medical consequences of infertility are the psychological sequelae. Afflicted patients and their families can suffer loss of esteem, disappointment and depression.
Aim of the Study
To determine the applicability of uterine biophysical profile (UBP) scoring by transvaginal sonography with chances of pregnancy in a cohort of females with unexplained infertility. Also to determine the applicability of individual parameters in predicting a positive pregnancy outcome.
Materials and Methods
This prospective observational study was conducted at department of radio diagnosis; g r medical college and J A group of hospitals during the period of 2015 to 2016. The study subjects included 50 infertile females (primary /secondary infertility) in the age group of 20-40 years, primarily referred for follicle maturation monitoring by transvaginal ultrasound (with color and pulsed Doppler) with patent tubes and normal utero-ovarian morphology. Male factor infertility was also excluded. The UBP was determined by applying the uterine scoring system for reproduction (USSR). A score of 16 or above, out of a perfect score of 20, was hypothesized to be favorable for pregnancy. Frequency of pregnancy was correlated with the cumulative score as well as individual variable. Significance of correlation was taken as p<0.05.
Exclusion Criteria:
- Congenital anomalies of Uterus
- Uterine masses
- Abnormal ovarian cycles.
Inclusion Criteria:
• Primary and secondary infertility
Ultrasound Equipments:
- ALOKA prosound SSD-4000 SV.
- Toshiba colour Doppler usg SSA 350 A/31 nemio 30. with 6-
- 12 MHz TVS probe and 3-5 MHz curvilinear probe
- No. of cases 50
Ultrasound Technique Unique to the Uterine Biophysical Profile
To perform the UBP special care should be taken. The following guidelines are recommended:
- To determine the presence of a 5-line appearance, information from both the transabdominal and transvaginal studies may be useful. In this case, a 5-line appearance is considered to be present and endometrial vascular penetration may be estimated when performing the endovaginal study.
- Perform the Doppler study slowly. The flow of blood in the endometrium is of low velocity. It may take time for the ultrasound machine to register the presence of blood flow and create the image. If one sweeps through the endometrium too quickly, flow may not be seen.
- Endeavor to make the endometrium as specular a reflector as possible. Use the techniques of manual manipulation of the anatomy and probe pressure to achieve this.
- Scan endovaginally both coronally and sagittally. There may be a difference in how well the blood flow is imaged.
- When measuring the endometrium in the A-P dimension, try to obtain the value when no contraction affecting it is present. Contractions may alter this value. Also, when possible, obtain the measurement in a standard plane such as when both the endometrial and cervical canals appear continuous.
The Uterine Scoring System for Reproduction ("USSR") comprises evaluation of the following parameters [1, 2, 3, 4, 5]:
- Endometrial thickness (full-thickness measured from the myometrial-endometrial junction to the endometrial- myometrial junction)
- Endometrial layering (i.e., a 5-line appearance)
- Myometrial contractions (seen as endometrial motion)
- Myometrial echogenicity
- Uterine artery Doppler flow evaluation
- Endometrial blood flow
- gray-scale myometrial blood flow
Each parameter is scored as follows:
- Endometrial Thickness
- Endometrial thickness is the maximum distance between the echogenic myoendometrial interfaces measured in long axis
- To avoid the variability in measurements by 1-2 mm due to uterine contractions which peaks during the periovulatory phase, it is advised to perform several measurements
- When present endometrial fluid should be excluded from the endometrial measurement.
- Obtain the measurement in a std. plane when both the endometrial and cervical canals appear continuous A. < 7 mm = 0 B. 7 - 9 mm = 2 C. 10 - 14 mm = 3 D. > 14 mm = 1
Endometrial Layering
A. no layering = 0 B. hazy 5-line appearance = 1 C. distinct 5-line appearance = 3
- Myometrial Contractions (Seen as Wave-Like Endometrial Motion) The inner third of myometrium demonstrates a subtle contractile pattern best appreciated in a magnified mid saggital view. The contractions propagate from the internal cervical os towards the uterine fundus. A. < 3 contractions in 2 minutes (real-time) = 0 B. > 3 contractions in 2 minutes (real-time) = 3
- Myometrial Echogenicity A. coarse/inhomogeneous echogenicity = 1 B. relatively homogeneous echogenicity = 2
- Uterine artery Doppler Flow Evaluation Uterine artery is demonstrated laterally to the cervix at the level of cervico corporeal junction. An elevated PI > 2.5, an absent end diastolic flow is considered as an abnormal waveform. A. PI > 3.0 = 0 B. PI< 2.5 - 2.99 = 0 C. PI < 2.2 - 2.49 = 1 D. PI < 2.19 = 2
- Endometrial Blood Flow within Zone 3 Zones of Vascular Penetration
- Zone 1 - A 2 mm thick area surrounding the hyperechoic outer layer of the endometrium
- Zone 2 - The hyperechoic outer layer of the endometrium
- Zone 3 - The hypoechoic inner layer of the endometrium
- Zone 4 - The endometrial cavity Power Doppler is preferable for 2 reasons
- To detect signal from vessels with low velocity blood flow
- To avoid signal loss due to 90 degree angle incidence of the ultrasound beam , that occurs with conventional colour Doppler. A. absent = 0 B. present, but sparse = 2 C. present multifocally = 5
- Myometrial Blood Flow Internal to the Arcuate Vessels Seen on Gray-Scale Examination A. absent = 0 B. present = 2
Statistical Tools
The information collected regarding all the selected cases were recorded in a Master Chart. Data analysis was done with the help of computer using Epidemiological Information Package (EPI 2002). Using this software, range, frequencies, percentages, means, standard deviations, chi square and ‘p’ values were calculated. Kruskul Wallis chi-square test was used to test the significance of difference between quantitative variables and Yate’s test for qualitative variables. A 'p' value less than 0.05 is taken to denote significant relationship.
Results and Analysis
| Cases | ||
|---|---|---|
| Age in Years | No. | % |
| Up to 25 yrs | 9 | 18 |
| 26-30 | 10 | 20 |
| 31-35 | 20 | 40 |
| 36-40 | 9 | 18 |
| >40 | 2 | 4 |
| Range | 23-42 yrs | |
| Mean | 32 yrs | |
| S.D. | 5.07 yrs | |
Table 1: Age distribution.
| Variables | Range | Mean | SD |
|---|---|---|---|
| Endometrial Thickness (in mm) | 5-18 | 8.63 | 2.65 |
| Uterine artery PI | 1.5-3.6 | 2.61 | 0.39 |
| UBP Score | 5-18 | 12.64 | 3.34 |
Table 2: Quantitative Variables.
| Cases | Endometrial Thickness (mm) | |||
|---|---|---|---|---|
| Variables | No | Mean | SD | |
| % | ||||
| Endometrial Layering | ||||
| Hazy 5 line | 13 | 26 | 8.78 | 2.19 |
| Distinct 5 line | 36 | 72 | 8.58 | 2.83 |
| No layering | 1 | 2 | 0.81 (Not significant) | |
| Endometrial Contractions | ||||
| <3 in 2 minutes | 17 | 34 | ||
| >3 in 2 minutes | 33 | 66 | ||
| Myometrial Echoes | ||||
| Coarse | 27 | 54 | ||
| Heterogeneous | 4 | 8 | ||
| Homogenous | 19 | 38 | ||
| Zone 3 Sub endometrial | ||||
| Absent | 6 | 12 | ||
| Sparse | 30 | 60 | ||
| Multi focal | 14 | 28 | ||
| Myometrial flow | ||||
| Present | 41 | 82 | ||
| Absent | 9 | 18 | ||
| Pregnancy | ||||
| Positive | 14 | 28 | ||
| Negative | 36 | 72 | ||
| Pregnancy Outcome | Positive | Negative | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age group | Positive | Negative | No. | % | No. | % | |||||
| No. | % | No. | % | ||||||||
| Endometrial Contractions | Pregnancy Outcome | Pregnancy Outcome | |||||||||
| Positive | Negative | Positive | Negative | ||||||||
| No | % | No | % | No | % | No | % | ||||
| Age group | Upto 25 yrs (9) | 3 | No. | % | No. | % | 33.3 | 6 | 66.7 | ||
| 26-30 (10) | 1 | 10 | 9 | 90 | |||||||
| 31-35 (20) | 7 | 35 | 14 | 64.3 | |||||||
| 36-40 (9) | 3 | 33.3 | 6 | 66.7 | |||||||
| >40 (2) | - | - | 2 | 100 | |||||||
| Mean | 31.7 yrs | 31.53 yrs | |||||||||
| SD | 5.2 yrs | 5.1 yrs | |||||||||
| ‘p’ | 0.9115 (Not significant) | ||||||||||
| <3 in 2 minutes (17) | 3 | 17.65 | 14 | 82.35 | 14 | 33.33 | 28 | 66.67 | |||
| >3 in 2 minutes (33) | 11 | 33 | 22 | 67 | - | - | 8 | 100 | |||
Table 7: Age and pregnancy outcome.
| Cases | Endometrial Thickness (mm) | |||
|---|---|---|---|---|
| Variables | No | % | Mean | SD |
| Endometrial Layering | ||||
| Hazy 5 line | 13 | 26 | 8.78 | 2.19 |
| Distinct 5 line | 36 | 72 | 8.58 | 2.83 |
| No layering | 1 | 2 | 0.81 (Not significant) | |
| Endometrial Contractions | ||||
Table 4: Endometrial Thickness and pregnancy outcome.
| 19 | 38 | |
|---|---|---|
| Zone 3 Sub endometrial | ||
| Absent | 6 | 12 |
| Sparse | 30 | 60 |
| Multi focal | 14 | 28 |
| Myometrial flow | ||
| Present | 41 | 82 |
| Absent | 9 | 18 |
Table 5: Uterine artery PI and pregnancy outcome.
| Endometrial Layering | Pregnancy Outcome | |||
|---|---|---|---|---|
| Positive | Negative | |||
| No. | % | No. | % | |
| Hazy 5 line (13) | 3 | 23 | 10 | 77 |
| Distinct 5 line (36) | 11 | 30.5 | 25 | 69.4 |
| No layering (1) | - | - | 1 | 100 |
Table 6: Endometrial Layering and pregnancy outcome.
| Pregnancy Outcome | ||||
|---|---|---|---|---|
| Myometrial Echoes | Positive | Negative | ||
| No | % | No | % | |
| Myometrial Echoes | 4 | 14.8 | 23 | 85.2 |
| Coarse (27) | 4 | 14.8 | 23 | 85.2 |
| Heterogeneous (4) | 1 | 25 | 3 | 75 |
| Homogenous (19) | 9 | 47 | 10 | 53 |
Table 10: Myometrial echoes and pregnancy outcome.
| Pregnancy Outcome | Pregnancy Outcome | |||||||
|---|---|---|---|---|---|---|---|---|
| Endometrial Contractions | Positive | Negative | Positive | Negative | ||||
| No | % | No | % | No | % | No | % | |
| Endometrial Contractions | ||||||||
| <3 in 2 minutes (17) | 3 | 17.65 | 14 | 82.35 | 14 | 33.33 | 28 | 66.67 |
| Absent (8) | 11 | 33 | 22 | 67 | - | - | 8 | 100 |
Table11: Myometrial flow and pregnancy outcome. Out of 50 patients, 42 patients found to have adequate myometrial flow and 8 patients show absent flow. But only 14 patients with myometrial flow were pregnancy positive (33.33%). Rest was pregnancy negative.
| Pregnancy Outcome | Uterine Biophysical Profile Score | |||
|---|---|---|---|---|
| Myometrial Echoes | Pregnancy Outcome | Mean | SD | |
| Positive | Negative | |||
| Myometrial Echoes | Positive | Negative | 10.97 | 2.24 |
| 0.000017 (Significant) | ||||
Table 9: Uterine Biophysical Profile Score and Pregnancy outcome Out of 50 patients, scores range from 5 to 18.
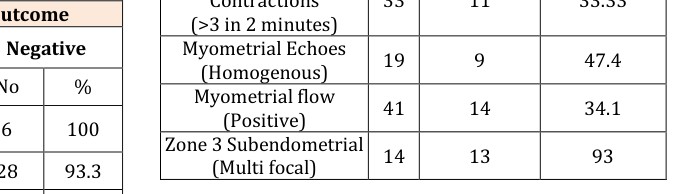
Table 10: Zone 3 Sub endometrial flow and pregnancy outcome. Out of 50 patients, 14 patients had multi focal subendometrial flow (zone 3) of which 13 patients (93%) was pregnancy positive. One patient was negative. 30 patients had very sparse subendometrial flow. 28 patients (93.3%) were pregnancy negative. But 2 patients turned out to be pregnancy positive (6.6%).
- Incidence among Positive
- Pregnancy Outcome Cases
- Uterine Biophysical
- Total cases
- Feature
- Cases
- %
- Endometrial Layering (Distinct 5 line)
- 36
- 11
- 30.55
- Endometrial
- Contractions
- (>3 in 2 minutes)
- 33
- 11
- 33.33
- Myometrial Echoes (Homogenous)
- 19
- 9
- 47.4
- Myometrial flow (Positive)
- 41
- 14
- 34.1
- Zone 3 Subendometrial (Multi focal)
- 14
- 13
- 93
Table 11: Incidence among positive pregnancy outcome
Our study group comprises of 50 patients (n: 50) All of them were being investigated for either primary / secondary infertility. All of them were subjected to transvaginal Sonography to assess the uterine biophysical profile; including myometrial and endometrial characterization (endometrial receptivity).
| Pregnancy Outcome | |||||||
|---|---|---|---|---|---|---|---|
| Zone 3 Sub Endometrial Flo | w | Positive | Negative | ||||
| No | % | No | % | ||||
| Absent (6) | - | - | 6 | 100 | |||
| Sparse (30) | 2 | 6.6 | 28 | 93.3 | |||
| Multifocal (14) | 13 | 92.9 | 1 | 7.1 |
Various studies are available in which various individual parameters (myometrial and endometrial characteristics) are analyzed in the prediction of pregnancy outcome in terms of positive pregnancy rates. We also tried to analyse the uterine biophysical profile in predicting positive pregnancy outcome. In our study, out of 50 patients, 14 patients (28%) were pregnancy positive and 36 patients (72%) were pregnancy negative. There is significant decline in human fecundity with advancing age noted.
**Summary and Conclusion**
By predicting the positive pregnancy outcome, the possible advantages are medical, psychological, economical and emotional. With available previous studies, we also analysed the uterine biophysical profile by transvaginal Sonography in the patients, to predict the outcome. We analyzed various parameters. viz. Endometrial thickness, endometrial layering, endometrial contractions, uterine myometrial echoes, uterine artery PI, subendometrial flow, and myometrial flow and scores given for each parameter.
In our study, we concluded that endometrial thickness between 6 to 11mm and distinct 5 line endometrial layering improves the pregnancy rates. Patients with Endometrial thickness < 6 mm are less likely to become pregnant. 33 % of patients in pregnant group had endometrial contractions > 3 in 2 minutes. But Rest of the patients with contractions > 3 in 2mnts was pregnancy negative. Hence we conclude that endometrial contractions (> 3 in 2mnts) towards fundus improve the implantation rate.
We also conclude that myometrial echoes and uterine artery PI has no significant correlation in predicting the outcome. More importantly, we found that those patients who have multi focal subendometrial flow (up to zone 3) (93% of patients) have conceived. Those patients with absent subendometrial flow and very sparse subendometrial flow (not up to zone III) didn’t conceive, indicating that subendometrial blood flow has significant role in predicting outcome. This well correlates with other studies. Finally we conclude, that patients with uterine biophysical score more than or equal to 16, are more likely to become pregnancy positive. (P value=0.000017) Those patients with score <16, are less likely to be pregnancy positive.
We conclude that by relying on the above mentioned significant parameters, it is possible to predict the positive pregnancy outcome.
- Multifocal subendometrial flow has got a significant role in implantation.
- Distinct triple layered appearance is associated with good outcome.
- If subendometrial blood flow is detected, the endometrial morphology becomes less important.
- Absent blood flow was associated with failure of conception (P <0.05).
- A high negative predictive value in cases, when there is minimal et.
- Myometrial Echoes and uterine artery Pi has got a less significance in predicting the outcome.
- Endometrial Contractions (> 3 In 2 Mins) towards fundus improve the implantation rate. finally we conclude that patients with uterine biophysical score more than or equal to 16, are more likely to become pregnant (P <0.000017).
- The success rate of various assisted reproduction technologies which are presently low, can go high if the same idea is applied by relying on these parameters.
- Further, if the likelihood of an unsuccessful cycle existed, the patient could be informed prior to the time of aspiration or transfer and the embryos could be returned to a frozen cycle in various assisted reproduction technologies.
**References**
1. Sohail S (2005) The uterine biophysical profile scoring validity. J Coll Physicians Surg Pak 15(9): 556-558.
2. Applebaum M (1995) The uterine biophysical profile. Ultrasound Obstet Gynecol 5(1): 67-68.
3. Ng EH, Chan CC, Tang OS, Yeung WS, Ho PC (2006) The role of endometrial and subendometrial Vascularity measured by three-dimensional power Doppler ultrasound in the prediction of pregnancy during frozen-thawed embryo transfer cycles. Hum Reprod 21(6): 1612-1617.
4. Coulam CB, Bustillo M, Soenksen DM, Britten S (1994) Ultrasonographic predictors of implantation after assisted reproduction. Fertil Steril 62(5): 1004-1010.
5. Zaidi J, Campbell S, Pittrof R, Tan SL (1995) Endometrial thickness, morphology, vascular penetration and velocimetry in predicting implantation in an in vitro fertilization program. Ultrasound Obstet Gynecol 6(3): 191-198.
References
-
Sohail S (2005) The uterine biophysical profile scoring validity. J Coll Physicians Surg Pak 15(9): 556-558.
-
Applebaum M (1995) The uterine biophysical profile. Ultrasound Obstet Gynecol 5(1): 67-68.
-
Ng EH, Chan CC, Tang OS, Yeung WS, Ho PC (2006) The role of endometrial and subendometrial Vascularity measured by three-dimensional power Doppler ultrasound in the prediction of pregnancy during frozen-thawed embryo transfer cycles. Hum Reprod 21(6): 1612-1617.
-
Coulam CB, Bustillo M, Soenksen DM, Britten S (1994) Ultrasonographic predictors of implantation after assisted reproduction. Fertil Steril 62(5): 1004-1010.
-
Zaidi J, Campbell S, Pittrof R, Tan SL (1995) Endometrial thickness, morphology, vascular penetration and velocimetry in predicting implantation in an in vitro fertilization program. Ultrasound Obstet Gynecol 6(3): 191-198.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’