A Posit that Luteinizing Hormone Independent Escalation of Progesterone Might be the Physiological Trigger for the Gonadotrophins Surge in Case of Human Menstrual Cycle
The present ovarian cycle model posits that ovulation gets triggered by a crucially maintained escalation of estradiol. Nevertheless, a deep probing of the published literature besides the work of team of Dozortev, Diamond along with Pellicer, more specifically Dozortev DI demonstrated significant doubt about the relative parts of progesterone as well as estradiol in the event of ovulation. Here proof provided by Dozortev DI’s work is presented that gives so much proof regarding the part played by estradiol has been misrepresented till the day, whereas the actual ovulation trigger is the Luteinizing hormone independent preovulatory progesterone surge in the circulation to about 0.5mg/ml. Moreover the recent work accommodates with the present work on the capacity of progesterone for ovulation trigger with its clearly proven capacity of blocking ovulation at the time of pregnancy, or when delivered in the kinds of synthetic progestins in the form of Oral contraceptive pills in addition to the experimental results with regards to estradiol benzoate stimulates ovulation in the lack of progesterone.
Kulvinder Kochar Kaur1*, Gautam Allahbadia2 and Mandeep Singh3
Introduction
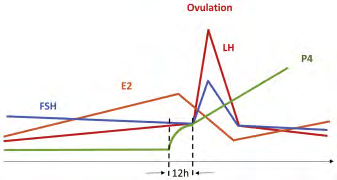
As per the present prototype models of ovulation the posit is that the escalation of estradiol (E2), into the range over200-300pg/ml for at least 50h is what results in the stimulation of gonadotropin releasing hormone (GnRH) to surge amounts. GnRH, further binds to its receptors existing In the anterior pituitary, resulting in liberation of follicle stimulating hormone (FSH) as well as Luteinizing hormone (LH) into the circulation, that finally ends in the rupture of the dominant follicles (DF) (Figure 1) [1].
Nevertheless, a recent prospective randomized study illustrated that if letrozole was delivered continuously right through the follicular phase ,with clearly validated repression of estradiol (E2), did not possess any influence on the ovulation timing in case of normally menstruating ladies. Thus Hurst, et al. [2] concluded that that part of E2 in ovulation had been misconstrued [3].
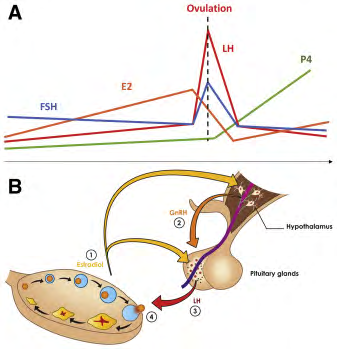
Figure1: Courtesy ref no-2-Current ovulation paradigm. (A) Schematic hormones interplay around ovulation and (B) the hypothalamic-pituitary-gonadal axis representation.
Noticeability, this was not the first finding that queried the part of E2 enhancement in the form of acting as a trigger for ovulation. Actually, it has been long known that at the time of controlled ovarian hyperstimulation (COS), a supra physiological E2 amounts get achieved quite early during the follicular phase, however it does not initiate ovulation. Moreover when the LH surge actually takes place, it is usually significantly decreased, that is not consistent with E2 working in the form of a trigger [4]. Moreover, escalation of circulating E2 amounts 10 fold (to around 13,000pmol/L) in contrast to the control by the delivery of exogenous E2, prior to ovulation. Zalanyi [5] further arrived at the conclusion that this theory of E2 resulting in ovulation needs to be given up [5]. Further another hormone that has been understood for long to initiate the LH surge has been progesterone (P). In 1964, Buchholz, et al. [6], were the 1st ones to demonstrate that administration of intramuscular injection of P resulted in an immediate escalation in urinary gonadotropins, akin to the gonadotropins peak observed at the time of ovulation. In agreement with this Odell as well Swerdloff [7], illustrated that injection of P promoted a LH as well as FSH surge in case of post-menopausal women following FSH down regulation with the utilization of an estradiol dosage. Inspite of these initial observations documenting the capacity of P, for stimulation of an ovulatory peak of gonadotropins, its part in the form of a physiological ovulation triggering agent has been not got appreciated till date. Probably this is secondary to Leydendecker’s, et al. [8], illustrated that estradiol benzoate can result in stimulation of an LH surge in case of women who had been castrated as well as total absence of any ovarian obtained P. Moreover, P has been acknowledged historically in the form of a LH suppressing hormone [5], in addition to that its artificially-obtained Progestin represent the primary constituent of the oral contraceptives (OCPs).
Further the preovulatory peak of P is apparently very little, just about 0.5ng/ml [9], in contrast to that with the post ovulatory escalation that is roughly 10 fold greater. The relatively small amount of the preovulatory peak makes it tough to appreciate its clinical significance. Further it can get easily ignored since it occurs within hrs, while practically all significant studies do the P sampling at daily basis. But for Hoff, et al. [9], conducted blood sampling 2 hrly in the day prior to ovulation was it feasible to watch that the P surge antecedes both the estradiol peak in addition to that of gonadotrophins flare by about 12hrs.
Another intrinsic limitation is to dissect the part of E2 as well as P is their intricate working in synergy, secondary to which E2 is needed for stimulation of P receptors in the hypothalamus [10].
Here effort has been done to get the proof together the part of P in the form of trigger for the gonadotrophins surge: the proof that as per Dozortsev D [2] is valid. They have compiled what they believe is pressurizing corroboration, that under normal physiological situation there is existence of 2 P waves. Of these the 1st wave is an LH independent a highly steepy escalation 12h prior to the gonadotrophins surge to roughly 0.5ng/ml, that signals towards the hypothalamus that the dominant follicles (DF) is prepared for rupture. This escalation causes stimulation of the GnRH signaling pathway, with a resultant LH /FSH surge that results in the follicle to rupture along with its granulosa cells to undergo luteinization.
Luteinization that is LH Independent, Meiosis Getting Resumed as well as Follicle Rupture
Luteinization that is LH Independent during Evolution
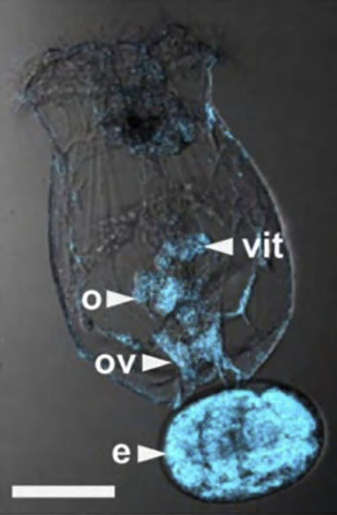
During Evolution, 1st luteinization got encountered at a minimum of 500 million years back as well as has continued till day in the form of a locally controlled process in lower animals (Figure 2) [11]. Despite mammals that include human beings, have generated a higher degree of luteinization regulation, there is considerable proof that the capacity of all granulosa cells that include cumulus cells, to undergo Luteinization spontaneously got retained in human beings [12].
Luteinization Represents Default Differentiation of all Granulosa Cells
In vivo all granulosa cells are seemingly bound to undergo luteinization but that is avoided from luteinization via a mode that has not been totally clarified. Nevertheless, despite all these details the sustenance of the block needs a basement membrane (BM) of the follicle that is totally intact [13]. On the integrity of the BM gets disturbed via inflammation, through activation of collagenase, or via escalation of intra follicular pressure [14], the GC’s get liberated from the differentiation block as well as get luteinized [15]. Intriguingly, the pace at which luteinization occurs in a follicle that is totally intact that has been separated from the ovary appears seemingly akin to the one occurring in presence/absence of LH. This robustly validates the point that the liberation from the block occurs secondary to alterations in the intrafollicular contents instead of stimulation of luteinization by LH [16]. In agreement with this posit, in case of hypophysectomized rats where total absence of LH exists, the follicles go through normal ovulation as well as luteinization following an FSH injection [16].
LH Independent, Meiosis Getting Resumed
In a significant article, Kubiac [17], posited that oocytes gradually acquire the capacity of fertilization following the, meiosis getting resumed as well as would get arrested at the so labeled MIII stage in case fertilization occurs prematurely. Akin to that at the time of follicular generation, the oocyte acquires for the capacity for resumption of meiosis at a minimum of a lot of days prior to ovulation in addition to prior to it acquiring generational competence [18] that gets defined as the capacity of generation till term on fertilization.
In case of physiological situations the LH surge results in the degeneration of the gap junction, generated by cumulus cells with the oolemma, besides among the ones among themselves. Occasionally the breakdown of these connections can be watched with ease in the form of debris beneath the Zona pellucida (ZP) (Figure 3), Nevertheless, any alterations in the follicular contents secondary to the deletion of follicular BM intactness would result in Spontaneous luteinization as well as breakdown of the gap junction with the akin outcomes; namely meiosis getting resumed as far as the oocytes has gained such capacity [19]. The exact time period of resumption of meiosis in such instances can be anticipated in lesser cases, in contrast to the physiological disturbances of the gap junction, that occurs concomitantly for all granulosa cells following a LH flare [20].
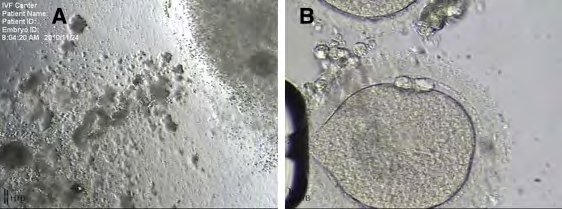
![Figure 3: Courtesy ref no-2-Debris from the degenerated gap junctions and corona cell pulled under the zona pellucida (arrow) resulting from failure of its gap junction degeneration. (From Dozortsev DI, unpublished data.) Like, a follicle that is about to undergo demise does not rupture, as well as the egg has resumption of meiosis secondary to cumulus cell demise in addition to acquiring a postmature look on retrieval of oocyte [unpublished Data Dozortsev DI] (Figure4).This kind of post maturity all the time represents a local process, like a post mature egg can get obtained by the side of the normal looking oocytes, in case of LH being well repressed [unpublished Data Dozortsev DI] (Figure 4).](/fulltextimages/7628/fig_3.png)
Figure 3: Courtesy ref no-2-Debris from the degenerated gap junctions and corona cell pulled under the zona pellucida (arrow) resulting from failure of its gap junction degeneration. (From Dozortsev DI, unpublished data.) Like, a follicle that is about to undergo demise does not rupture, as well as the egg has resumption of meiosis secondary to cumulus cell demise in addition to acquiring a postmature look on retrieval of oocyte [unpublished Data Dozortsev DI] (Figure4).This kind of post maturity all the time represents a local process, like a post mature egg can get obtained by the side of the normal looking oocytes, in case of LH being well repressed [unpublished Data Dozortsev DI] (Figure 4).
Follicle Rupture- LH independent
Ovarian follicles might rupture at end of follicular phase without LH The capacity of the ovarian follicles to rupture in the absence of a LH surge has got illustrated in case of hypophysectomized rats in a convincing fashion [16]. In case of in vitro fertilization (IVF), this process is termed as vanishing follicles, that takes place more often in elder subjects at the time of a cycle that has been stimulated [21]. This disappearance of follicles is usually escalation correlated with an escalation of circulating P to the post ovulatory amounts, despite on LH suppression [21]. Noticeably just the rupture of follicles, which have not been earlier not received exposure to LH (or HCG) can’t be believed to be ovulation provided it .It causes an egg to be liberated as as get available to a spermatozoa for fertilization. Although FSH has the capacity to initiate follicle to rupture, it is not correlated with gap junctions breaking down, that might cause the egg getting trapped within the ruptured follicle, or ovulation of an immature egg, or an egg that has the surroundings of tight cumulus cells that makes sperm penetration a virtual impossibility.
Part of LH Once rupture of follicles, meiosis getting Resumedin addition to luteinization of the granulosa cells have the capacity of occurring without LH, what is the precise need for the LH surge? Despite ovulatory processes can take place in absence of LH, an extremely low possibility of pregnancy is there in the absence of an intricate coordination in time, since there exists a relatively small viable fertilization window, which can result in a term pregnancy [22].
The exact timing period of the viable fertilization window in case of human beings is uncertain; Nevertheless, the experience with conducting day1 Intra Cytoplasmic Sperm Injection(ICSI)- illustrates with clarity that the maximum probability of an embryo generation is not existing following 24hr following oocyte pick up [23] or about 60hrs following an HCG injection . Dozortsevetal [22], illustrated that the maximum probability of an of an embryo generation till term gets reduced if fertilization occurs later than 41hrs post HCG, despite the probability of fertilization occuring keeps rising .Conversely if the penetration of the oocyte by sperm occurs prior to 37hrs subsequent to HCG, a reduction in fertilization in addition to pregnancy rates fall [22].
This implies that the human oocytes possesses the maximum probability of viable fertilization just within 4-5hrs subsequent to ovulation. Having the knowledge that ovulation occurs 36-37hrs post HCG, seemingly it is intricately associated with the ideal fertilization window, that implicates that the presumed messenger needs to watch the follicle’s pending rupture as wellas correlate with the GnRH to trigger the Luteinizing hormone surge.
As a part note the physiological LH surge has FSH to give it company all the time, hence usually called LH/FSH surge. It is unknown if a need for FSH truly exists for the rupture of follicle at this stage or is just a relative adverse action of LH surge, that by itself is enough to provoke rupture of follicle along with ovulation. The probability of a FSH surge, being a relative adverse action of LH surge gets made by the copresence of FSH within same cells or even the cytoplasm of the same area of the cell [24]. The selectiveness of their liberation is ensured not by GnRH but by other separate messengers like neuropeptide Y (NPY) protein [24], that yields a quite convincing reasoning for seeing some level of one with the other. Hence these findings point that the part of LH in ovulation is coordinating Meiosis getting resumed in, cumulus cell getting loosened in addition to follicular rupture.
Ovulation as Well Follicular Phase (FP)
Antral follicle generation Oocyte Regulation of Granulosa as well Follicle Escalation Prior to Entering in FP The pre antral follicle growth prior to its qualification into an antral follicle, is independent of any of the hormones implicated in reproduction as well as gets regulated via growth factors (GF) that get generated by Oocyte itself. Those growth factors regulate granulosa cells in addition to follicle escalation in size [25, 26]. The oocytes in the follicle that is encapsulated by a lot of layers of granulosa cells. The layer that is proximal most alias corona radiate generates tight junctions with the oolemma. At this stage each granulosa cell is meeting the requirements of the oocyte.
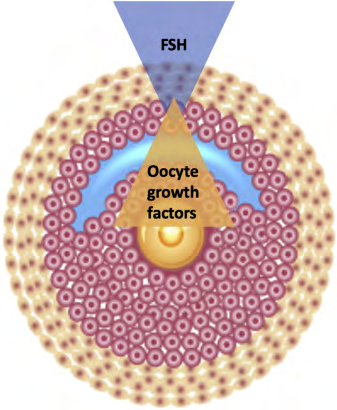
Prior to generation of the antral follicle, all granulosa cells have a commitment to generate FSH receptors besides differentiation into mural granulosa. Nevertheless, prolonged generation ofSMAD2/3 (as well as other GF that are growth differentiation factor9 (GDF9) in addition to bone morphogenetic protein 15(BMP15) by an oocyte avoids granulosa cells from acquisition of FSH receptors. GF’s move freely within the follicle as well as gets diluted with the maximum quantity proximal to the egg, as well as least at the follicular wall [27], generation of a gradient with the maximum amount proximal to the egg, as well as least at the follicular wall (Figure5). Once a cavity is generated within the follicle as well as its volume escalation occurs, oocytes- obtained GF’s get diluted till the maximum granulosa cells get relieved off the oocyte regulation as well as generate adequate FSH receptors. This ensures that the follicle gains responsiveness to FSH by end of the luteal phase of the prior cycle [28].
FSH Gains the role of regulator of the follicle once the oocyte gets recruitment into FP The generation of the oocytes at the time of FP will still get regulation by the oocytes-obtained GF’s. Nevertheless, escalation of the follicle size, that is secondary to the proliferation of the mural granulosa besides fluid getting collected, would be under regulation by FSH to start with in addition to later by FSH as well as LH, that gets generated from the anterior pituitary. Total recall of this double regulation aids us to visualize the events implicated for the egg getting hold of generational competency along with the event implicated for the final egg liberation from the follicle alias ovulation, get stimulated by various independent ,besides noncoordinated modes, that are responsible for the quality of the oocyte [29, 30].
Competitive association among FSH as well as GF’s The way already clarified the granulosa cells having commitment for acquisition of FSH receptors is their inherent characteristic as well as can’t get regulated externally. Nevertheless, the proper differentiation into cumulus along with mural granulosa cells represents a fluid event, since its decision occurs by competing gradients of the oocytes- obtained GF’s as well as FSH [27].
Finally these competing gradients are the once deciding that how much of these cells continue in the oocyte- cumulus complex in addition to how much of these cells get allotted to the follicular wall as well as generate estradiol (E2). Whatever proof that is existent suggests that if there are high FSH amounts then greater granulose would get recruitment into mural granulose cells, that keeps occasional granulosa cells to continue with an egg [24, 27]. It continues to be uncertain that how many cells are required to remain with the oocyte for it to receive adequate support in the form of nutrition, but probability exists that a lesser threshold is present. This brings about a robust, although a theoretical chance that escalated FSH amounts might result in the reduction of the quality of the oocyte. A lot of studies have documented the enhancement of quality of the oocyte with minimal ovarian stimulation validate this presumption [31]. Another feasible result of escalated granulosa recruitment into mural granulosa cells, despite enough amounts of cumulus cell are remaining for feeding the oocytes, is a follicle whose growth is out of proportion rapid thus it might go on to rupture prematurely .One of the significant outcomes of this competitive association is that oocyte no longer regulates the life cycle of the follicle, besides not possessing the capacity to get to term maturation by the time of the rupture of the follicle [30].
Ovulation
The initial preovulatory surge of P is LH independent Right from the initial days of ovulation research, the part of E2 in the form of an ovulation trigger was queried when a steep escalation was found as initially as 12h prior to the circulating P was estimated as early as 12hprior to any alterations in LH or E2 [8]. Not like E2 Preovulatory P continues to be relatively similar right through the FP, with its alterations are directly correlated with the impairment of the BM of the follicle, that is a signal for pending rupture of the follicle. Hence its escalation can work as an efficacious positive feedback that signals to the hypothalamus regarding the follicle being ready for evolution (Figure 6).
Buchholz, et al. [5], illustrated that the intramuscular injection of P stimulates an immediate escalation in Gonadotrophins akin to the escalation akin to seen in ovulation as well as midcycle surge. At a later stage these outcomes gotverified by Odell, as well as Swerdloff [6], besides by Leydendecker, et al. [7]. Liu as well as, Yen [32], demonstrated that P is necessary for the generation of normal dimensions of the LH surge, despite the surge on its own needs to get priming by E2. Batista, et al. [33], in 1992, documented from direct findings that progesterone inection deletes the block on ovulation secondary to RY486 administration in a dose –based manner, while RY486 administration avoids a premature LH surge [34]. In agreement with P acting as an ovulation trigger, P gene knockout mice do not ovulate, inspite of normally growing follicles. A lot of other proof that suggests the key part of P as the maximum upstream ovulation stimulator [4, 35, 36].
The importance of the preovulatory escalation of P amounts might be tough to agree with in view of it being very small in amount that is just 0.5ng/ml- in contrast to amounts of P that is believed to be significant in an Obstet Gynaecol practice. Nevertheless, on putting it proper perspective within the baseline of P at the time of baseline of P during the FP, this would depict a steep escalation of P12hr of 50-200%occurring 12h prior to peak of E2 or LH flare.
The acknowledged mode of the preovulatory LH independent surge of P Just prior to ovulation, the follicle becomes significantly Vascularalized that is followed by inflammation [37], that results in reduction of the hypoxic environment (Figure 7).This has a lot of significance since it opens the door for 2 feasible modes of P escalation.
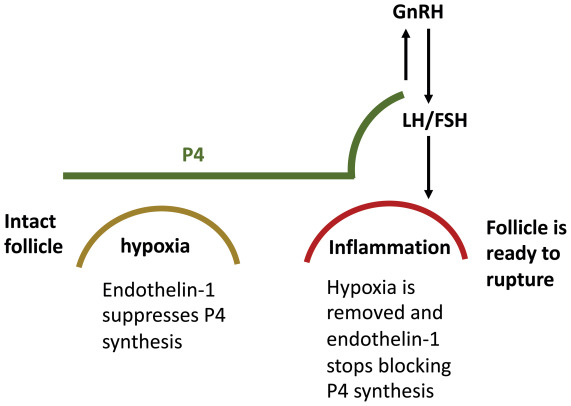
Figure 7: Courtesy ref no-2-As the growing follicle reaches its maximum size (determined by the speed of follicle growth, ovarian cortex elasticity, and other factors), it becomes inflamed, increasing the vascular supply and hence delivery of oxygen, thereby removing hypoxia and blocking endothelin 1, which removes the block for P4 synthesis, leading to a precipitous rise of P4 in the circulation. FSH = follicle-stimulating hormone; LH = luteinizing hormone; P4 = progesterone.
The initial one is that the alterations in the intrafollicular atmosphere liberate certain of the granulosa cells from the luteinization block. The second one presumed mode does not implicate luteinisation but an alteration in the constituents implicated in P generation. In particular it has been demonstrated that once hypoxic situations exist that Endothelin 1 represses P generation, awa on removal of hypoxia, escalation of P generation results [14]. The belief of Dorzstev, et al. [2], is that the possible source of P surge which binds to Hypothalamic progesterone receptor-A. This priming has been documented to be needed for the GnRH pulsation that ends in the flare of LH [38]. The regulation of P via hypoxia is not astonishing ,with the knowledge that hypoxia is implicated in the regulation of a lot of patho physiological pathways [39], whose innovation recently ended in nobel prize in medicine recently.
Noticeably the circulating P that antecedes ovulation does not display amounts having a direct proportion to the amount of P within the follicle [40]. This might point that the preovulatory LH surge is not purely due to escalated generation but further secondary to alterations in the permeability of the follicular wall. This might further give the reasoning of preovulatory surge of E2,that possesses little low molecular weight in contrast to P as well as might have certain benefits that aid it in crossing the follicle into the circulation.
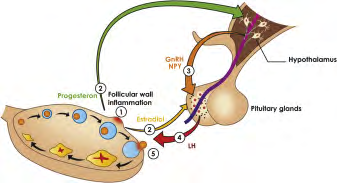
Figure 8: Courtesy ref no-2Proposed ovulation sequence. As the follicle begins to lose integrity (1) because of inflammation or LH-independent luteinization, P4 in circulation increases and E2 declines. Once P4 reaches the triggering threshold, it exerts positive feedback on GnRH signaling pathways and NPY (2). In its turn, GnRH binds to receptors in the pituitary, inducing the surge of gonadotropins, with the preferential release of LH (4) resulting from modulation by NPY (5). Gonadotropins cause the follicle to rupture, cumulus to disperse, mural granulosa cells to luteinize, and egg to ovulate. If E2 in circulation drops significantly before P4 induces LH flare, this releases LH (2), which accelerates luteinization of granulosa cells and boosts P4 to the GnRH triggering level. E2, estradiol; FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; LH = luteinizing hormone; NPY = neuropeptide Y; P4 = progesterone.
Whatever the precise mode of preovulatory escalation of P, once it reaches about 0.5ng/ml times over the baseline amounts, it signals to the Hypothalamus via the progesterone (P) receptor-A, regarding the imminent rupture of the follicle, resulting in the generation of the downstream cascade of processes. It is further feasible that a lot of modes detailed above work in synergism, resulting in redundancy (Figure8).
Rapid liberation of LH as well as FSH escalates fluid collection within the follicle, results in the breakdown of the gap junctions among the oocytes as well as cumulus cells, by which cumulus cells get scattered , as well as stimulation of Meiosis getting Resumed but for the condition that oocyte has gained this capacity [18]. For this the timing of Meiosis getting Resumed by the oocyte within a determined 30’ of the LH surge, resulting in the liberation of the oocyte with the rupture of the follicle 36-37h subsequently at the initiation of the optimal viable fertilization window. In case of controlled ovarian hyperstimulation cycles P might escalate much greater than 0.5ng/ml, without resulting in LH surge getting triggered since the GnRH gets disengaged from its receptors, resulting in P that is located upstream from the GnRH signalling pathway, gets avoided from stimulation of gonadotrophins surge at any area.
Clarification of the Complicated Paradoxical Action of P in Ovulation As far as history is concerned P has been considered as an ovulation blocking drug [7]. This capacity of P has been well acknowledged, besides getting corroborated by a lot of experience with different type of progestins in Oral contraceptive pills. On first view this can’t be reconciled with the probability of P resulting in stimulation of LH surge as well as stimulate ovulation, specifically since the circulating amounts of progestins that get utilized in OCP’s is markedly smaller in contrast to 0.5ng/ml amounts of P in the pre ovulatory surge.
The initial key step for the resolution of this conflict is to appreciate the that a gonadotrophin surge needs the collection of LH as well as FSH, in the repective granules in the prior FP. Without this collection, nothing is available for surge. Secondly the P like action of progestins is significantly greater in contrast to P. Hence in contrasting them with P, by the amounts existing in circulation misleads us. What is required is contrasting them rather by their activity. The determined activity of all progestins preparations in the circulation is greater than an equivalent of 0.5ng/ml of the pre ovulatory P.
Like a single pill in an OCP of dydrogesterone possesses P activity that is equivalent to that consisting of 200mg of injected P [41]. Hence, an oral consumption of 10mg of dydrogesterone would cause a determined circulating P
activity a minimum of a lot of times greater than its accepted gonadotrophins triggering amounts as well as greater than 1.7ng/ml threshold that as per Leydendecker, et al. [7], it doesn’t cause a positive feedback on LH liberation but hampers it.
This paradoxical situation as per Dozortsev D gets unravelled by posit that on continuous low P, like in FP, it lets gonadotrophins to collect as well as P receptors for getting sensitized. Thus once P starts to escalate, despite at relatively lesser P amounts, it has the capacity to stimulate GnRH trigger as well as results in LH/FSH liberation. In comparison when P action continues to be escalated continuously over and above gonadotrophins surge that of the triggering threshold, the way it is observed with OCP, at time of pregnancy, or the luteal phase, it results in desensitization of its own as well as by proxy that of GnRH receptors [42], ensuring that LH collection or its surge is not feasible, along with blockade of ovulation results.
Recalculation of P as well as E2 parts in trigger of gnrh surge This detailing of P in the form of physiological ovulation trigger can’t be finished without reconciling its presumed part with experiments where an LHsurge was stimulated by the injection of E2 in cases of castrated ladies, in whom total absence of any ovarian obtained P [7]. Dozotsev, et al. [2], think that a crucial point for resolution of this contradiction is acknowledging that E2 might not repress the generation of LH, but just its liberation into the blood [43], probably working via E2 membrane receptors, akin to those implicated in the rapid liberation of anterior pituitary hormone prolactin [44]. Hence one can presume that on E2 delivery to a woman where none of the ovaries are functional, her LH amounts in blood decreases secondary to its collection within the pituitary, while on the other hand, E2 getting cleared from the circulation would aid in the rapid liberation of LH in the blood stream. This gives a reasoning with satisfaction the outcomes of Leydendeckeretal [7], where following the injection of E2 benzoate in a woman who has been castrated ,an unambiguous intricate ,inverse association among reducing amounts of E2 as well as escalating LH in the with circulation. Further belief is that the LH peak observed on day 5 following injection in their experiment is secondary to the fall of E2 from 1000 to200pg/ml, at an amount that has the possibility that it can’t efficaciously block the liberation of LH into the circulation.
Significantly the LH surge generated by the clearing of E2 from the circulation does not avoid the generation of a following LH surge by P [7], that robustly implicates that utilization of various signaling pathways by them .This presumption gets further enforced by the finding that E2 does not have the capacity of induction of an LH surge following a P generated gonadotrophin surge [7]. Moreover, just the P generated gonadotrophin surge is correlated with a physiological LH: FSHratio [7].
Hence it is believed that in association P as well as E2 generate a mode that is safe from failure. To make sure that LH surge occurs, but just P influences a positive feedback on the GnRH signaling pathway. Thus it was posited that once a follicle loss of integrity gets started, the rapidity of P escalation in addition to fall of E2, besides the sensitivity of their respective receptors, would decide the precise sequence of the preovulatory processes, In case P first crosses the threshold amounts in circulation for triggering, a woman would demonstrate a single LH peak., that in turn boosts LH liberation, it generates. Incase E2 falls first below the threshold needed for blockade of LH liberation, it generates the first LH peak, that in turn boosts the P amounts by luteinizing granulosa cells as well as leads to a 2nd LH surge secondary to falling E2 would be anticipated to be smaller in contrast to that seen in the study by Leydendeckeretal [7], since the presuppression LH amounts in castrated women are practically a magnitude greater.
Exploration for Searching for what Might Serve as the Natural Ovulation Trigger
Ovulation trigger comprises a key step in the treatment of controlled ovarian stimulation in cases of patients subjected to in vitro fertilization, Intra Uterine Insemination, timed coitus, besides other kinds of fertility treatments. Besides Ovulation trigger being implicated for the latter stages of ovulation as well as rupture of follicle, it further shifts its granulose for generation of P, priming of the endometrium for later implantation. At present HCG is the only medicine receiving successful approval by the USFDA in the form of an ovulation trigger. Nevertheless, utilization of HCG is gradually facing reduction in view of the high chances of ovarian hyperstimulation Syndrome (OHSS), escalated utilization of GnRH analogue is being done in the form of an off label ovulation drug of choice in view of the lesser incidence of OHSS, possessing generally mostly good record of safety in addition to effectiveness, with relatively lesser cost.
Various kisspeptin derivatives are being evaluated (in phase II) for ovulation trigger. Nevertheless they are anticipated to be costly, once they do manage to enter the market [45]. The significant limitation of all the present available triggers, that is inclusive of kisspeptins, is that they are not capable of totally reproducing the natural pulsatile GnRH surge, that is thought to be the consequence of this event. this might reason out the deficiency in the luteal phase as well as the requirement of P addition. For compensating this deficit kisspeptin as an example requires repetitive injections. Further to simulate the pulsating quality of GnRH
liberation, a utilization of pump has been documented successfully [46]. None of them is clinically practical for utilization in a general infertile population.
In case P is actually the maximum upstream ovulation trigger, it might become a very cheap agent of choice, that would simulate natural ovulation.
Conclusions
A lot of experimental in addition to clinical proof suggests that a preovulatory luteinizing hormone independent escalation of P in the form of a trigger for the flare of ovulatory gonadotrophins. Nevertheless, the switch of the prototype has been slow, as one anticipates in medicine as well as a biology. Hopefully this summary stimulates lot of clinicians to have an open look at role of P in ovulation without any bias.
References
-
Christensen A, Bentley GE, Cabrera R, Ortega HH, Perfito N, et al.(2012) Hormonal regulation of female Reproduction. Hormon Metab Res 44(8): 587-591.
-
Dozortsev D, Diamond MP (2020) Luteinizing hormone independent rise of Progesterone as the physiological trigger of the ovulatory Gonadotrophins surge in the human. Fertil Steril 114(2): 191-199.
-
Hurst BS, Merriam KS, Elliot M, Matthews ML, Marsgburn PB, et al. (2015) A Sustained Elevated Estradiol is not the Trigger for the Preovulatory Luteinizing Hormone Surge. Women’s Health & Gynaecology 1: 1-3.
-
Messinis IE, Templeton A (1987) Effect of high dose exogenous oestrogen on midcycle Luteinizing hormone surge in Human spontaneous cycles. Clin Endocrinol(Oxf) 27(4): 453-459.
-
Zalanyi S (2001) Progesterone and ovulation. Eur J Obstet Gynaecol Reprod Biol 98(2): 152-159.
-
Buchholz R, Nocke L, Nocke W (1964) The influence of gestagens on the urinary excretion of pituitary gonadotropins, estrogen and pregnanediol in women in the post menopause and during the normal menstrual cycle. Int J Fertil 9: 231-251.
-
Odell WD, Swerdloff RS (1968) Progesterone–induced Luteinizing and follicle stimulating hormone surge in post menopausal women: a stimulatory ovulatory peak. Proc Natl Acad Sci USA 61(2): 529-536.
-
Leyendecker G, Wardlaw S, Nocke W (1972) Experimental studies on the Endocrine regulations during the periovulatory phase of the human menstrual cycle. The effects of exogenous 17- oestradiol and Progesterone on the release of pituitary Luteinizing and follicle stimulating hormone. Acta Endocrinol (Copenh) 71(1): 160-178.
-
Hoff JD, Quigley ME, Yen SSC (1983) Hormonal dynamics at midcycle: a reevaluation. J Clin Endocrinol Metab 57(4): 792-796.
-
Leavitt W, Chen TJ, Allen TC (1977) Regulation of Progesterone receptor formation by estrogen action. Ann NY Acad Sci 286: 210-225.
-
Stout EP, La Clair JJ, Snelli TW, Shearer TL, Kubanek J (2010) Conservation of Progesterone hormone function in invertebrate Reproduction. Proc Natl Acad Sci USA 107(26): 11859-11864.
-
Murphy BD (2000) Models of Luteinization. Biol Reprod 63(1): 2-11.
-
Wehrenberg U, Rune GM (2000) Spontaneous Luteinization of antral marmoset follicles in vitro. Mol Human Reprod 6(6): 504-509.
-
Takahashi T, Ohnishi J (1995) Molecular mechanism of follicle rupture during ovulation. Zoolog Sci 12(4): 359- 365.
-
Tedeschi C, HazumE, Kokia E, Ricciarelli E, Adashi EY, et al. (1992) Endothelin 1as a Luteinization inhibitors of rat granulosa cells Progesterone(P) accumulation via selective modulation of key steroidogenic steps affecting both P formation and degradation. Endocrinology 131(5): 2476-2478.
-
Hubbard GM, Erickson GF (1988) Luteinizing hormone- independent Luteinization and ovulation in the hypophysectomized rat: a possible role for the oocyte? Biol Reprod 39(1): 183-194.
-
Kubiack JZ (1989) Mouse oocytes gradually develop the capacity for activation during the metaphase II arrest. Dev Biol 136(2): 537-545.
-
Goudet G, Bezard J, Duchamp G, Gerard N, Palmer E (1997) Equine oocytes competence for nuclear and cytoplasmic maturation:effect of follicle size and Hormonal environment. Biol Reprod 57(2): 232-245.
-
Chian C, Bucket WM, Tulandi T, Tan SL (2000) Prospective randomized study of Human chorionic gonadotrophin priming before immature oocyte retrieval from unstimulated women with polycystic ovary syndrome. Human Reprod 15(1): 165-170.
-
Norris RP, Freudzon M, MehlmannLM, Cowan AE, Simon AM, et al. (2008) Luteinizing hormone causes MAP kinase dependent phosphorylation and closure of connexin 43 gap junctions in mouse ovarian follicles: one of 2 paths to meiotic resumption. Development 135(19): 3229-3238.
-
Kol S (2008) The vanishing follicle in women aged over forty: premature, mechanical, LH independent Luteinization may reflect oocyte-follicle low quality? Med Hypothesis 70(6): 1227-1228.
-
Dozortsev D, Nagy P, Abdelmassih S, Oliviera S, BrasilA, et al. (2004) The optimal time for Intra Cytoplasmic Sperm Injection in the Human is from 37 to 41 hours after administration of Human chorionic Gonadotrophin. Fertil Steril 82(6): 1492- 1496.
-
Yuzpee AA, Liu Z, Fluker MR (2000) Rescue Intra Cytoplasmic Sperm Injection (ICSI)-salvaging in vitro fertilization (IVF) cycles after total or near–total fertilization failure. Fertil Steril 73(6): 1115-1119.
-
Bauer-Dantoin AC, Tabesh B, Norgle JR, Levine JE (1993) RY486 administration blocks neuropeptide Y potentiation of Luteinizing hormone (LH) releasing hormone induced LH surges in proestrous rats. Endocrinology 133(6): 2418-2423.
-
Gilchrist RB, Lane M, Thompson JG (2008) Oocytes– secreted factors regulators of cumulus cell function and Oocyte quality. Human Reprod Update 14(2): 159-177.
-
Sanifins A, Rodriques P, Albertini DF (2018) GDF- 9 and BMP-15 direct the follicle symphony. J Assist Reprod Genet 35(10): 1741-1750.
-
Diaz FJ, Wigglesworth K, Epigg JJ (2007) Oocytes determine the cumulus cell lineage in mouse ovarian follicles. J Cell Sci 120(Pt 8): 1330-1340.
-
Channing CP, Schaerf FW, Anderson LD, Tsafiri A (1980) Ovarian follicular and luteal physiologys. Int Rev Physiol 22: 117-201.
-
Dozortsev D, Pellicer A, Diamond MP (2020) Progesterone is a physiological trigger of ovulatory gonadotrophins. Fertil Steril 113(5): 923-924.
-
Dozortsev D, Pellicer A, Diamond MP (2020) Term Oocyte maturation and term ovarian stimulation: impact on Oocyte competence. Fertil Steril 114(2): 221-222.
-
Zhang J, Chang J, Sone Y, Silber S (2010) Minimal ovarian stimulation (mini-IVF) for IVF utilizing vitrification and cryopreserved embryo transfer. Reprod Biomed Online 21(4): 485-495.
-
Liu JH, Yen SS (1983) Induction of midcycle Gonadotrophins surge by ovarian steroids in women: a critical evaluation. J Clin Endocrinol Metab 57(4): 797- 802.
-
Batista MC, Cartledge TP, Zellmer AW, NiemanLK, Merriam GR, et al. (1992) Evidence for a critical role of progesterone in the regulation of the midcycle Gonadotrophins surge and ovulation. J Clin Endocrinol Metab 74(3): 565-570.
-
Escudero BL, Boerringer PJ, Bennink HJ, Epifanio R, Horcajadas JA, et al. (2005) Mifepristone is an effective oral alternative to the prevention of premature Luteinizing hormone surges and /or premature luteinisation in women undergoing controlled ovarian hyper stimulation for in vitro fertilization. J Clin Endocrinol Metab 90(4): 2081-2088.
-
Lydon JP, DeMayo FJ, Funk CR, Mani SK, Hughes AR, et al. (1995) Mice lacking progesterone receptor exhibit pleiotropic reproductive abnormalities. Gene Dev 9(18): 2266-2278.
-
Coneely DM, Mulac-Jericevic B, Lydon JP, DeMayo FJ (2001) Reproductive function of the progesterone receptor iso forms: lessons from knockout mice. Mol Cell Endocrinol 179(1-2): 97-103.
-
Smith G, Roberts R, Hall C, Nuki G (1996) Reversible ovulatory failure associated with development of luteinizated unruptured follicles in women with inflammatory arthritis taking nonsteroidal anti- inflammatory drugs. Br J Rheumatol 35(5): 458-462.
-
White MM, Sheffer I, Teeter J, Apostolakis EM (2007) Hypothalamic progesterone receptor-A mediates Gonadotrophins surges, self priming and receptivity in estrogen –primed female mice .J Mol Endocrinol 38(1- 2): 35-50.
-
Semenza GL, Agani F, Feldser D, Iyer N, Kotch L, et al. (2005) Hypoxia,HIF-α,and the pathophysiology of com- mon Human diseases. Adv Exp Med Biol 475: 125-130.
-
Rothchild I (1965) Interrelations between progesterone and theovary, pituitary and the central nervous system in the control of ovulation and the regulation of progesterone secretion. Vitam Horm 23: 210-327.
-
King RJ, Whitehead MI (1986) Assessment of the potency of orally admintered progestins in women. Fertil Steril 46(6): 1062-1066.
-
McArdle CA, Forrest Owen W, William G, Davidson J, Poch A, et al. (1995) Desensitization of gonadotropin releasing hormone action in the gonadotrope—derived alpha T3-1cell line. Endocrinology 136(11): 4864-4871.
-
McNeilly AS, Crawford JL, Taragnat C, Nicol L, McNeilly JR (2003) The differential secretion of FSH and LH: regulation through genes, feedback and packaging. Reprod Suppl 61: 463-476.
-
Bulayeva NN, Wozniak AL, Lash LL, Watson CS (2005) Mechanisms of membrane estrogen receptor-alpha mediated rapid stimulation of Ca2+ levels and prolactin release in a pituitary cell line. Am J Physiol Endocrinol Metab 288(2): E388-397.
-
Abbara A, Clarke S, Islam R, Prague JK, Comninos AN, et al. (2017) A second dose of kisspeptin -54improves oocyte maturation in women at high risk of Ovarian hyperstimulation Syndrome: a phase2 randomized controlled trial. Human Reprod 32(9): 1915-1924.
-
Zheng J, Mao J, Xu H, Wang X, Huang R, et al. (2017) Pulsatile GnRH therapy may restore hypothalamus- pituitary-testis axis function in patients with congenital combined pituitary hormone deficiency: a prospective, self controlled trial. J Clin Endocrinol Metab 102(7): 2291-2300.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’