Bilateral Alive Tubal Ectopic Pregnancy and its Management
Ectopic pregnancy is an important cause of maternal mortality. Bilateral tubal pregnancies are rare; The reported incidence is only 1 in 200 000 pregnancies. Detecting bilateral tubal ectopic pregnancy is urgent because of the associated morbidity and mortality1 The management of bilateral tubal ectopic pregnancies may be medical or surgical, and depends to a large extent on the state of the fallopian tubes at presentation. The main challenge being to identify and treat as early as possible .Risk factors for ectopic pregnancy comprises of previous ectopic pregnancy, tubal damage secondary to tubal surgery, Adhesions secondary to previous laparotomies, chronic infection and Endometriosis. Other nonspecific factors that might contribute to an increased risk are cigarette smoking, age more than 35 years, and use of Assisted reproductive technology( ovulation induction). Presentation to the health care services may varies widely from mild vaginal bleeding and lower back and abdominal pain to clinically unstable condition and shock due to ruptured ectopic and life threatening internal bleeding.
Introduction
Diagnosis of ectopic pregnancy is not always straight forward. As a rule of thumb, any pregnant female reporting to emergency room with abdominal pain in early pregnancy should always raise the suspicion of Ectopic pregnancy until proved otherwise. Trans vaginal Ultrasound is playing a paramount role in the diagnosis where one can see an intact or ruptured ectopic confidently. In some cases where the diagnosis is not clear and patient is clinically stable, repeat BHCG(Q) after 48 hours to see the optimal rise is an option as well. In case of Spontaneous bilateral tubal ectopic pregnancies without previous induction of ovulation event which is extremely rare, diagnosis is rarely confirmed before surgery, therefore Careful examination of the tubes and of the abdomen is necessary to avoid missing bilateral ectopic and Heterotopic pregnancies. Another important factor in this context is the choice of management and consideration of possible fertility sparing surgery, keeping in mind the potentially increased risk of persistent trophoblasts and recurrent ectopic pregnancy. Patient and the family should be well informed about the management and their views and opinion should be taken into consideration while planning for treatment.
In clinically stable patient intracardiac injection of potassium chloride with single or multiple dose regime of Methotrexate can be tried with much success while in symptomatic or clinically unstable patient surgical management will be considered suitable. Salpingostomy can be done if possible but patient should be well informed about the increase risk of future ectopic and its associated complications beforehand.
Case Report
A 37 years old G6P4+1, 6/52 weeks pregnant presented to ER with two day history of feeling unwell. She complained of bilateral Lower quadrant pain, on right side more severe than the left. Pain increased in intensity prior to presentation with associated Dizziness and loss of consciousness for 2 minutes. There were no associated sign and symptoms related to bowel and bladder and she never had any vaginal bleeding episode. Regarding her past Obstetric history, she deliver vaginally four times with manual removal of placenta, Last pregnancy was a missed miscarriage with spontaneous expulsion. She didn’t have any risks factor for Ectopic pregnancy.
On examination patient was conscious, alert, oriented to person place & time. She had normal vital signs but looked pale and in pain. There was considerable degree of distension and tenderness on palpation. On speculum examination no bleeding was found and cervix was closed, bimanual examination revealed bulky uterus and adnexal
fullness bilaterally.
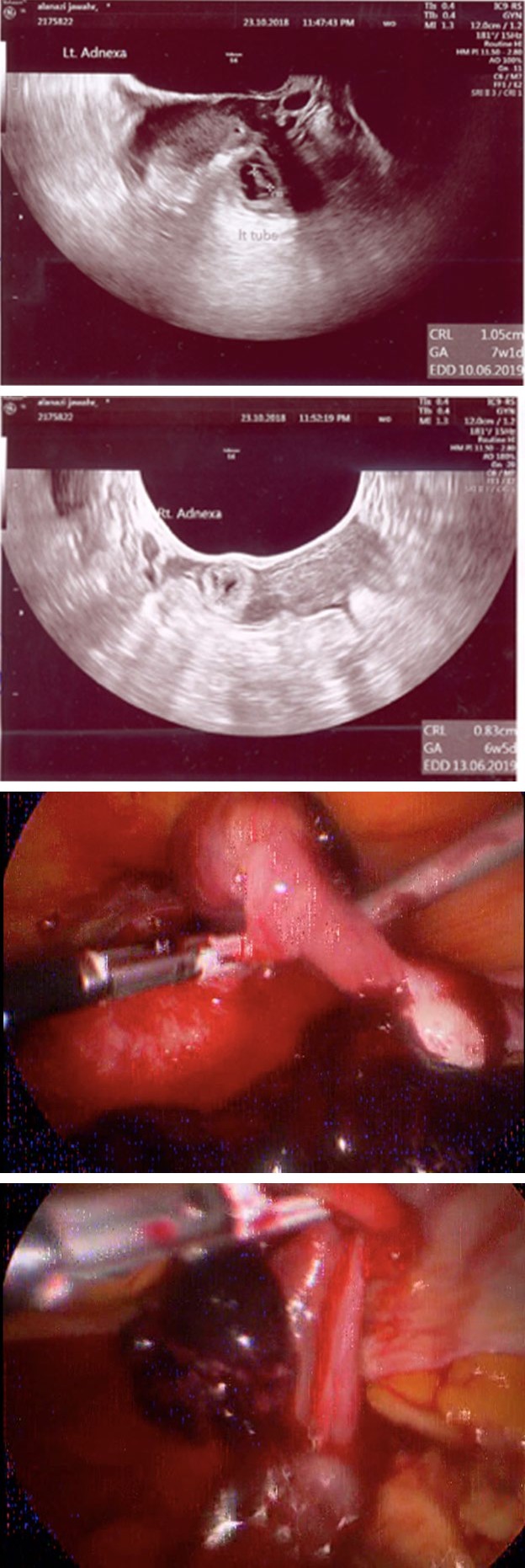
Her laboratory workup revealed hemoglobin of 122gm/ dl and total HCG was 98877iu. Urgent pelvic Ultrasound requested that has showed fluid filled Endometrium and no intrauterine pregnancy was seen. There was Right adnexal mass contains gestational sac measure=3.0X2.2cm with a viable fetus CRL 7mm=6wk (a) and a Left Adnexal mass containing gestational sac measure=3.2X2.4cm with a viable fetus corresponds to CRL 11mm=7wk (b). There was moderate amount of fluid in the pouch of Douglas with low level echoes.
Patient was informed about the findings and need for emergency surgery. Options of Laparoscopy v/s Laparotomy were discussed with the patient, all benefits, Risks & complications were explained thoroughly. Risk of recurrent ectopic in case of salpingostomy was explained. She was given time to discuss with her partner and they both consented for laparoscopic bilateral salpingectomy.
(a) (b)
(c) (d) Figure 1: Ectopic pregnancy.
Intra operatively, abdominal cavity was found full of clotted blood. On inspection finding of a right intact tubal ectopic pregnancy © and a left tubal ruptured ectopic pregnancy (d) were confirmed Bilateral salpingectomy (e) done using Ligasure. Patient tolerated the procedure well and had uncomplicated inpatient hospital course and OPD follow up afterwards.
Discussion
Ectopic pregnancy is still an important cause of maternal mortality. Although bilateral tubal ectopic pregnancy is very rare, and is usually the result of an assisted reproduction technique, yet its incidence is thought to be somewhere between 1 in 125 and 1 in 1580 extra-uterine pregnancies. In the UK about 11 in 1000 pregnancies are ectopic. The most recent Confidential Enquiry into Maternal Deaths, reports 11 deaths from this cause in the past triennium. Detecting bilateral tubal ectopic pregnancy is urgent because of the associated morbidity and mortality Recurrent ectopic pregnancies occur in 6–16 % of women with a previous history of ectopic pregnancy In recent years there has been a 3-fold increase due to the rapid growth in the number of women undergoing assisted reproductive techniques1. This has also resulted in a rise in bilateral tubal pregnancies.
Several theories have been postulated regarding the etiology of bilateral tubal ectopic pregnancy, with one proposed mechanism being the trans-peritoneal migration of trophoblastic cells. Foster, et al. [1] suggested that bilateral tubal pregnancy requires multiple ovulations to occur, the oocytes to be fertilized and the oocytes to implant at sites of tubal damage. Another theory describes a mechanism for superfetation, i.e., fertilization and development of a second oocyte in an already pregnant women [2] predisposing factors for occurrence of ectopic pregnancy include; early age of sexual intercourse, increased maternal age, multiple sexual partners, pelvic infections, history of infertility, use of fertility drugs, previous ectopic pregnancies and previous pelvic surgeries [3]. Patients with a familial history of twinning are considered to be at higher risk Twin ectopic pregnancies may involve one tube or both tubes [4].
Whether spontaneous or induced, the hallmarks of good management include early presentation, high index of suspicion, meticulous ultrasound scanning, good case selection, judicious intra-operative inspection of the contralateral tube, histology of specimens and appropriate patient counselling. The management of bilateral tubal ectopic pregnancies may be medical or surgical, and depends to a large extent on the state of the fallopian tubes at presentation. The main challenge being to identify and treat as early as possible those cases of ectopic pregnancy with the potential to cause serious morbidity and death, and at the same time minimize interventions in those destined to be resolved without causing any harm [3]. A study described the use of combined ultrasound-guided local injection of potassium chloride or methotrexate (MTX) and systemic MTX as an efficient nonsurgical option for women with tubal pregnancy, high serum β-hCG concentrations, and fetal cardiac activity [5].
Tubal ectopic pregnancy can be treated surgically by salpingectomy (removal of the affected fallopian tube) or salpingostomy (preservation of the affected tube) [2]. Despite the potentially increased risks of persistent trophoblasts and repeat ectopic pregnancy, salpingostomy is often preferred over salpingectomy because preservation of both tubes is assumed to offer better fertility prospects, although little evidence exists to support this assumption [6]. Laparoscopic surgical treatment is preferred to open procedures because the patient recovers more quickly and subsequent rates of intrauterine and ectopic pregnancy are similar.
Conclusion
Comprehensive clinical guidelines for the treatment of ectopic pregnancy have been published by the Royal College of Obstetricians and Gynecologists but because of its rarity, synchronous ectopic pregnancy management is not covered. For that reason management of these pregnancies should be evaluated and planned for each case. Patient and their family should be involved in each step of the treatment. Couple should have thorough counseling about the treatment options and the likely consequence for their future fertility.
Acknowledgement
We obtained permission & consent from the patients to publish this report with the pictures anonymously and ethical approval was granted by the Ethics Committee of the hospital.
References
-
Baijal N, Sahni M, Verma N (2007) Discordant twins with the smaller baby appropriate for gestational age– unusual manifestation of superfoetation, a case report. BMC Pediatr 7: 2.
-
Tabachnikoff R M, Dada M O, Woods R J, Rohere D, Myers C P, et al. (1998) Bilateral tubal pregnancy. A report of an unusual case. J Reprod Med 43(8): 707-709.
-
Jurkovic D (2007) Ectopic pregnancy. In: Edmonds DK, (Ed.), Dewhurst’s Textbook of Obstetrics and Gynaecology, 7th (Edn.), Massachusetts: Blackwell Publishing, pp: 106-116.
-
Ajayi GO, Agboola A, Coker O (1996) Cautionary case of unilateral twin tubal pregnancy. Niger J Surg Sci 6: 32-33.
-
Wang M, Chen B, Wang J. et al. (2014) Nonsurgical management of live tubal ectopic pregnancy by ultrasound-guided local injection and systemic methotrexate. J Minim Invasive Gynecol 21(4): 642-649.
-
Mol F, van Mello N M, Strandell A, European Surgery in Ectopic Pregnancy (ESEP) study group (2014) Salpingotomy versus salpingectomy in women with tubal pregnancy (ESEP study): an open-label, multicentre, randomised controlled trial. Lancet 383(9927): 1483- 1489.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’