Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome
Introduction: Polycystic ovarian syndrome (PCOS) is a common endocrine disorder in reproductive women and leading causes of female sub fertility. Symptoms include amenorrhea, infertility, anovulation with irregular menstruation, and excessive release of androgenic hormones. When compared to normal women, PCOS patients have higher serum AntiMullerian hormone (AMH) levels, along with increased serum androgens and higher number of small-antral follicles. Objective: This study seeks to explore the effectiveness of previous literature on usefulness of testing serum levels of, LH, FSH in comparison with AMH for a period of 3 months of treatment. Methods: Prospective and cross sectional study, conducted from march 2017 to Oct 2018. 100 women reporting to OBG clinic with inclusion criteria were , Age group: ≥ 18 to ≤ 40 years, Patients complaining of irregular menstruation, amenorrhea and infertility, while exclusion criteria were women with any other co morbid conditions, receiving any medications, Pregnant, lactating and post-menopausal women. We divided them into two groups of 50 each. Group 1 was analyzed for LH, FSH, and scanning (as routine) and group 2 were analyzed for LH, FSH, AMH and scanning (as routine). The blood was centrifuged, separated and analyzed at Central laboratory. To compare between LH, FSH with AMH, we use USG scan as standard diagnostic tool to prove the efficacy of AMH. Conclusion: Our results showed that serum AMH has significant increase in PCOS compared to serum LH and FSH levels. Our findings conclude that AMH is good clinical parameters that can be used for diagnostic testing of PCOS.
Introduction
Polycystic ovarian syndrome (PCOS), a common endocrine disorder in women with leading cause of female fertility. The symptoms of polycystic ovaries include amenorrhea, infertility, anovulation with irregular menstruation and excessive release of androgenic hormones [1, 2, 3, 4, 5, 6, 7]. This syndrome of ovarian dysfunction has shown to affect 4-18% of reproductive women worldwide [8]. Women diagnosed with PCOS have additionally revealed to exhibit a pattern for pre-obesity with links indicating a high progression of 30-40% of them progressing towards having type 2diabetes (T2D). Some may also present with abnormalities in insulin resistance (IR), inflammation, adipose tissue dysfunction, impaired fasting glucose (IGF) and impaired glucose tolerance (IGT) [9, 10].
In 1990, at consensus workshop which was sponsored by NIH/NICHD the diagnostic criterion for PCOS was defined. It was said that PCOS patient has androgen excess, oligo ovulation, and other entities [11, 12]. In 2003, workshop sponsored by ESHRE/ASRM in Rotterdam, said that PCOS patient suffering from with any two from three criteria like anovulation or oligo, polycystic ovaries detected by gynecologic ultrasound, excess androgenic activity and, other entities are to be excluded that would cause the same [13], while the definition by Rotterdam includes more patients with or without excess of androgen. The study results of patients with androgen excess and without androgen excess cannot be extrapolated [14, 15, 16].
Studies have suggested that during PCOS imbalance of other hormones also can occur, along with androgenic excess while when compared to normal subjects, in PCOS patients the levels of serum Anti-Mullerian hormone (AMH) will be increased [16, 17, 18]. In female, from pre- antral and small-antral follicles it produces post-natally by granulosa cells and in male, sertoli cells produce during fetal sex differentiation and induces Mullerian duct inhibition [19, 20, 21]. Women with PCOS have increase number of small-antral follicles with high serum androgens. Controversies still exist with its correlation to serum androgens even though, serum AMH levels have been correlated positively with numbers of small-antral follicles [21, 22].
We consider that, there are very few explorative study among women with PCOS for detecting serum levels of luteinizing hormone (LH), follicle stimulating hormone (FSH) and AMH. Therefore this study seeks to explore the Dwajani S and Rupakala BM. Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome. J Gynecol 2019, 4(2): 000179.
effectiveness of previous literature on usefulness of testing serum levels for a period of 3 months of treatment of AMH in comparison with LH, FSH. Hence our objective was to explore the effect of testing serum levels of AMH with LH, FSH women with PCOS.
Methods
Institutional Ethical Review Board approval was obtained prior to initiation of the study and ICH-GCP guidelines will be followed until completion. Study was conducted by department of pharmacology/central research lab along with department of obstetrics and gynaecology, at rajarajeswari medical college, Bangalore.
This is a prospective, cross sectional study, conducted from March 2017 to oct 2018. We enrolled 100 women reporting to OBG clinic with complaints/ symptoms of PCOS. Inclusion criteria were –
- Age group: ≥ 18 to ≤ 40 years
- Patients complaining of irregular menstruation, amenorrhea and infertility.
- Patients who consented to participate, while exclusion criteria were
To compare between LH, FSH with AMH, we use USG scan as standard diagnostic tool to prove the efficacy of AMH. We also tried to prove the efficacy of LH FSH by combining two groups and as separate entity. In order to estimate the efficacy of LH and AMH measurements into “normal” and “high”, their Receiver operating characteristics [ROC] curve were plotted. The ROC curve plots specificity v/s sensitivity. Area under curve [AUC] is expressed in percentage which represents the ability to classify normal and high values.
All the data were entered into Microsoft excel sheet before analysis. The data was analyzed using descriptive Copyright© Dwajani S and Rupakala BM.
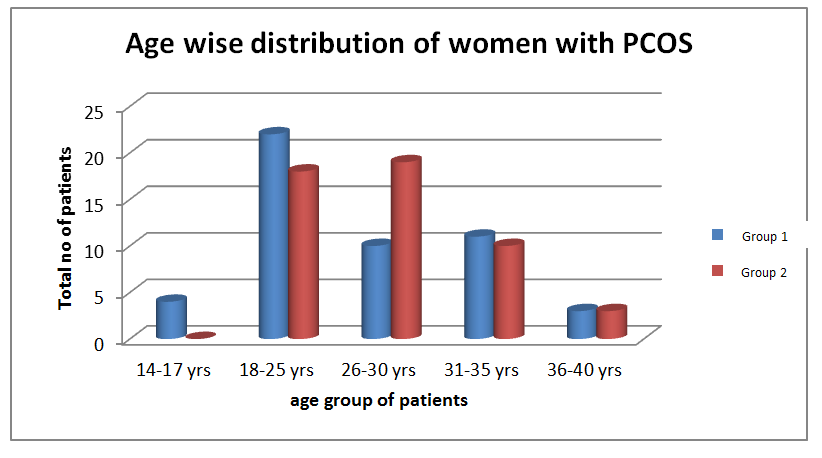
statistics. Quantitative data was expressed as mean, standard deviation, qualitative data as percentage and frequency distribution. Statistical package “R” version 4.2 was used for analysis. For comparing the efficacy of LH, FSH and AMH bar graphs were used which represents the fraction. The standard errors on mean fraction were computed using SE = √ p(1-p) / n, where p is the fraction of patients in group-2 showing “high” for the test. ROC curve for LH and AMH classification were plotted using pROC library. All the computations including estimation Total 100 women with PCOS were recruited in the study. Among two groups majority of women were in age range between 18-25 years and represented in Figure 1. 70% of women with PCOS were married. 70% in group 1 and 58% in group 2 were from rural background.
of statistical parameters, detection effectiveness, ROC curve and welsch independent ‘t’ test were performed.
Results
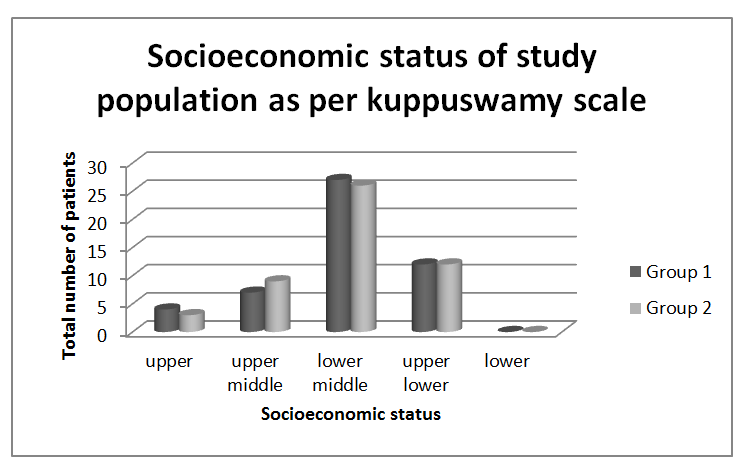
To calculate the socioeconomic status we used revised kuppuswamy scale we had 54% in group 1 and 52% of women with PCOS in group 2 who were in the lower middle class (Figure 2) [23].
Dwajani S and Rupakala BM. Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome. J Gynecol 2019, 4(2): 000179.
Copyright© Dwajani S and Rupakala BM.
Among 100 women with PCOS, only 5% of patients had family history. Majority of the women had irregular cycles between 60 days to 90 days and had a menstrual flow for 10 to 15 days. All patients were newly diagnosed patients who were not on any treatment for PCOS. Majority of them complained of dysmennorhea and heavy flow.
Comparison of Detection Efficiency of PCOS for AMH and LH, FSH
The bar chart below shows the fraction of patients in Group 2 for whom the LH, FSH and AMH were performed and the results showed “high”. For all the 50 patients, scan report showed confirmation for PCOS. Hence these ratios represent efficiency for detecting PCOS. The error bars represent standard error on observed mean fractions
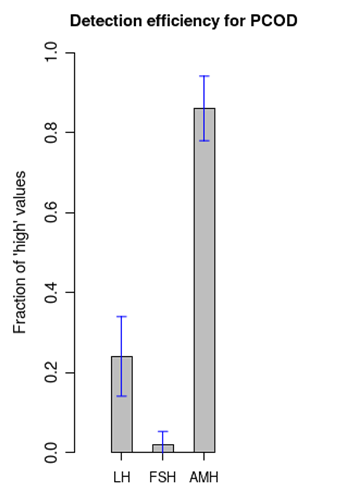
- From this plot, we notice that within standard errors, the AMH has considerable higher efficacy of detection
- [>82%] when compared to LH and FSH [< 30%]. The values of the above plot are summarized in the table below
- High Normal
- No of patients
- Fraction
- SE (Standard of high
- Error)
- LH
- 12
- 38
- 50
- 0.24
- 0.01
- FSH
- 1
- 49
- 50
- 0.02
- 0.032
- AMH
- 43
- 7
- 50
- 0.86
- 0.081
Table 1: Values of LH,FSH, AMH.
Comparison between Group-1 and Group-2
In order to compare the values of LH, FSH and AMH across Group-1 and Group-2, two sample independent t test with unequal variances (Welsch test) was performed. The results are summarized here in the table. The p values between Group 1 and Group 2 indicate that the values of LH and FSH are not significantly different, with a significance level of 0.05 assumed for the test.
| Mean and SD in Group-1 | Men and SD in Group-2 | P-value of t-test | |
|---|---|---|---|
| LH | 9.09 ± 5.72 | 8.35 ± 3.39 | 0.434 |
| FSH | 7.15 ± 4.22 | 6.85 ± 2.70 | 0.68 |
Table 2: Values of LH and FSH across two groups.
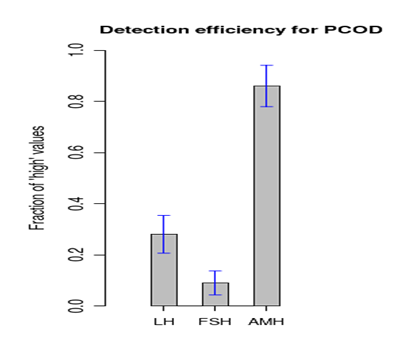
Detection Efficiencies by Combining Data Sets of Group 1 and Group 2
The two data sets of Group-1 and Group-2 were combined to get the detection efficiencies for LH and FSH. The efficiency of AMH was available only for Group-2 as computed before. This combined data is shown in the table below and plotted in the following graph.
| High | Normal | No. of patients | Fraction of high | Standard error SE | |
| LH | 28 | 72 | 100 | 0.28 | 0.074 |
| FSH | 9 | 91 | 100 | 0.09 | 0.047 |
| AMH | 43 | 7 | 50 | 0.86 | 0.081 |
Table 3: Values of LH, FSH and AMHb.
Dwajani S and Rupakala BM. Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome. J Gynecol 2019, 4(2): 000179.
Copyright© Dwajani S and Rupakala BM.
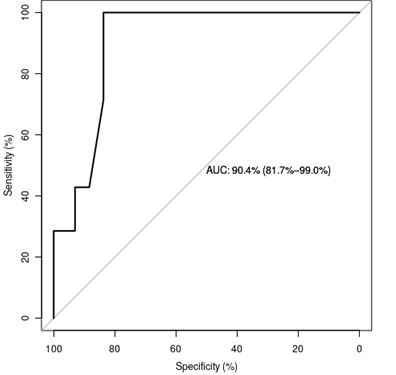
ROC curve for the LH and AMH
In order to estimate the efficiency of the classification of LH and AMH measurements into “normal” and “high” categories, their ROC curves were plotted using “pROC” library of R statistical package. The two figures corresponding to LH and AMH are given below:
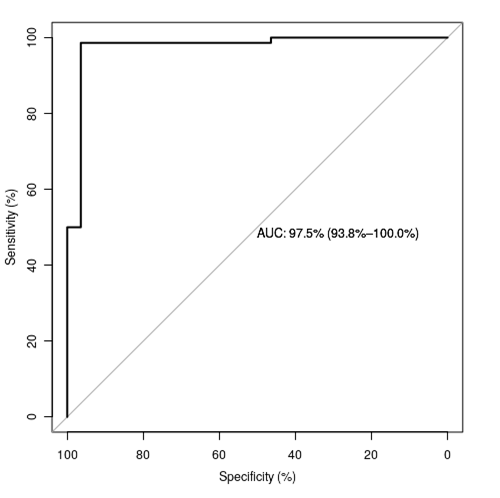
The ROC curve for LH has a very good AUC of 97.5% indicating that the LH classification of high and low classification is efficient. Similarly, the Roc curve for AMH classification into high and low has a good AUC value of 90.4%.
Dwajani S and Rupakala BM. Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome. J Gynecol 2019, 4(2): 000179.
Discussion
In our study we observed to have higher levels of AMH in women with PCOS. Studies have shown that women with PCOS differed in their LH concentrations and it can also peak to three times the levels of their FSH values [24, 25]. We also observed that LH/FSH levels were significantly different on comparing with other groups. In contrast, according to 2003 Rotterdam ESHRE/ASRM criteria, it was stated clearly that LH/FSH should not be recommended as an identifier for women having PCOS where a study later proved them correct by concluding that LH/FSH ratio had little effect in diagnosing PCOS [26].
PCOS has a broad spectrum of biochemical and clinical characteristics while its distinctive feature of follicular maturation is a failure. FSH sensitivity is inhibited by AMH synthesized in small antral follicles and an important parameter which plays a pivotal role in diagnosis of PCOS. Our study results show that women with PCOS have significantly higher serum AMH levels while correlations with androgens in PCOS have been reported [27]. On contrary, no correlations has been found either in normal women or in PCOS [28, 29, 30, 31].
A positive relationship had been revealed by our study, between levels of FSH and AMH. Hence, lower levels of FSH are associated with higher levels of AMH. This is in support of the speculation that excess of AMH is involved in decreasing FSH induced aromatase activity Copyright© Dwajani S and Rupakala BM.
which is a characteristic feature for follicular arrest in PCOS [32]. Since PCOS is leading cause of female infertility, it is therefore recommended that women who experience these symptoms seek their gynecologist for advice. Physicians must continue to highlight the importance dietary changes to include grains, vegetables and fruits as prevention of PCOS. Dietary and lifestyle modifications of women must be looked at from all angles and their development to PCOS. As research calls it, “this thief of womanhood” is been affecting women daily while more importance should be given on women living with PCOS [33]. Even though we live in a “gender-polarized” and advanced technological world, a young woman without a menstrual cycle, psychological discomfort and infertility problems can soon be sadly outnumbered with our future children being computers, machines and robots [34].
Limitations of Study
More detailed information on quality of life, life style modifications and dietary changes would have added more impact on this manuscript.
Conclusion
From our results of present study, we conclude that serum AMH levels are significantly increased in PCOS when compared to serum LH and FSH levels. Our findings conclude that AMH can be considered as good clinical parameters which can be used for diagnostic testing of PCOS.
Acknowledgment
Authors wish to sincerely thank our statistician Dr. R. Srivatsan and all the patients who gave their invaluable contributions to this research
References
-
Legro RS, Strauss JF (2002) Molecular progress in infertility: polycystic ovary syndrome. Fertil Steril 78(3): 569-576.
-
Kandarkis ED, Kandarakis H, Legro RS (2006) The role of genes and environment in the etiology of PCOS. Endocrine 30(1): 19-26.
-
Fauser BCJM, Diedrich K, Bouchard P, Dominiguez F, Matzuk M, et al. (2011) Contemporary genetic Dwajani S and Rupakala BM. Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome. J Gynecol 2019, 4(2): 000179. technologies and female reproduction. Human Reproduction Update 17(6): 829-847.
-
Teede H, Deeks A, Moran L (2010) Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impact on health across the lifespan. BMC Medicine 8: 41.
-
Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, et al. (2004) The prevalence and features of polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab 89(6): 2745- 2749.
-
Boomsma CM, Fauser BC, Macklon NS (2008) Pregnancy complications in women with polycystic ovary syndrome. Semin Reprod Med 26(1): 72-84.
-
Goldenberg N, Glueck C (2008) Medical therapy in women with polycystic ovary syndrome before and during pregnancy and lactation. Minerva Ginecol 60(1): 63-75.
-
Moran LJ, Hutchison SK, Norman RJ, Teede HJ (2011) Lifestyle changes in women with polycystic ovary syndrome. The Cochrane Library 16(2): CD007506.
-
Trolice MP (2011) Defining prediabetes in polycystic ovarian syndrome. Open Journal of Obstetrics and Gynecology 1: 36.
-
Chaoyang Li ESF, Guixiang Zhao, Mokdad Ali H (2008) Prevalence of Pre-Diabetes and Its Association with Clustering of Cardio metabolic Risk Factors and Hyperinsulinemia Among U.S. Adolescents: National Health and Nutrition Examination Survey 2005–2006. Diabetes Care 32(2): 342-347.
-
Goodarzi MO, Azziz R (2006) Diagnosis, epidemiology and genetics of the polycystic ovary syndrome. Best Practice and Research 20(2): 193-205.
-
Hsu MI, Liou TH, Chou SY, Chang CY, Hsu CS (2007) Diagnostic criteria for polycystic ovary syndrome in Taiwanese Chinese women: comparison between Rotterdam and NIH 1990. Fertil Steril 88(3): 727-729.
-
Rotterdam ESHRE/ASRM Sponsored PCOS Consensus Workshop Group (2004) Revised 2003 consensus on the diagnostic criteria and long term health risks related to polycystic ovary syndrome. Hum Reprod 81(1): 19-25. Copyright© Dwajani S and Rupakala BM.
-
Carmina E (2004) Diagnosis of polycystic ovary syndrome: from NIH criteria to ESHRE-ASRM guidelines. Minerva ginecologica 56(1): 1-6.
-
Hart R, Hickey M, Franks S (2004) Definitions, prevalence and symptoms of polycystic ovaries and polycystic ovary syndrome. Best Practice & Research Clinical Obstetrics & Gynecology 18(5): 671-683.
-
Fallat ME, Siow Y, Marra M, Cook C, Carillo A (1997) Mullerian inhibiting substance in follicular fluid and serum: a comparison of patients with tubal factor infertility, polycystic ovary syndrome and endometriosis. Fertil Steril 67(5): 962-965.
-
Cook CL, Siow Y, Brenner AG, Fallat ME (2002) Relationship between serum mullerian- inhibiting substance and other reproductive hormones in untreated women with polycystic ovary syndrome and normal women. Fertil Steril 77(1): 141-146.
-
Laven JS, Mulders AG, Visser JA, Themmen AP, De Jong FH, et al. (2004) Anti-Mullerian hormone serum concentrations in normoovulatory and anovulatory women of reproductive age. J Clin Endocrinol Metab 89: 318-323.
-
Cate RL, Mattaliano RJ, Hession C, Tizard R, Farber NM, et al. (1986) Isolation of the bovine and human genes for Mullerian inhibiting substance and expression of the human gene in animal cells. Cell 45(5): 685-698.
-
Durlinger AL, Gruijters MJ, Kramer P, Karels B, Ingraham HA, et al. (2002) Anti-Mullerian hormone inhibits initiation of primordial follicle growth in the mouse ovary. Endocrinology 143(3): 1076-1084.
-
Weenen C, Laven JS, Von Bergh AR, Cranfield M, Groome NP, et al. (2004) Anti-Mullerian hormone expression pattern in the human ovary: potential implications for initial and cyclic follicle recruitment. Mol Hum Reprod 10: 77-83.
-
Pigny P, Merlen E, Robert Y, Cortet Rudelli C, Decanter C, et al. (2003) Elevated serum level of anti-mullerian hormone in patients with polycystic ovary syndrome: relationship to the ovarian follicle excess and to the follicular arrest. J ClinEndocrinol Metab 88(12): 5957-5962.
-
Tulika Singh, Sanju Sharma, Seetharamiah Nagesh (2017) Socio-economic status scales updated for 2017. J Res Med Sci 5(7): 3264-3267. Dwajani S and Rupakala BM. Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome. J Gynecol 2019, 4(2): 000179.
-
Polson DW, Wadsworth J, Adams J, Franks S (1988) Polycystic Ovaries: a common finding in normal women. The Lancet 1(8590): 870-872.
-
Cook CL, Siow Y, Brenner AG, Fallat ME (2002) Relationship between serum mullerian- inhibiting substance and other reproductive hormones in untreated women with polycystic ovarian syndrome and normal women. Fertility and Sterility 77(1): 141- 146.
-
Wei CL, Jayagopal V, Kilpatrick E, Holding S, Atkin SL (2006) The LH/FSH ratio has little use in diagnosing polycystic ovarian syndrome. Annals Clinical Biochem 43(3): 217-219.
-
Stephanie Mohammed, Shivananda Nayak B (2017) Exploration of ovarian hormones, diet and lifestyle of women with Polycystic ovarian syndrome. International Journal of Current Advanced Research 6(1): 1671-1675.
-
Balen AH, Conway GS, Kaltsas G, Techatrasak K, Manning PJ, et al. (1995) Polycystic ovary syndrome: the spectrum of the disorder in 1741 patients. Human Reproduction 10(8): 2107-2111.
-
Chang WY, Knochenhauer ES, Bartolucci AA, Azziz R (2005) Phenotypic spectrum of polycystic ovarian syndrome:clinical and biochemical characterization of the three major clinical subgroups. Fertility Sterility 83(6): 1717-1723.
-
Rondanelli M, Perna S, Faliva M, Monteferrario F, Repaci E, et al. (2014) Focus on metabolic and nutritional correlates of polycystic ovary syndrome and update on nutritional management of these critical phenomena. Archives of gynaecology and obstetrics 290(6): 1079-1092.
-
Alili A, Idrizi EA (2014) Clinical and Biochemical characteristics in women with polycystic ovarian syndrome in the region of Pollog, Republic of Macedonia. European Scientific Journal.
-
Douglas CC, Norris LE, Oster RA, Darnell BE, Azziz R, et al. (2006) Difference in dietary intake between women with polycystic ovary syndrome and healthy controls. Fertility and sterility 86(2): 411-417.
-
Kitzinger C, Willmott J (2002) The thief of womanhood: women's experience of polycystic ovarian syndrome. Social science & medicine 54(3): 349-361. Copyright© Dwajani S and Rupakala BM.
-
Braun V, Wilkinson S (2005) Vagina equals woman? On genitals and gendered identity. Women's Studies Dwajani S and Rupakala BM. Exploration and Comparison of Ovarian Hormones with Anti-Mullerian Hormone amongst Women with Polycystic Ovarian Syndrome. J Gynecol 2019, 4(2): 000179. International Forum 28(6): 509-522. Copyright© Dwajani S and Rupakala BM.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’