An Update on COVID19 from Etiopathogenesis, to Role in Male Infertility, Pregnancy Lactation and Regarding Treatment
After our earlier review on COVID 19 in March here we further try to update what knowledge we have further gained on the subject. Currently we are amidst the worldwide pandemic of a new type of Coronavirus (COVID-19) that is going on, and originated from Wuhan, China and has now spread to 140 other countries including Japan, Korea, Italy, USA and UK.
Mini Review
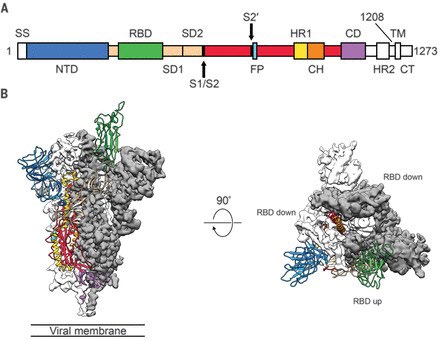
After our earlier review on COVID 19 in March here we further try to update what knowledge we have further gained on the subject. Currently we are amidst the worldwide pandemic of a new type of Coronavirus (COVID-19) that is going on, and originated from Wuhan, China and has now spread to 140 other countries including Japan, Korea, Italy, USA and UK. The World Health Organization (WHO) declared that COVID-19 has assumed pandemic proportions, causing severe respiratory tract infections (RTI) in humans. Doubtfully this originated from bats and somehow mutated and adapted human transmission (reviewed by us in [1]. Structurally it is similar to SARS-Co V with The spike(S) glyco protein of the Corona viruses being a class I viral fusion protein present on the outer envelope of the virion having a key role in viral infection by recognizing host cell receptors and modulating fusion of the viral as well as cellular membranes [2]. The Coronavirus S glyco protein gets synthesized as a precursor protein made up of ~1300 amino acids which then gets cleaved into an amino(N)terminal S1 subunit (~700 amino acids) as well as carboxy(C) terminal S2 subunit(600 amino acids). 3 S1/S2 heterodimers assemble to develop a trimer spike that protrudes via the envelope. The Cryo-EM structure of the 2019-nCoV spike in the pre-fusion conformation is demonstrated in (Figure 1) [3].
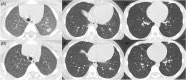
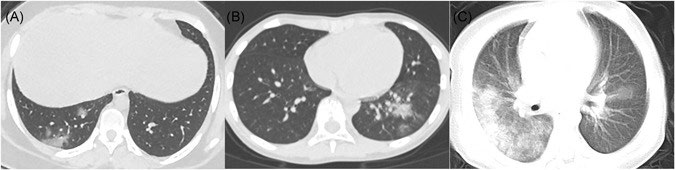
For diagnosis Rapid and proper finding of COVID-19 is important to control outbreaks in the community as well as in hospitals [4]. Mainly Laboratory examination includes nasopharyngeal as well as oropharyngeal swab tests. For identification of patients, by RT PCR-. The commonest symptoms were fever, cough, expectoration, headache, myalgia or fatigue, diarrhea and haemoptysis. Some people might experience Severe acute respiratory syndrome (SARS). Other organs are also susceptible to COVID-19. The single cell RNA-seq data was utilized for evaluating angiotensin converting enzyme 2( ACE2) expression for telling the potential risk of various human organs to COVID-19 infection.COVID-19 uses the same cell entry receptor like SARS-CoV, ACE2, that regulates both cross-species as well as human-human transmissions. COVID19-infection should be diagnosed with typical chest computed tomography (CT) characteristics in spite of negative RT-PCR results [5]. Of 1014 patients, 59% had RT-PCR positive, while 88% had positive chest CT scans [6]. Coronavirus belongs to the Corona viridae family; hence it does not come as a surprise those imaging findings, which are similar to those of SARS-CoV2 as well as MERS-CoV [1]. Typical CT findings are bilateral pulmonary parenchymal ground glass and consolidative pulmonary opacities, sometimes with a rounded morphology and peripheral lung distribution [5, 1]. But in pediatric patients (Figure 2), Procalcitonin elevation and consolidation with surrounding halo signs were common which were different from adults. It is suggested that underlying confection may be more common in pediatrics, and the consolidation with surrounding halo sign which is considered as a typical sign in pediatric patients.Further for investigating the occurrence of olfactory and gustatory dysfunctions in patients with laboratory confirmed COVID-19 infection and further faecal dissemination was proven[7, 8]. Lechien, et al. [8] added in European study, the sudden anosmia or ageusia need to be recognized by the international scientific community as important symptoms of COVID-19 infection [9]. Further Solaimanzadeh, with point of view of early treatment differently, with a perspective on pathophysiology, he tried to emphasize the problems in COVID-19 related to another respiratory illness, including high altitude pulmonary oedema (HAPE and how use of acetazolamide, ifedipine and PDE-Inhibitors need to be tried with the view of pulmonary oedema like picture instead of straight intubation and PEEP [10].
What We Have Learnt about Etiopathophysiology Since the Advent of COVID19
In individuals who suffer from COVID-19, a clinical syndrome has been observed which is considered as a main mechanism that is able to lead to the breakdown of the lungs, cardiovascular system, kidneys and liver. That syndrome is known as Cytokine Release Syndrome (CRS), and has been observed in other pathological conditions that activate the immune system to an extensive level, such as various infections or treatments that are able to over activate the immune system [11]. CRS is the leading cause of serious morbidity in patients infected with SARS-CoV and MERS- CoV. Elevated serum Interleukin (IL) -6 levels have been found in patients with SARS-CoV-1, with which SARS-CoV-2 is closely linked, and are associated with respiratory failure, Acute Respiratory Distress Syndrome (ARDS), and poor clinical outcome [12, 13]. It has been estimated that 20% of COVID-19 patients will have severe symptoms of pneumonia, leading to ARDS [14]. This complication is similar to the ARDS caused by the release of cytokines and the Haemophagocytic LymphoHistiocytosis Syndrome (HLHS) previously observed in patients with SARS-CoV and MERS-CoV as well as patients with B acute lymphoblastic leukemia receiving genetically modified autologous T-lymphocytes (CAR-T cells).
CRS is the leading cause of serious morbidity in patients infected with SARSCoV and MERS-CoV infections, and elevated levels of Il-6 and other inflammatory cytokines and chemokines have been identified in patients with the mentioned infections [12, 13]. An elevated level of serum C-Reactive Protein (CRP), an acute-phase protein whose expression depends on IL-6 which is released by macrophages and T cells, is also an indicator of severe CoV infection. IL-6 is a pro-inflammatory mediator as promotes inflammation and its signaling pathways include the classic cis- and Trans signaling pathway [15]. In cis pathway, IL-6 binds to the membrane-bound IL-6 receptor (mIL-6R) and forms a complex with the gp130 membranic glycoprotein, which is expressed in all cells, whereas the mIL-6R receptor expression is limited in the immune system cells. The downstream signaling pathway is mediated by the JAK/ STAT3 family kinases, and its activation leads to various effects in the innate / non-adaptive and mainly in the adaptive immune system. The final results is that B, T- lymphocytes and neutrophils, macrophages and NK killers, can be implicated in CRS development [15]. In Trans signaling pathway, IL-6 binds to its soluble receptor, IL-6R (sIL-6R), and forms a complex with gp 130, on all cells membrane surface. IL-6/ sIL-6R/JAK-STAT3 signaling pathway is activated even in cells which do not normally express the mIL-6 receptor, such as endothelial cells and leads to a systematic “cytokine storm” which contains the Vascular Endothelial Growth Factor (VEGF), Monocyte Chemo attractant Protein-1(MCP-1), IL-8, and additional IL-6 release, that leads to a reduced expression of E-cadherin in endothelial cells. Increased levels of VEGF in combination with decreased E-cadherin expression are responsible for an increased vascular permeability and “leakage”, mechanisms, that are implicated in the pathophysiology of hypotension and lung dysfunction in ARDS [16]. Based on the finding that lymphocytopenia is often observed in severe COVID-19 patients, the CRS caused by SARS-CoV-2 virus has to be mediated by leukocytes other than T cells, as it has been found in patients receiving CAR-T treatment. Therefore it is possible that lymphocytopenia is also associated with the clinical severity of the disease [17] and consists of a differential diagnostic criterion for COVID-19 [18]. However, lymphocytopenia has also been associated with a poor prognosis in other viral infections such as in influenza A H1N1 pandemic in 2009 [19] and cannot considered a specific biomarker for CoVid-19 poor prognosis.SARS-CoV-1 infects dendritic cells and monocytes, MERS-CoV infects monocytes and Tlymphocytes through the receptor of dipeptidyl peptidase 4 (DPP4) [20, 21], whereas recent studies suggest that SARS-CoV-2 also infects dendritic cells. Dendritic cells dysfunction leads to abnormal T-lymphocytes activation which in turn may lead to their reduction and apoptosis, conditions that may contribute to the immunopathology of COVID-19 [20, 22]. Infection of monocytes, macrophages, dendritic and T-lymphocytes by SARS-CoV-2 leads to their activation and release of IL-6, CRP and other inflammatory cytokines and chemokines. IL-6 also suppresses lymphocytes activation, and is associated with lymphopenia [22].
Histopathology of Lung Lesions
The lung lesions of SARS patients are characterized by histopathological findings such as nonspecific inflammatory responses with edema and inflammatory cell infiltration, severe alveolar epithelial cells exfoliation, alveolar septal swelling, alveolar septa damage, and alveolar space infiltration in an organized manner. SARS‐CoV infection can cause pathological changes, degeneration, infiltration, and hyperplasia [23]. In a recent study by Tian, et al. [24] which presented two cases treated by lobectomy due to lung adenocarcinoma, were subsequently diagnosed with COVID-19. Histopathological examination indicated that, in addition to adenocarcinoma, the lungs of both patients showed edema, protein release, lung cells focal reactive hyperplasia, and local infiltration by inflammatory cellular components. In addition, none of the patient showed symptoms of pneumonia during the surgical procedure and, therefore, the observed findings demonstrate early stages of the pathologic anatomical picture of the lung during the development of COVID-19 pneumonia. As already has been referred the pathogenesis of SARS and MERS are not yet fully elucidated, and it seems that viral and host factors play a principal role in SARS‐CoV and MERS‐ CoV infections.
Treatment
Treatment although not known with the virus being novel, drugs tried and in trials have been antivirals like IFN-α, lopinavir/ritonavir as well as ribanivir for treating COVID-19. Darunavir, which is a second generation of HIV1 protease inhibitor. Favipiravir, a new kind of RNA-dependent RNA polymerase (RdRp) inhibitor is undergoing clinical trials for treating COVID-19. Remdesivir, a nucleoside analogue as well as broad spectrum antiviral, also has shown potential benefits inCOVID-19.The maximum drug used in recent new York break is remsedevir being tried by WHO in many countries along with Favipiravir, hydroxyl chloroquine, that are under trials by WHO in various countries like favirapir got legalized in japan[53]. Further Ivermectin an FDA-approved broad spectrum antiparasitic agent [54], was shown to be effective in vitro studies in Vero/hSLAM cells by Leon Cary. Although ICMR trials were being conducted on role of hydrxy chloroquine, now it has been approved for prophylaxis in health workers and aged people having susceptibility to COVID19. In India ICMR research done in Pune with in vitro and safety studies advised.
- All asymptomatic healthcare workers involved in containment and treatment of COVID19 and asymptomatic healthcare workers working in non- COVID hospitals/non-COVID areas of COVID hospitals/ blocks.
- Asymptomatic frontline workers, such as surveillance workers deployed in containment zones and paramilitary/police personnel involved in COVID-19 related activities.
- Asymptomatic household contacts of laboratory confirmed cases [55].
Moreover in India ICMR has started a trial with certain botanical plants besides traditional ayurvedic medicines like turmeric etc. Convalescent plasma transfusion was delivered early following symptoms onset in the therapy of SARS [56]. Till date lot of successful transfers done in USA and lots in India.
As far as vaccines are concerned with structure of SARS- CoV2 S protein known, might help in the rapid generation Most of the vaccines getting developed for Coronaviruses target the spike glycoproteins or S proteins [57]. But watching the progress with Ebola vaccine that took 3 years still not marketed it seems some companies have skipped animal trials and still as far as reports come not before January 2021 new vaccines will come A ray of hope has come from placental expanded cells that Pluristem Diagnostics is conducting in Israel and possibly with it helping immune metabolism and helping in proteins formation might help in preventing severe lung inflammation, renal and other toxicities. Earlier PEX have been used for muscle regeneration in injuries etc. [58]. Still lockdown the most intelligent decision taken by our PM. Social distancing remains important till we get over this pandemic .Further some studies are being conducted to see if BCG has any protective effect with compulsory immunization in India, Pakistan, Bangladesh having <severe attacks is being studied. Probable explanation might be that these non-specific effects (NSEs) of the Bacille Calmette-Guérin (BCG) vaccine, for instance, implicate adaptive and innate immune mechanisms, with recent evidence suggesting that trained immunity might be a key instrument at play [59]. Collectively referring to the memory-like characteristics of innate immune cells, trained immunity stems from epigenetic reprogramming that these innate immune cells undergo following exposure to a primary stimulus like BCG. The epigenetic changes subsequently regulate cytokine production and cell metabolism and in turn, epigenetic changes are regulated by these effects In india vaccines being produced are also taking advantage of using measles vaccine having compulsion as carrier of Covid virus antigen so that well tolerated.
Role in Male Fertility
It has been confirmed that COVID-19 has the characteristic of human-to-human transmission, mainly through respiratory droplets and contact. Other routes require further verification. The virus responsible for COVID-19, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been detected in stool, gastrointestinal tract, saliva, and urine samples.2However, little is known about SARS-CoV-2 in semen. In this cohort study Li et al., found that SARS-CoV-2 can be present in the semen of patient’s withCOVID-19, and SARS-CoV-2 may still be detected in the semen of recovering patients. Owing to the imperfect blood- testes/deferens/epididymis barriers, SARS-CoV-2 might be seeded to the male reproductive tract, especially in the presence of systemic local inflammation. Even if the virus cannot replicate in the male reproductive system, it may persist, possibly resulting from the privileged immunity of testes. So far, researchers have found 27 viruses associated with viremia in human semen. But the presence of viruses in semen may be more common than currently understood and traditional non–sexually transmitted viruses should not be assumed to be totally absent in genital secretions. 5,6 Studies on viral detection and semen persistence are beneficial to clinical practice and public health, especially concerning viruses that could cause high mortality or morbidity, such asSARS-CoV-2.This study is limited by the small sample size and the short subsequent follow-up. Therefore, further studies are required with respect to the detailed information about virus shedding, survival time, and concentration in semen [60].
If it could be proved that SARS-CoV-2 can be transmitted sexually in future studies, sexual transmission might be a critical part of the prevention of transmission, especially considering the fact that SARS-CoV-2was detected in the semen of recovering patients. Abstinence or condom use might be considered as preventive means for these patients. In addition, it is worth noting that there is a need for studies monitoring fetal development. Therefore, to avoid contact with the patient’s saliva and blood may not be enough, since the survival of SARS-CoV-2 in a recovering patient’s semen [60].
While contrarily as the coronavirus disease 2019 (COVID-19) pandemic rages across the world, the scientific community continues to study the pathophysiology of the SARS-Cov-2 virus to provid guidance on disease transmission, susceptibility, and treatment. The disease is a respiratory infection and is known to lead to the expected symptoms, including fever, cough, and shortness of breath [61]. A highly contagious virus, SARSCov-2 is detected in the nasal secretions, sputum, feces, and rarely in the blood (1%) of infected individuals although not in the urine [62]. Cardiac, ocular, and neurologic symptoms of COVID-19 have been reported, but the reproductive implications of coronavirus infection remain unknown. As the reports have documented higher rates of infection, morbidity, and mortality among male patients, attention has shifted to potential male genetic susceptibility. Scientists have identified the main path for coronavirus entry into the cell-namely via the viral spike (S) protein attaching to the angiotensin-converting enzyme 2 (ACE2) and employing the cellular serine protease (TMPRSS2) for S protein priming, both of which are known to be present in the testis [63]. Thus, concern has arisen regarding infection of the testes and possible sexual transmission.
In their current report, Pan, et al. [64] address these separate but related questions regarding the possible testicular manifestations of COVID-19. Among the 34 men studied, no detectable SARS-Cov-2 was identified in the semen via reverse-transcription polymerase chain reaction. This is reassuring regarding possible viral transmission or lack thereof. However, it is important to note that the men studied were often several weeks removed from acute infections, and many had had only mild symptoms, so it is conceivable that earlier time points or higher viral loads could lead to different results. But given the normal time course of semen turn over, that appears less likely. Given the known mechanisms of SARS-Cov-2 entry into cells and the requirement for dual expression of ACE and TMPRSS2 proteins, the authors used their existing single cell RNA seq cellular data to show that only 4 of 6,490(<0.1%) testicular cells contain RNA for both proteins. Thus, it appears unlikely that SARS-Cov-2 can enter into any cells in the testis (e.g., germ cells, Ley dig cells, or Sertoli cells) as has been hypothesized.
Next, Pan, et al. [64] reported another interesting and novel clinical observation: 6 (17.6%) of 34 men reported scrotal discomfort at the time of COVID-19 infection. Previously reports on the symptoms of COVID-19 centered on the stigmata of severe systemic or respiratory illness. This novel scrotal observation should be confirmed, but it may improve future screening and should be further studied to understand the pathophysiology as well as the reproductive sequelae in men. Indeed, the current report was not able to assess any changes in semen quality among the participants, so it remains unknown how or whether the fecund ability of infected men is impaired. Prior data from other febrile illnesses have demonstrated that acute illness and elevated body temperatures (i.e., fevers) can temporarily lower spermatogenesis. Whether COVID-19 follows this model remains to be elucidated. In addition, more than 80% of those who are infected by the COVID-19 are asymptomatic, so the reproductive implications for these men would likely be favorable but remain unknown. Nevertheless, the current report represents the first exploration of the association between SARS-Cov-2 and human fecund ability. How women are affected and what the consequences are for assisted and unassisted reproduction in the face of acute COVID-19 infection or recovery remains to be studied. But given the current impact of the pandemic on the world, the likelihood the virus will remain for some time, and the birth of over 100 million babies every year, the reproductive implications of SARS-Cov-2 should be further studied [65].
Pregnancy with COVID-19
The current COVID-19 pneumonia pandemic caused by SARS-CoV2 virus is spreading globally at a rapid rate with a reproduction number (RD) of 2-2.5, pointing that 2-3 persons will be infected from an index patient. Pregnant women with their foetuses represent a high risk population during infectious disease outbreaks [66]. Until March 16, 2020, outcome of 55 pregnant women infected with COVID-19 as well as 46 neonates have been documented in the literature, without any definite proof of vertical transmission [66]. Physiological as well as mechanical changes in pregnancy enhance susceptibility to infections in general, especially when the cardiorespiratory system is affected, and aid in fast progression to respiratory failure in the gravid. Moreover, the pregnancy bias towards T-helper 2 (Th2) system dominance that protects the fetus, makes the mother having higher vulnerability to viral infections, that are more effectively contained by the Th1 system. These special challenges make it imperative that an integrated approach is done for pregnancies affected by SARS-CoV2 virus [66].
Dashrath, et al. presented a review of pathophysiology as well as susceptibility, diagnostic challenge with reverse transcription polymerase chain reaction (RT PCR) assays, therapeutic controversies, intrauterine transmission and maternal-fetal complications. Fetal surveillance due to predisposition to intra uterine growth restriction (IUGR) as well as special attention to labour as well as delivery was addressed. Further, they concentrated on keeping frontline obstetric care providers safe principles of workplace segregation, responsible social distancing, and containment of cross-infection to health care providers, marked use of personal protective equipment judiciously as well as telemedicine. Their objective was to provide a framework that can be used by tertiary maternity units that manage pregnant women in the flux of a pandemic while maintaining the safety of the patient as well as health care provider at its core [66]. No evidence supports adverse birth outcomes, intrauterine infection, or vertical transmission of COVID-19 [67]. But viral infections can be acquired when the infant passes via the birth canal during vaginal delivery or via postpartum breast feeding [68].
Further Rasmussen et al. reported Coronavirus disease 2019 is an emerging disease with a rapid increase in cases and deaths since its first identification in Wuhan, China, in December 2019. Limited data are available about coronavirus disease 2019 during pregnancy; however, information on illnesses associated with other highly pathogenic coronaviruses (ie, severe acute respiratory syndrome and the Middle East respiratory syndrome) might provide insights into coronavirus disease 2019’s effects during pregnancy. Coronaviruses cause illness ranging in severity from the common cold to severe respiratory illness and death. Currently the primary epidemiologic risk factors for coronavirus disease 2019 include travel from mainland China (especially Hubei Province) or close contact with infected individuals within 14 days of symptom onset. Data suggest an incubation period of w5 days (range, 2e14 days). Average age of hospitalized patients has been 49e56 years, with a third to half with an underlying illness. Children have been rarely reported. Men were more frequent among hospitalized cases (54e73%). Frequent manifestations include fever, cough, myalgia, headache, and diarrhea. Abnormal testing includes abnormalities on chest radiographic imaging, lymphopenia, leukopenia, and thrombocytopenia. Initial reports suggest that acute respiratory distress syndrome develops in 17e29% of hospitalized patients. Overall case fatality rate appears to bew1%; however, early data may overestimate this rate. In 2 reports describing 18 pregnancies with coronavirus disease 2019, all were infected in the third trimester, and clinical findings were similar to those in no pregnant adults. Fetal distress and preterm delivery were seen in some cases. All but 2 pregnancies were cesarean deliveries and no evidence of in utero transmission was seen. Data on severe acute respiratory syndrome and Middle East respiratory syndrome in pregnancy are sparse. For severe acute respiratory syndrome, the largest series of 12 pregnancies had a case-fatality rate of 25%. Complications included acute respiratory distress syndrome in 4, disseminated intravascular coagulopathy in 3, and renal failure in 3, and secondary bacterial pneumonia in 2, and sepsis in 2 patients. Mechanical ventilation was 3 times more likely among pregnant compared with no pregnant women. Among 7 first-trimester infections, 4 ended in spontaneous abortion. Four of 5 women with severe acute respiratory syndrome after 24 weeks’ gestation delivered preterm. For Middle East respiratory syndrome, there were 13 case reports in pregnant women, of whom 2 were asymptomatic, identified as part of a contact investigation; 3 patients (23%) died. Two pregnancies ended in fetal demise and 2 were born preterm. No evidence of in utero transmission was seen in severe acute respiratory syndrome or Middle East respiratory syndrome. Currently no coronavirus-specific treatments have been approved by the US Food and Drug Administration. Because coronavirus disease 2019 might increase the risk for pregnancy complications, management should optimally be in a health care facility with close maternal and fetal monitoring. Principles of management of coronavirus disease 2019 in pregnancy include early isolation, aggressive infection control procedures, oxygen therapy, avoidance of fluid overload, consideration of empiric antibiotics (secondary to bacterial infection risk), laboratory testing for the virus and confection, fetal and uterine contraction monitoring, early mechanical ventilation for progressive respiratory failure, individualized delivery planning, and a team-based approach with multispecialty consultations. Information on coronavirus disease 2019 is increasing rapidly. Clinicians should continue to follow the Centers for Disease Control and Prevention website to stay up to date with the latest information.
Breast Feeding
Fernández-Carrasco et al. tried to study if any negative consequences during breastfeeding existed. The objective of this work is to investigate the action plan on breast feeding in postpartum women with SARS-CoV-2 and her newborn. They did a literature search via Medline, Web of Science, Scopus, BVS, and Cuiden databases. The methodological quality of the articles had been assessed using the “Grading of Recommendations Assessment, Development and Evaluation” (GRADE). This study has not been registered in PROSPERO.A total of 14 documents were found, of which 9 are observational empirical studies. Most of the studies were conducted in China, Italy, the USA, and Australia. A total of 114 mothers infected with coronavirus with their respective newborns were assessed. The analyzed investigations state that it is best for the newborn to be breastfed; given that mother’s milk samples were analyzed, detecting the presence of antibodies of the coronavirus in them, being a protective factor against infection. Thus concluding that Breastfeeding in postpartum women with SARS-CoV-2 is highly recommended for the newborn, if the health of the mother and newborn allow it. When direct breastfeeding is favored, the appropriate respiratory hygiene measures always have to be considered. Whether the mother’s health does not permit direct breastfeeding, her breast milk should be previously extracted and kept unpasteurized. To secure the newborn feeding, milk banks are also an appropriate option.
Conclusion
Here we have tried to update what we had not covered earlier along with newer facts as they keep on getting unraveled with COVID 19 now around for 6 months. The etiopathogenesis of ARDS has been more well understood that has dictated a change in attitude in how to approach a patient with ARDS like symptoms. Although in Oxford in UK have started some vaccine trials in UK was attempt-ted on 22/4/2020 it was a failure .However seeing the growing increases in pandemic with USA reaching >9 lakh currently with almost 90,000 deaths and need of early therapy is there. India although has got cases upto 1.9 lakh our cure rate is very high with 3 % mortality with a total of 5000 deaths till now. A ray of hope has come from placental expanded cells that Pluristem Diagnostics is conducting in Israel and possibly with it helping immune metabolism and helping in proteins formation might help in preventing severe lung inflammation, renal and other toxicities. Earlier PEX have been used for muscle regeneration in injuries etc. Still lockdown the most intelligent decision taken by our PM. Social distancing remains important till we get over this pandemic. Further some studies are being conducted to see if BCG has any protective effect with compulsory immunization in India, Pakistan, Bangladesh having <severe attacks is being studied. Probable explanation might be that these non-specific effects (NSEs) of the Bacille Calmette-Guérin (BCG) vaccine, for instance, implicate adaptive and innate immune mechanisms, with recent evidence suggesting that trained immunity might be a key instrument at play [19]. Collectively referring to the memory-like characteristics of innate immune cells, trained immunity stems from epigenetic reprogramming that these innate immune cells undergo following exposure to a primary stimulus like BCG. The epigenetic changes subsequently regulate cytokine production and cell metabolism and in turn, epigenetic changes are regulated by these effects. Further in India we use a lot of our routine herbal remedies which might help in enhancing immunity. In india vaccines being produced are also taking advantage of using measles vaccine having compulsion as carrier of Covid virus antigen so that well tolerated –God willing we will be able to fight with this in time specially with the claims of Pluristens that 100% recovery possible after they did some trials in Israel(unpublished observations).
References
-
Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2020) A Comprehensive review on epidemiology, aetiopathogenesis, diagnosis and treatment of the novel corona virus syndrome-COVID-19. Iberoamerican Journal Medicine.
-
Song W, Gui M, Wang X, Wiang Y (2018) Cryo-EM structure of the SARS Coronavirus spike glyco protein in complex with its host cell receptor ACE2. PLoS Pathogens 14(8): E1007236.
-
Wrapp D, Wang N, Corbett KS, Goldsmith JA, Hsieh CL, et al. (2020) Cryo-EM structure of the 2019-nCoV spike in the pre-fusion conformation. Science 367(6483): 1260- 1263.
-
To KK, Tang OT, Chik-Yan Yip C, Chan KH, Wu TC, et al. (2020) Consistent detection of 2019 novel Coronavirus in saliva. Clin Infect Dis 71(15): 841-843.
-
Xie X, Zhong Z, Zhao W, Zheng C, Wang F, et al. (2020) Chest CT for typical 2019-nCoV pneumonia: relationship to negative RT- PCR testing. Radiology 296(2): E41-E45.
-
Ai T, Yang Z, Hou H, Zhan C, Chen C, et al. (2020) Correlation of chest CTand RT-PCR testing in Coronavirus disease 2019(COVID-19) in China :A report of 1014 cases. Radiology 296(2): E32-E40.
-
Xia W, Shao J, Guo Y, Peng X, Li Z, et al. (2020) Clinical and CT Features in Pediatric Patients With COVID-19 Infection: Different Points From Adults. Pediatr Pulmonol 55(5): 1169-1174.
-
Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, et al. (2020) Olfactory and gustatory dysfunctions as a clinical presentation of mild-to moderate forms of the Coronavirus disease 2019(COVID-19):A Multicenter European Study. Otorhino laryngol, pp: 1-11.
-
Solaimanzadeh I (2020) Acetazolamide, nifedipine and phosphodiesterase inhibitors:Rationale for Their Utilization as adjunctive Countermeasures in the Treatment of Coronavirus disease 2019(COVID-19). Cureus 12(3): e7343.
-
Moore JB, June CH (2020) Cytokine release syndrome in severe COVID-19. Science 368(6490): 473-474.
-
Chen G, Wu D, Guo W, Cao Y, Huang D, et al. (2020) Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest 130(5): 2620- 2629.
-
Ruan Q, Yang K, Wang W, Jiang L, Song J (2020) Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med 46(5): 846-848.
-
Wu Z, McGoogan JM (2020) Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 323(13): 1239- 1242.
-
Kang S, Tanaka T, Narazaki M, Kishimoto T (2019) Targeting Interleukin-6 Signaling in Clinic. Immunity 50(4): 1007-1023.
-
Tanaka T, Narazaki M, Kishimoto T (2016) Immunotherapeutic implications of IL-6 blockade for cytokine storm. Immunotherapy 8(8): 959-970.
-
Yang X, Yu Y, Xu J, Shu H, Xia J, et al. (2020) Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir Med 8(5): 475-481.
-
Wang Y, Chen X, Cao W, Shi Y (2014) Plasticity of mesenchymal stem cells in immunomodulation: pathological and therapeutic implications. Nat Immunol 15(11): 1009-1016.
-
Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, et al. (2009) Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med 361(7): 680-689.
-
Chu H, Zhou J, Wong BH, Li C, Chan JF, et al. (2016) Middle East Respiratory Syndrome Coronavirus Efficiently Infects Human Primary T Lymphocytes and Activates theExtrinsic and Intrinsic Apoptosis Pathways. J Infect Dis 213(6): 904-914.
-
Law HK, Cheung CY, Ng HY, Sia SF, Chan YO, et al. (2005) Chemokine up-regulation in SARS-coronavirus-infected, monocyte- derived human dendritic cells. Blood 106(7): 2366-2374.
-
Zheng M, Gao Y, Wang G, Song G, Liu S, et al. (2020) Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol 17(5): 533-535.
-
Li G, Fan Y, Lai Y, Han T, Li Z, et al. (2020) Coronavirus infections and immune responses. J Med Virol 92(4): 424-432.
-
Sufang Tian, Weidong Hu, Li Niu, Huan Liu, Haibo Xu, et al. (2020) Pulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients With Lung Cancer. J Thor Oncol 15(5): 700-704.
-
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, et al. (2020) Clinical characteristics of 2019 novel coronavirus infection in China. N Engl J Med.
-
Dan H, Maureen G, Richard B, Clark KL (2020) Quantitative mRNA expression profiling of ACE 2, a novel homologue of angiotensin converting enzyme. FEBS Letters 532(2): 107-110.
-
Letko M, Marzi A, Munster V (2020) Functional assessment of cell entry and receptor usage forSARS- CoV-2 and other lineage B betacoronaviruses. Nat Microbiol 5: 562-569.
-
Mossel EC, Wang J, Jeffers S, Edeen KE, Wang S, et al. (2008) SARS-CoV replicates in primary human alveolar type II cell cultures but not in type I-like cells. Virology 372(1): 127-135.
-
Weinheimer VK, Becher A, Tonnies M, Holland G, Knepper J, et al. (2012) Influenza A viruses target type II pneumocytes in the human lung. J Infect Dis 206(11): 1685-1694.
-
Wang D, Hu B, Hu C, Zhu F, Liu X, et al. (2020) Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 323(11): 1061-1069.
-
Lin L, Lu L, Cao W, Li T (2020) Hypothesis for potential pathogenesis of SARS-CoV-2 infection–a review of immune changes in patients with viral pneumonia. Emerg Microbes Infect 9(1): 727-32.
-
Wan SX, Yi QJ, Fan SB, Lv J, Zhang X, et al. (2020) Characteristics of lymphocyte subsets and cytokines in peripheral blood of 123 hospitalized patients with 2019 novel coronavirus pneumonia (NCP). medRxiv
-
Qian Z, Travanty EA, Oko L, Edeen K, Berglund A, et al. (2013) Innate immune response of human alveolar type II cells infected with severe acute respiratory syndrome-coronavirus. Am J Respir Cell Mol Biol 48(6): 742-748.
-
Mason RJ (2020) Pathogenesis of COVID-19 from a cell biologic perspective. Eur Respir J, Article ID: 2000607.
-
Kumar PA, Hu Y, Yamamoto Y, Hoe NB, Wei TS, et al. (2011) Distal airway stem cells yield alveoli in vitro and during lung regeneration following H1N1 influenza infection. Cell 147(3): 525-538.
-
Yee M, Domm W, Gelein R, Bentley KL, Kottmann RM, et al. (2017) Alternative Progenitor Lineages Regenerate the Adult Lung Depleted of Alveolar Epithelial Type 2 Cells. Am J Respir Cell Mol Biol 56(4): 453-464.
-
Gu J, Korteweg C (2007) Pathology and pathogenesis of severe acute respiratory syndrome. Am J Pathol 170(4): 1136-1147.
-
Xu Z, Shi L, Wang Y, Zhang J, Huang L, et al. (2020) Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med 8(4): 420-422.
-
Jin Y, Yang H, Ji W, Wu W, Chen S, et al. (2020) Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 12(4): 372.
-
Takada A, Kawaoka Y (2003) Antibody-dependent enhancement of viral infection: molecular mechanisms and in vivo implications. Rev Med Virol 13(6): 387-398.
-
Wang J, Hajizadeh N, Moore EE, McIntyre RC, Moore PK, et al. (2020) Tissue Plasminogen Activator (tPA) Treatment for COVID-19 Associated Acute Respiratory Distress Syndrome (ARDS): A Case Series. J Thromb Haemost 18(7): 1752-1755.
-
Galván Casas C, Català A, Carretero Hernández G, Rodríguez-Jiménez P, Fernández Nieto D, et al. (2020) COVID-19: A Rapid Prospective Nationwide Consensus Study in Spain With 375 Cases. Br J Dermatol.
-
Rustin MHA (1986) Nifedipine in the treatment of chilblains. Br Med J 293(6552): 923-924.
-
Goette D (1990) Chilblains (Perniosis). J Am Acad Dermatol 23: 257-262.
-
Hedrich CM, Fiebig G, Hauck FH, Sallmann S, Hahn G, et al. (2008) Chilblain lupus erythematosus: a review of literature. Clin Rheumatol 27(10): 949-954.
-
Sifuentes Giraldo WA, Ahijón Lana M, García Villanueva MJ, González Garcíá C, Vásquez Diaz M (2012) Chilblain lupus induced by TNF-alpha antagonists: acase report and literature review. Clin Rheumatol 31(3): 563-568.
-
Prakash S, Weisman MH (2009) Idiopathic chilblains. Am J Med 122(12): 1152-1155.
-
Yang X, Perez OA (2010) Successful treatment of perniosis with hydroxychloroquine. J Drugs Dermatol 9(10): 1242-1246.
-
Gordon R, Arikiena AM, Pakula AS (2014) Chilblains in Southern California: two case reports and review of literature. J of Med Case Reports 8: 381.
-
Wilder Smith A, Freedman DO (2020) Isolation, quarantine, social distancing and community containment: pivotal role for old style public health measures in the novel Coronavirus (2019-nCoV) outbreak. J Travel Med: 27(2): 1-4.
-
Chen N, Zhou M, Dong X, Qu J, Gong F, et al. (2020) Epidemiological and Clinical characteristics of 99 cases of Wuhan, China: a descriptive study. Lancet 395(10223): 507-513.
-
Zou X, Chen K, Zou J, Han P, Hao J, et al. (2020) Single cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable in 2019-nCoV Infection. Front Med 14(2): 185-192.
-
Dong L, Shasha S, Gao J (2020) Discovering drugs to treat Corona virus disease 2019(COVID 19). Drug Discoveries &Therapeutics 14(1): 58-60.
-
Leon C, Julian DD, Mike GC, David AJ, Kylie M, et al. (2020) The FDAapprovedDrug Ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antiviral Research 178: 104787.
-
Du L, He Y, Zhou Y, Liu S, Zheng SJ, et al. (2009) The spike proteins of SARS-CoV-a target for vaccine and therapeutic development. Nat Rev Microbiol 7: 226-236.
-
Mair-Jenkins J, Saavedra-Campos M, Baillie JR, Cleary P, Khaw PM, et al. (2015) The effectiveness of convalescen t plasma and hyperimmune immunoglobulin for the treatment of Severe Acute respiratory infections of viral etiology:a systematic review and exploratory meta- analysis. J Infect Dis 211(1): 80-90.
-
Prather WR, Toren A, Meiron M (2008) Placental- derived and Expanded Mesenchymal Stromal Cells (PLX-I) to Enhance the Engraftment of Hematopoietic Stem Cells Derived from Umbilical Cord Blood. Expert Opin Biol Ther 8(8): 1241-1250.
-
Uthaykumar D, Paris S, Chapat L, Freyburger L, Poulet H, et al. (2018) Non-specific Effects of Vaccines Illustrated Through the BCG Example: From Observations to Demonstrations. Front Immunol 9: 2869.
-
Li D, Jin M, Bao P, Zhen W, Zheng X (2020) Clinical Characteristics and Results of Semen in Men with Corona virus Disease 2019. JAMA Network Open 3(5): e208292.
-
Wang D, Hu B, Hu C, Zhu F, Liu X, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 323(11): 1061-1069.
-
Wang W, Xu Y, Gao R, Lu R, Han K, et al. (2020) Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 323(18): 1843-1844.
-
Hoffmann M, Kleine-Weber H, Schroeder S, Kreuger N, Herrler T, et al. (2020) SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 181(2): 271-280.
-
Pan F, Xiao X, Guo J, Song Y, Li H, et al. (2020) No evidence of SARSCoV-2 in semen of males recovering from COVID-19. Fertil Steril 113(6): 1135-1139.
-
Eisenberg ML (2020) Corona virus Disease 2019 and mens reproductive health. Fertil Steril 113(6): 1154.
-
Dashraath P, Jeslyn WJL, Xian Karen LM, Min LL, Sarah L, et al. (2020) Corona virus Disease 2019 Pandemic and Pregnancy. Am J Obstet Gynaecol 222(6): 521-531.
-
Chen N, Guo J, Wang C, Luo F, Yu X, et al. (2020) Clinical characteristics and intrauterine vertical transmission potential of COVID 19 infection in nine pregnant women: a retrospective review of medical records. Lancet 395(10226): 507-513.
-
Schwartz DA, Graham AL (2020) Potential maternal and infant outcomes from (WuhanCoronavirus 2019-nCoV Infecting pregnant women: Lessons from SARS/ MERS and other human Coronavirus infection. Viruses 12(2): 194.
-
Rasmussen SA, Smulien JC, Lednicky JS, Wen TS, Jamieson DJ (2020) Corona virus Disease 2019 (COVID 19)and Pregnancy: What Obstetricians Need to Know. Am J Obstet Gynecol 222(5): 415-426.
-
Fernández-Carrasco FJ, Vázquez-Lara JM, Urbano González-M, Gómez-Salgado M, Parrón-Carreño T, et al. (2020) Corona virus COVID- 19 Infection and Breast feeding. Rev Esp Salud Publica 94: e202005055.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’