Association of Types of Epithelial Ovarian Cancer with Stage, Cytoreduction and Progression Free Survival Rate
Introduction: To assess the clinical impact of the Types of Epithelial ovarian tumour designated as Type I and II according to Immunohistochemistry and Histopathology to study the association of Types of EOC with stage, cytoreductability and progression free survival rate. Methods: This study was conducted in the Department of Gynaecological oncology, Amrita Institute of Medical Sciences, Kochi, Kerala, India in year 2017–2018 after obtaining the approval of the Institute Ethical Review Board committee. Patients were asked to sign an informed written consent after explaining the need for the procedure, their possible outcomes and the significance of the results. No new intervention was required in this study. All patients with Epithelial ovarian cancer that was surgically treated (Both Primary delbulking and interval debulking surgery) in the Dept. of Gynaecological Oncology were recruited in this study. Intraoperative mapping of pattern of distribution of disease was done and the patients were divided into 3 Groups. Group A (Pelvis, nodes), Group B (omentum, peritoneum, hemidiaphragm, surface liver), Group C (Mesentry, Porta hepatic, Lesser sac). If disease was found to be extensive (Fagotti>8/PCI>17) these patients underwent Neoadjuvant cheomotherapy with Paclitaxil and Carboplatin and then assessed for interval surgery. Residual disease was defined as R0-no residual macroscopic disease after surgery, R1-0.1- 0.5cm residual disease, R2-0.5-1cm, R3>1cm Stages are defined according to the FIGO classification WHO 2014 criteria (I–IV), stage I/II is considered early FIGO stage, and stage III/IV, where the tumor has spread beyond the pelvic region, as late FIGO stage. The categories of grade are well-differentiated (Grade 1) moderately differentiated (Grade 2), and poorly differentiated (Grade 3). Grade 1 is considered as low-grade tumors and Grades 2-3 as high-grade tumors. Histologic types were defined as serous adenocarcinoma, mucinous adenocarcinoma, endometrioid adenocarcinoma, clear cell neoplasms, carcinosarcoma, transitional/Brenner tumors, mixed tumors, or undifferentiated carcinomas along with their IHC markers (p53, WT 1, ER, Napsin) were obtained from their histopathology reports. All pathologic diagnoses were given by our dedicated Onco-pathologists. Kaplan-Meier and logistic/Cox-regression analyses were performed to assess the impact of histological type on surgical outcome and survival. Results: All EOC patients (n=101) reporting to our Dept. of Gynaecological oncology who underwent tumour debulking in our institution (09/2016–012/2018) were classified into one of two groups: type I tumours (n=36); composed of lowgrade serous, low-grade endometrioid, clear cell, mucinous and transitional carcinomas; and Type II tumours (n=65) composed of high-grade serous, high-grade endometrioid, undifferentiated and malignant mixed-mesodermal tumours. Primary debulking surgery rate (PDS) with complete cytoreduction (R0) was more in Type I EOC, with almost 91.2% vs 67.4% in Type II EOC showing clinically and statistical significance (p value.0.016). Also R1/R2 (R1-0.1-0.5cm residual disease, R2-0.5-1cm residual disease), was more in Type II compared to Type I showing borderline statistical significance (p value.0.566). According to the pattern of distribution, PDS and IDS was assessed in all the 3 Groups in Type I & II EOC. Type I had 94.4% PDS compared with 66.2% Type II in Group A (pelvis, nodes) showing clinically and statistical significance (p value 0.001.). In group B (omentum, peritoneum, hemidiphram, liver) Type I had 88.2% PDS vs 60% in type II showing clinically and statistical significance (p value 0.038). In group C (Porta, mesentry, lesser sac) Type I had 75% PDS vs 63.2% in type II showing clinically and statistical significance(p value 0.0676). According to the pattern of distribution, cytoreductability (R0/R1,2) was assessed in all the 3 Groups in type I & II EOC. Type I had 8.8% R1/2 compared with 32.6% Type II in Group A (pelvis, nodes) showing clinically and statistical significance (p value 0.016). In group B (omentum, peritoneum, hemidiphram, liver) Type I had 13.3% R1/2 vs 51.9% in type II showing clinically and statistical significance(p value 0.044). In group C (Porta, mesentry, lesser sac) Type I had 33.3%R1/2 vs 58.3% in type II, not showing statistical significance (p value 0.429). Conclusion: Type I EOC patients appear to present at earlier stages with younger age of presentation, their distribution in group B (Omentum, Peritoneum, Surface Liver, Hemidiaphragm) has a significant p value in relation to their cytoreductability (R0,R1/2). However, Progression free survival analysis an overall survival was not significant due to the short follow up interval.
Introduction
Ovarian cancer (OC) is the eighth most common cancer among women worldwide, and the leading cause of death from gynaecologic malignancies with an estimated 295,414 incident cases and 184799 deaths annually.
Previously EOC was believed to originate primarily from the surface epithelial cells covering the ovaries and lining subserosal cysts [1, 2, 3]. However, recent morphologic, immunohistochemical and molecular studies have led to a new paradigm for the pathogenesis and origin of EOC, dividing EOC into two groups designated as type I and type II [4, 5].
A number of studies have investigated the prognostic value of dividing serous ovarian cancer in high- and low- grade serous carcinomas from pathological characteristics [6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20]. However, only few studies have included the full spectrum of histological subtypes of EOC and a comprehensive number of other prognostic values, when evaluating the FIGO stage, cytoreductability, Progression free survival and overall survival of the two groups [21, 22].
Methods
The primary objective was to study the association of types of epithelial ovarian cancer with stage. Secondary objectives was to study the association of types of epithelial ovarian cancer with cytoreduction, and to determine the progression free survival rate of type I and II epithelial ovarian cancer.
Selection and Description of Participants
Our study design was a Prospective comparative study. We included all patients with epithelial ovarian carcinoma and patients who underwent primary cytoreductive surgery or Interval Debulking surgery here at our institute for a period of 2 years (09/2016–012/2018) .We excluded Non epithelial ovarian carcinomas, Boderline ovarian tumours, Endometrial cancer and Benign pathology. Institutional ethical committee clearance was obtained and patients who provided the written informed consent were included. Baseline patient information was obtained, including date of birth, age, sex, height, weight, relevant medical history, histology, grade, BMI, Oncology treatment, FIGO stage, CA125.
Surgical Staging Procedure
All patients who underwent both primary and interval debulking surgery for epithelial ovarian cancer had a Mid- line incision, followed by complete analysis of the pattern of distribution of the disease and Grouped into 3 categories-Group A (Pelvis, nodes), Group B (omentum, peritoneum, hemidiaphragm, surface liver), Group C (Mesentry, Porta hepatic, Lesser sac). In case of advanced disease patients underwent diagnostic laparoscopy followed by assessment for resectability using Fagotti score/sugar bakers peritoneal carnicomatosis index. If disease was found to be extensive (Fagotti>8/PCI>17) these patients underwent Neoadjuvant cheomotherapy with Paclitaxil and Carboplatin and then assessed for interval surgery.
Residual disease was defined as R0-no residual macroscopic disease after surgery, R1-0.1-0.5cm residual disease, R2-0.5-1cm, R3>1cm. Stages are defined according to the FIGO classification WHO 2014 criteria (I– IV), stage I/II is considered early FIGO stage, and stage III/IV, where the tumor has spread beyond the pelvic region, as late FIGO stage. The categories of grade are well-differentiated (Grade 1), moderately differentiated (Grade 2), and poorly differentiated (Grade 3). Grade 1 is considered as low-grade tumors and Grades 2–3 as high- grade tumors.
Histologic types were defined as serous adenocarcinoma, mucinous adenocarcinoma, endometrioid adenocarcinoma, clear cell neoplasms, carcinosarcoma, transitional/Brenner tumors, mixed tumors, or undifferentiated carcinomas along with their IHC markers (p53, WT 1, ER, Napsin)were obtained from their histopathology reports. All pathologic diagnoses were given by our dedicated Onco-pathologists.
No new intervention is required in this study. Progression free survival rate was defined as the time interval from the date of primary surgery to the date of disease progression or recurrence
Statistical Analysis
Statistical analysis was performed using IBM SPSS version 20.0 software. Categorical variables are expressed using frequency and percentage. Continuous variables are presented using mean and standard deviation. To test the statistical significance of the association between categorical variables Chi square test was used. To determine the Progression free survival rate of dividing epithelial ovarian cancer into Type I and Type II Kaplain Meir curve will be applied and compared with Log rank test.
Results
A total of 145 patients diagnosed with EOC during this period were included in the study, out of this, 44 patients were excluded as IHC was not done or they had undergone NACT followed by Interval surgery without IHC. Among 101 patients 36 were categorized as type I tumors, and 65 as type II tumors.
Among 101 patients 36 were categorized as type I tumors, and 65 as type II tumors, the overall distribution was serous type 2 -59.4%, clear cell carcinoma-14.9%, serous type 1-13.9, mucinous carcinoma-5.9% endometrioid carcinoma type 1-5.9%. (Table 1). In general younger age predisposition was found in Type I, than Type II. The Mean age was 55yr (±12.9), which was used as the cut off age to compare the two types. This has a statistically significant p value (<0.001). Patients with type I EOC 91.7% had a good performance status and were in ECOG 0,1 category, compared to type II, the p value (0.412) was not statistically significant .
| Histopathology subtype | Frequency | Percent |
|---|---|---|
| Serous type 1 | 14 | 13.9 |
| Serous type 2 | 60 | 59.4 |
| Clear cell carcinoma | 15 | 14.9 |
| Mucinous carcinoma | 6 | 5.9 |
| Endometrioid type 1 | 5 | 5 |
| Endometrioid type 2 | 1 | 1 |
| Total | 101 | 100.0 |
Table 1: Distribution of EOC Subtypes.
Patients with type II EOC had elevated CA 125 more than 500, compared to type I, showing a statistical significance (p value.0.001) Ascitis at the time of presentation was observed more in Type I 67.7%,compared to 33.3% in type II showing clinically and statistically significant p value (0.002).
| FIGO | Type 1n=36(%) | Type 2n=65(%) | p value |
| 1&2 | 63.9 | 30.8 | 0.001 |
| 3&4 | 36 | 69.2 | 0.001 |
Table 2: Comparison of surgery type.
At the time of diagnosis patients presented with early FIGO stage (1&2) in Type I in 63.9% and Late FIGO stage (3&4) 69.2%, showing a statistical significance (p value.0.001) (Table 2).
majority of type I patients presented at an early FIGO stage (1&2) favoring more number of PDS in this group (Table 3).
| Debulking surgery type | Type 1 n=36(%) | Type 2 n=65(%) | p value |
|---|---|---|---|
| PDS(77) | 34(94.4) | 43(66.2) | 0.001 |
| IDS(24) | 2(5.6) | 22(33.8) | 0.001 |
Table 3: FIGO stage.
Primary debulking surgery rate (PDS) with complete cytoreduction (R0) was more in Type I EOC, with almost 91.2% showing clinically and statistical significance (p value.0.016), whereas R0(no residual macroscopic disease after surgery) was achieved only in 67.4% of Type II EOC.R1/R2 (R1-0.1-0.5cm residual disease, R2-0.5-1cm residual disease),was more seen in Type II showing borderline statistical significance(p value.0.566) (Table 4).
| Type | Debulking surgery type | Surgery Type | P value | |
| Type | Debulking surgery type | R0 | P value | R1/R2 |
| 1 | PDS | 31(91.2) | 3(8.8) | 0.016 |
| 1 | IDS | 0(0) | 2(100) | 0.016 |
| 2 | PDS | 29(67.4) | 14(32.6) | 0.566 |
| 2 | IDS | 17(77.3) | 5(22.7) | 0.566 |
Table 4: Distribution of cytoreductability in type 1 & 2 EOC.
Among 101 patients, 36 patients in Type I and 65 patients in Type II had Group A pattern of distribution(pelvis and nodes) (Figures 1 & 2), Intraoperative pattern of spread was categorized into 3 groups, Group A-Pelvis, Nodes; Group B-Omentum, Peritoneum, hemidiaphragm, Liver surface; Group C-
Portaheptais, Mesentry, Lesser sac ;and their distribution was plotted in type I and II.
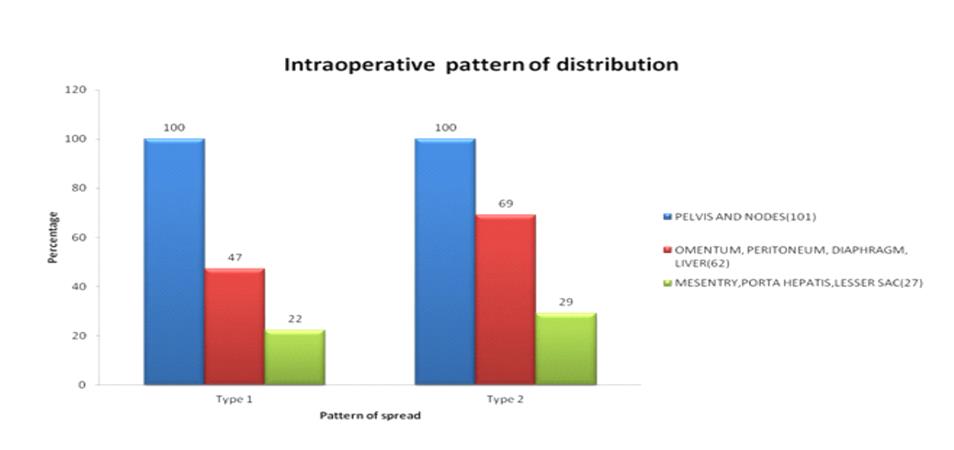
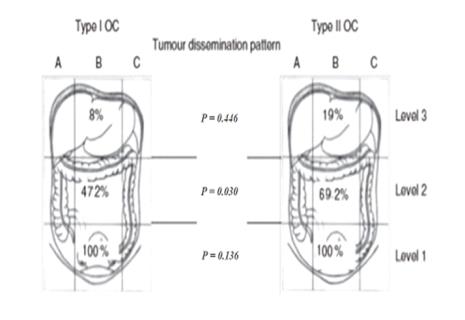
As observed in our study the Intraoperative pattern of spread between Type I & II EOC, Both had 100% distribution in Pelvis and nodes, Type II had an increased pattern of distribution in the omentum, peritoneum, hemidiaphragm, liver about 69.2% compared to 47.2% in type and was showing clinically and statistical significance (p value 0.030). Distribution in portaheptais, mesentry, lessersac, not showing statistical significance (p value.0.446) in type II about 19%, compared to 8% in type I EOC (Figure 3).
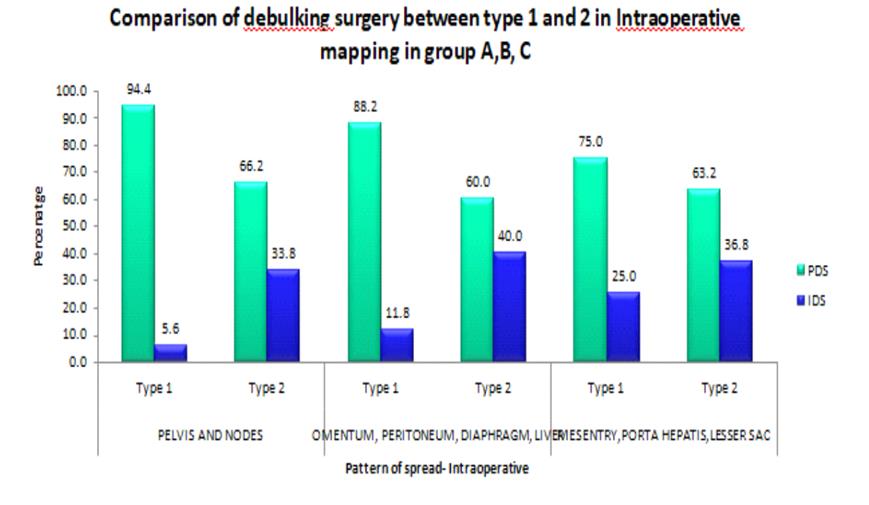
According to the pattern of distribution, PDS and IDS were assessed in all the 3 Groups in type I & II EOC. Type I had 94.4% PDs compared with 66.2% Type II in Group A (pelvis, nodes) showing clinically and statistical significance (p value 0.001.). In group B (omentum, peritoneum, hemidiphram, liver) Type I had 88.2% PDS vs 60% in type II showing clinically and statistical significance (p value 0.038). In group C (Porta, mesentry, lesser sac) Type I had 75% PDS vs 63.2% in type II showing clinically and statistical significance(p value 0.0676) (Figure 4) .
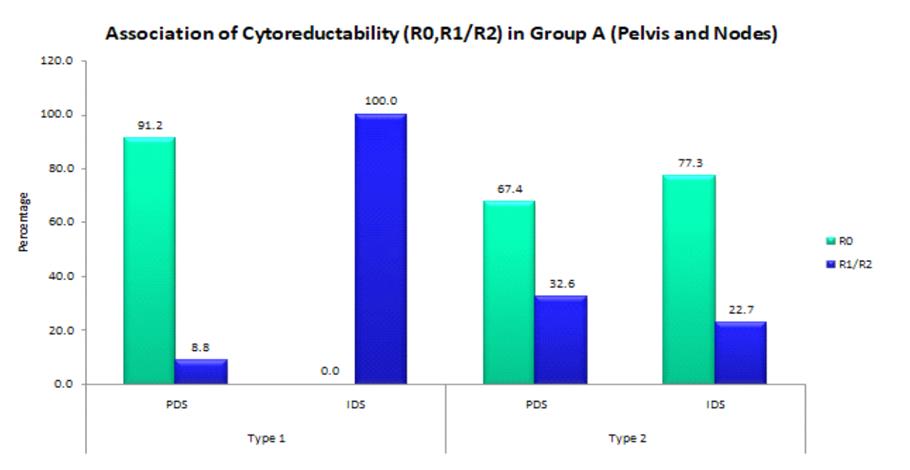
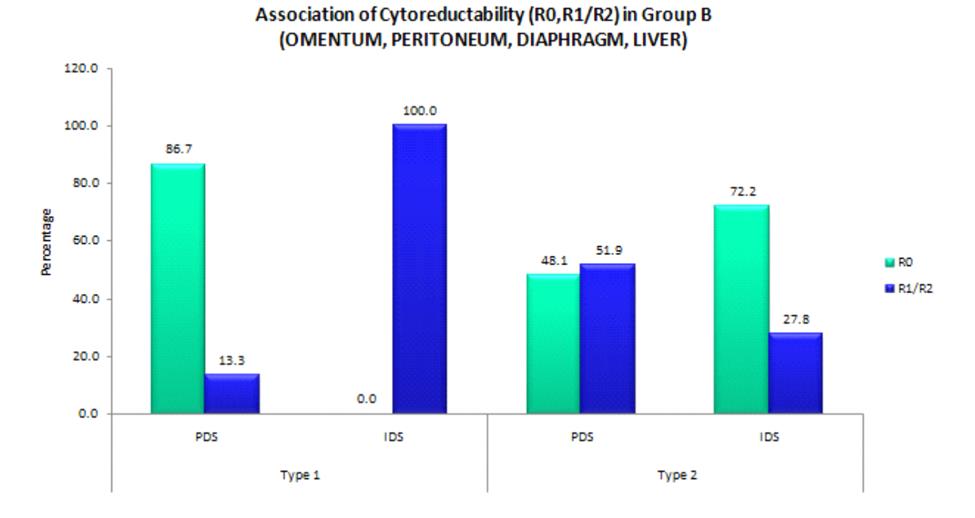
According to the pattern of distribution, cytoreductability (R0/R1,2) was assessed in all the 3 Groups in type I & II EOC. Type I had 8.8% R1/2 compared with 32.6% Type II in Group A (pelvis, nodes) showing clinically and statistical significance (p value 0.016). In group B (omentum, peritoneum, hemidiphram, liver) Type I had 13.3% R1/2 vs 51.9% in type II showing clinically and statistical significance(p value 0.044). In group C (Porta, mesentry, lesser sac) Type I had 33.3%R1/2 vs 58.3% in type II, not showing statistical significance (p value 0.429) (Figure 5).
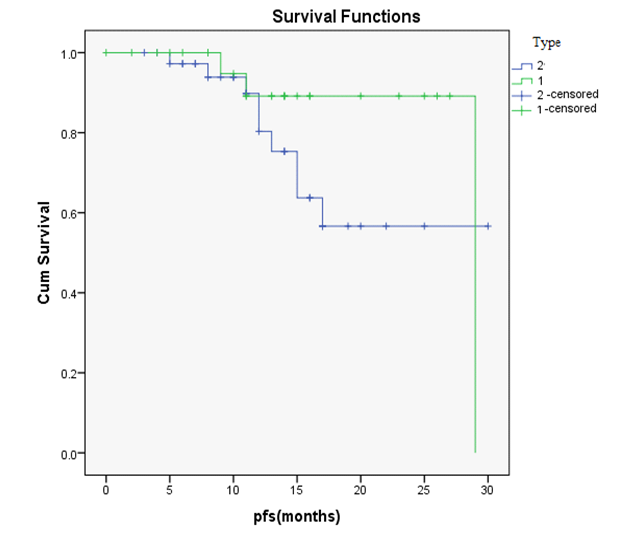
Recurrence median survival time: 24.25 months [95% CI:21.54-26.96]. Follow up mean period: 26.3 months [95% CI:23.99-28.62] 2 year PFS time:35%The difference in the Progression free survival for Type I is 26.944 and Type II is 22.579, is found to be statistically not significant (p value 0.21). The estimation is not significant as the analysis of PFS will require a longer follow up duration. The mean Follow up period was 26.3 months (Figure 6).
Discussion
In our study we classified epithelial ovarian carcinomas based on histopathology and immunohistochemistry into Type I & II.
Several studies have investigated the eligibility of a dualistic model for ovarian serous carcinoma [5, 15, 16, 17, 18, 19, 20, 21]. All studies show that a dualistic model for ovarian serous cancer is a significant predictor of survival. Most of these studies, however, have only focused on ovarian serous carcinomas and have not included all histological subtypes of OC, and thereby the specified divisions into type I and type II tumors proposed by Kurman and Shih [5, 6, 7, 11]. We have extensively looked into parameters like age at the time of diagnosis, ascitis, Ca 125 levels, Pattern of spread, Primary /Interval debulking surgery, cytoreductability. Progression free survival and overall survival analysis which defines and types the EOC into category Type I and II. A Danish population-based study by Hannibal, et al. [17] evaluated the prognostic significance of histologic grade of tumor in serous EOC dividing serous ovarian cancer into LGSC and HGSC. They found LGSC to have a significant better prognosis than HGSC. Although, including a large cohort (n= 4317) combined with a long observation time (28 years), they only included ovarian serous carcinoma and did not investigate the specific distribution into type I and type II EOC. Furthermore this study was carried out before the introduction of centralized national treatment guidelines for OC, and did not have the advantages of comparing several prognostic variables from a clinical database, such as treatment.
To our best knowledge, only one other study by Braicu, et al. [22] has analyzed the prognostic impact of dividing EOC into type I and type II tumors based exclusively on pathological features, where no significant difference in overall survival for the advanced FIGO stages (III–IV) was found. Nevertheless this study did not investigate survival for type I tumors vs. type II tumors in a multivariate analysis, adjusted for other likely prognostic variables, had a relative short follow-up time (median = 23 months) and included a notable smaller number of patients (n = 632) with an uneven distribution in type I (n = 100) and type II (n= 532).
In our study we subcategorised Type I LGSC, low- grade endometrioid adenocarcinomas, clear cell neoplasms, mucinous adenocarcinomas and Brenner tumors. Type II tumors comprised HGSC, high-grade endometrioid adenocarcinomas, carcinosarcomas and undifferentiated carcinomas with a sample size of n=101 (Type I=36, type II-65). The overall survival and Progression free survival were not found to be statistically significant as the follow up duration was only for 2 years.
We demonstrated that type I patients were significantly younger at initial presentation of disease compared with patients with type II tumours. To our knowledge, very few studies have assessed the impact and significance of tumour histology using a validated and systematic documentation tool such as Intraoperative mapping pattern of distribution, where intraoperative tumour dissemination, tumour residuals are described and recorded in a prospective and systematic manner using specifically designed schemes and figures (Figure 3), avoiding potential bias and errors in the assessment of tumour dissemination and site of tumour residuals as described in our study.
Even though the existing guidelines regarding EOC do not officially include the histological subtype in the decision-making process, there is increasing evidence that indicates histology has a significant role in the overall patients’ outcome and prognosis [23, 24, 25].
In a further study by the GOG, advanced stage mucinous adenocarcinoma of the ovary is being characterised as highly lethal with highly significantly lower OS rates compared with women with serous carcinoma (14 vs 42 months; P<0.001).
We performed a subanalysis of the prognostically more favourable cohort of the tumour free operated patients and showed that type II histology had higher residual disease in terms of cytoreducatbility. This might be hence a sign of a potential ‘higher aggressiveness’ of type II cancers after all, whereas the exact underlying mechanisms have to be investigated in future trials.
It is known that underlying the general high mortality of EOC is the molecular behaviour of the disease, with 75% of patients presenting at an advanced clinical stage, in terms of a high-volume disease with dissemination in the entire abdominal cavity [7]. Type I tumours have been described as slow growing, as evidenced by the observation that they are large and often confined to the ovary at diagnosis [5]. This observation was corroborated in this study, where type I tumours initially presented in at an early stage restricted to the pelvis, and only 47% in type I with spread to the (Introperative pattern of distribution Group B-Omentum, peritoneum, hemidiaphragm, surface of liver) as opposed to 69% in type II patients. This may imply that despite the fact that rare entities such as mucinous and clear cell carcinomas show a poorer response to conventional chemotherapeutic regimes, their tendency to be diagnosed at earlier stages, confined to the pelvis, may actually result in a more favorable prognosis and more beneficial profile of the type I tumours.
Conclusion
It is now known that underlying the general high mortality of EOC is the molecular behaviour of the disease, with 75% of patients presenting at an advanced clinical stage, in terms of a high-volume disease with dissemination in the entire abdominal cavity [7]. Type I tumours have been described as slow growing, as evidenced by the observation that they are large and often confined to the ovary at diagnosis [5]. This observation was corroborated in this study, where type I tumours initially presented at an early stage restricted to the pelvis, nodes (Group A), as opposed to type II patients who had a increased predominance pattern in peritoneum, omentyum, hemidiaphragm, Liver (Group B) with a significant p value and with clinically significant pattern of spread in Portahepatis, lesser sac, mesentry (Group C). This was reflected proportionally in cytoreductability with more patients in R1/2 (suboptimal cytoreduction) in type II compared to Type I who has R0 (optimal cytoreduction).
Our strength of our study is that it was conducted as a Prospective study, In a well-established Department of Gynaecological oncology with complete documentation of our entire intraoperative disease pattern, combined with our specialized Gynaec-Oncopathologist, limiting the potential of misclassification, and all our patients had a 100% follow up during the period of study.
Our study analysed that prognostically more favourable cohort of the tumour free operated patients and showed that type II histology was a negative prognosticator of survival (Progression free survival and overall survival). This might be hence a sign of a potential ‘higher aggressiveness’ of type II cancers after all, whereas the exact underlying mechanisms have to be investigated in future trials.
Rare entities such as mucinous and clear cell carcinomas show a poorer response to conventional chemotherapeutic regimes, their behavioural pattern and classification into Type I or II is still a Grey zone, because of their significant low numbers and their tendency to be diagnosed at earlier stages, confined to the pelvis, may actually result in a more favourable prognosis and more beneficial profile of the type I tumours from our study.
However, these hypotheses have to be verified in prospective morphological and molecular genetic studies, where a molecular biological profiling of the tumour will be conducted at inception of the disease and, subsequently, correlated with surgical outcome and survival. In this way a new rationale in the approach to detection, therapeutic management and follow-up may be developed, which would be closer to the actual tumour biology profiling and large scale heterogeneity of the disease and may allow a more individualized and potentially more effective management.
Limitations
Follow up period was short, and hence Overall survival could not be analyzed. In our analysis we did not perform an assessment of the Ras/Raf wild type, which may be noted as shortcoming of this study which would have further helped us in typing ovarian cancer into I and II. Multicentric analysis with a larger sample size and longer follow up would have further increased the strength of this study.
References
-
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, et al. (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer (Journal international du cancer) 127(12): 2893-2917.
-
Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013. CA Cancer J Clin 63(1): 11-30.
-
Auersperg N, Ota T, Mitchell GW (2002) Early events in ovarian epithelial carcinogenesis: progress and problems in experimental approaches. Int J Gynecol Cancer 12(6): 691-703.
-
Singer G, Kurman RJ, Chang HW, Cho SK, Shih IeM (2002) Diverse tumorigenic pathways in ovarian serous carcinoma. Am J Pathol 160(4): 1223-1228.
-
Shih Ie M, Kurman RJ (2004) Ovarian tumorigenesis: a proposed model based on morphological and molecular genetic analysis. Am J Pathol 164(5): 1511- 1518.
-
Kurman RJ, Shih Ie M (2010) The origin and pathogenesis of epithelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol 34(3): 433-443.
-
Kurman RJ, Shih IeM (2008) Pathogenesis of ovarian cancer: lessons from morphology and molecular biology and their clinical implications. Int J Gynecol Pathol 27(2): 151-160.
-
Kindelberger DW, Lee Y, Miron A, Hirsch MS, Feltmate C, et al. (2007) Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: evidence for a causal relationship. Am J SurgPathol 31(2): 161-169.
-
Crum CP, Drapkin R, Miron A, Ince TA, Muto M, et al. (2007) The distal fallopian tube: a new model for pelvic serous carcinogenesis. Curr Opin Obstet Gynecol 19(1): 3-9.
-
Ahmed AA, Etemadmoghadam D, Temple J, Lynch AG, Riad M, et al. (2010) Driver mutations in TP53 are ubiquitous in high grade serous carcinoma of the ovary. J Pathol 221(1): 49-56.
-
Kurman RJ, Shih Ie M (2011) Molecular pathogenesis and extraovarian origin of epithelial ovarian cancer- shifting the paradigm. Hum Pathol 42(7): 918-931.
-
WHO (2014) WHO Classification of Tumors of Female Reproductive Organs. International Agency for Research on Cancer, World Health Organization, Lyon, pp: 1511- 1518.
-
Ayhan A, Kurman RJ, Yemelyanova A, Vang R, Logani S, et al. (2009) Defining the cut-point between low- and high-gradeovarian serous carcinomas: A clinicopathologic and molecular geneticanalysis. Am J Surg Pathol 33(8): 1220-1224.
-
Bowtell DD (2010) The genesis and evolution of high- grade serous ovarian cancer. Nat Rev Cancer 10(11): 803-808.
-
Kobel M, Kalloger SE, Santos JL, Huntsman DG, Gilks CB, et al. (2010) Tumor type and substage predict survival in stage I and II ovarian carcinoma: insights and implications. Gynecol Oncol 116(1):50-56.
-
Bodurka DC, Deavers MT, Tian C, Sun CC, Malpica A, et al. (2012) Reclassification of serous ovarian carcinoma by a 2-tier system: a Gynecologic Oncology Group study. Cancer 118(12): 3087-3094.
-
Hannibal CG, Vang R, Junge J, Kjaerbye-Thygesen A, Kurman RJ, et al. (2012) A binary histologic grading system for ovarian serous carcinoma is an independent prognostic factor: a population-based study of 4317 women diagnosed in Denmark 1978– 2006. Gynecol Oncol 125(3): 655-660.
-
Motohara T, Tashiro H, Miyahara Y, Sakaguchi I, Ohtake H, et al. (2010) Long-term oncological outcomes of ovarian serous carcinomas with psammoma bodies: a novel insight into the molecular pathogenesis of ovarian epithelial carcinoma. Cancer Sci 101(6): 1550-1556.
-
Seidman JD, Horkayne-Szakaly I, Cosin JA, Ryu HS, Haiba M, et al. (2006) Testing of two binary grading systems for FIGO stage III serous carcinoma of the ovary and peritoneum. Gynecol Oncol 103(2): 703- 708.
-
Malpica A, Deavers MT, Lu K, Bodurka DC, Atkinson EN, et al. (2004) Grading ovarian serous carcinoma using a two-tier system. Am J Surg Pathol 28(4): 496- 504.
-
Steffensen KD, Waldstrom M, Grove A, Lund B, Pallisgard N, et al. (2011) Improved classification of epithelial ovarian cancer: results of 3 Danish cohorts. Int J Gynecol Cancer 21(9): 1592-1600.
-
Braicu EI, Sehouli J, Richter R, Pietzner K, Denkert C, et al. (2011) Role of histological type on surgical outcome and survival following radical primary tumour debulking of epithelial ovarian, fallopian tube and peritoneal cancers. Br J Cancer 105(12): 1818- 1824.
-
Høgdall LT, Nielsen MLS (2011) Danish Gynecologic Cancer Database. A nationwide clinical database for cancer in ovaries, uterus and cervix, pp: 1-97.
-
Alexander J Cole, Trisha Dwight, Anthony J Gill, Kristie-Ann Dickson, Ying Zhu, et al. (2016) Assessing mutant p53 in primaryhigh-grade serous ovarian cancer using immunohistochemistry and massively parallel sequencing. Scientific reports, Nature.
-
Piek JM, Verheijen RH, Kenemans P, Massuger LF, Bulten H, et al. (2003) BRCA1/2-related ovarian cancers are of tubal origin: a hypothesis. Gynecol Oncol 90(2): 491.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’