Pregnancy & COVID 19 Infection: Our Experience
Corona virus disease is also known as Covid -19. This pandemic has represented major impact on health system and societies world-wide. There is no particular high risk seen among mother and fetus. In addition to these aspects specifically to Covid -19 and gestation that should be known by specialist in order to correctly diagnose disease, classify severity; distinguish obstetric complications with specific signs of Covid -19 and for taking most appropriate management decision. The pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARSCoV2) has exposed vulnerable populations to global health crisis. Mother and fetuses are particularly susceptible to poor outcome. There are very limited data how SARSCoV2 behaves in pregnant women & their infants. We pearly reviewed 100 gravida women infected with covid-19 pneumonia. Out of which 72 symptomatic patients admitted to our hospital while 28 asymptomatic but Covid-19 positive patients’ care taken on OPD basis followed by home quarantine for 14 days. Aims & Objectives 1) To summarize the clinical features and oxygen requirement of COVID-19 in pregnancy and post-delivery. 2) Any intervention required to improve maternal and perinatal outcome. 3) Use of Remdesivir in hypoxic antenatal & postnatal patients with COVID - 19. Introduction The pandemic of severe acute respiratory syndrome coronavirus 2 (SARSCoV2) has exposed many populations in the world leads to global health crisis. Pregnant women and their fetuses are particularly susceptible to this infection with poor outcome. We pearly reviewed 100 gravida infected with COVID-19 pneumonia, out of which 72 symptomatic patients with high & moderate viral load admitted to our hospital while 28 asymptomatic patients with low viral load were taken care on OPD basis followed by home quarantine for 14 days. Materials & Methods This was a single-center; metaanalysis performed at Sunshine global hospital, Vadodara, Gujarat designated hospitals for pregnancy with COVID-19 in the epicenter of the SARS-CoV-2 outbreak and data compiled at Scientific Research Institute, Surendranagar, and Gujarat. We included antenatal & postnatal women with COVID-19 from inpatient & outpatient department.
Introduction
The novel coronavirus first time identified in December 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1, 2], has rapidly spread around the world. Second wave of COVID 19 more dangerous than first wave & affected more people as compared to first. Death rate seen more & effect of it on pregnancy got worsened [3, 4]. Treatments are rapidly evolving during the time of this deadly pandemic and several drugs remain under investigation as potential therapies for critically ill COVID-19 patients. Proposed antiviral treatment options include hydroxyl chloroquine, Remdesivir, and lopinavir/ritonavir, which are all safe in pregnancy.
Remdesivir is a nucleoside analog that inhibits RNA- dependent RNA polymerase. Remdesivir has previously demonstrated in vivo activity against both Ebola virus and Middle East respiratory syndrome (MERS-CoV) [5].
The novel coronavirus disease (COVID-19) is the most challenging health crisis that we are facing today. Against the backdrop of this pandemic, it becomes imperative to study, the effects of this infection on pregnancy and its outcome [6]. Hence, the present study was undertaken to evaluate the effects of COVID-19 infection in antenatal & postnatal period & its outcome.
LSCS was done for obstetric indications like non-progress of labour, foetal distress, etc. & non obstetric indications like high d-dimer, altered liver function tests [7]. Regarding the characteristics of the newborns, majority of neonates were born with a normal Apgar index [7–10] with average birth weight of (2.0–3.5 kg).
Pregnancy itself is high risk of adverse obstetrical and neonatal outcomes from many viral infections. A whole cluster of systemic effects, which propagate the risk of complications from respiratory infections, arise due to the altered physiological and immunological state that is a typical component of pregnancy. The cardiovascular and respiratory components of these changes, along with the development of an immunological adaptation that allows the maternal body to tolerate the antigenically diverse fetus; inflate the risk towards development of severe respiratory diseases.
Here, we analyzed the findings of 100 patients, there were complications of COVID-19 in some fetuses and it affected some pregnant women suggested that it does have adverse fetal and neonatal complications. A point that must be stressed upon is that almost all of the mothers that have been included in these studies were antenatal and postnatal. Lscs was planned after 34 weeks or completed weeks. Postnatally patient’s condition can be worsen on day 3-4 and were admitted for the same.
Materials & Methods
Study Design and Participants
This was a single-center; metaanalysis performed at Sunshine global hospital, Vadodara, Gujarat designated hospitals for pregnancy with COVID-19 in the epicenter of the SARS-CoV-2 outbreak and data compiled at Scientific Research Institute, Surendranagar, and Gujarat.
We included antenatal & postnatal patients with COVID-19 from inpatient & outpatient department.COVID-19 was diagnosed by RTPCR. All the COVID-19 patients had positive reverse transcription polymerase chain reaction (RT-PCR) results from respiratory samples.
Patient Identification and Data Collection
All patients consecutively admitted to The Sunshine global hospital, Vadodara, Gujarat with the diagnosis of COVID-19.
Data extracted from the patient records included age, the severity of COVID-19, symptoms, Hemodynamic status , laboratory tests, CT findings, treatments (antivirus regimens, antibiotics, corticosteroids ) and length of hospital stay, gestational age on admission, the outcome of pregnancy, and information on neonate were also recorded.
Laboratory and Radiological Presentations
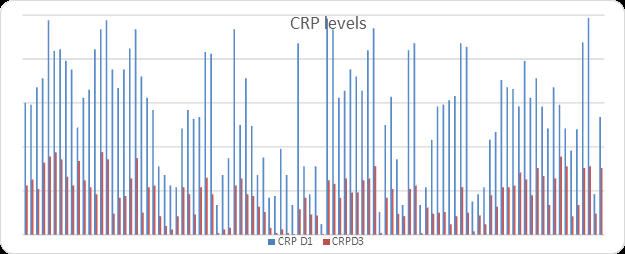
More leukocytosis (> 9.5 × 109/L) (10, 35.7% vs. 2, 3.7%; p < 0.001) and Elevated CRP levels (> 0.6 mg/dl) (17, 68% vs. 14, 25.9%; p = 0.001) were detected in pregnant women.
Baseline Hb level (117.5 g/L, IQR 106.75–129.00, vs. 126.00 g/L, IQR 121.25–135.50; p = 0.018) and albumin level (35.50 g/L, IQR 34.00–38.65 vs. 43.00 g/L, IQR 41.00–43.85; p < 0.001) were lower in pregnant patients.
Elevated alanine aminotransferase was observed in two (3.7%) non-pregnant women, with no reports in pregnant women (p = 0.80).
Patient Concerns
We report a clinically confirmed 100 cases of COVID-19 with pregnancy. Patients were tested positive for COVID-19 before delivery but became negative few days after delivery, out of which 41 patients delivered by LSCS at our hospital, 2 patients delivered vaginally, 5 patients got admitted after LSCS & 3 ANC in 1st trimester ,10 ANC patients got admitted in 2nd trimester & 11 in 3rd trimester& discharged, they delivered at their respective gynecologist. At 34 weeks of gestation with steroid coverage early LSCS was planned to decrease the materno fetal vertical transmission. We noted that after delivery recovery of mothers & babies was very high. 5 patients who presented very late but reports were very bad, they succumbed.
Outcome
ANC patients who admitted to our hospital in first & second trimester gave birth to a healthy baby after being cured from COVID-19 infection. 2 patients came in labour so delivered vaginally. 42 babies were negative on RTPCR, 1 still born baby was delivered in ICU, 1 baby was positive on RTPCR was kept under observation in NICU who turned negative after 7 days. 5 patients who presented very late but reports were very bad, they succumbed. Average number of hospital stay after LSCS is 5-10 days & after normal delivery 4 days. Pregnant patients with COVID 19 presented with mild to moderate symptoms with low viral load in early stage the recovery chances are high. Pregnant patients with COVID 19 with high viral load, chances of complications are high among them. Chances of vertical transmission cannot be neglected.
Lesson Subsections
The Findings of this case report are useful for understanding the possible clinical features of COVID-19 infection in pregnancy, duration of antibody & Passive immunity of the fetus, complications post natally due to COVID 19. Pregnant patients with COVID 19 presented with mild to moderate symptoms in early stage, the recovery chances are high.
Vertical Transmission of COVID-19
There has been a case where the possibility of vertical transmission has been elicited, where the neonate had an increased IgM level, which indicated involvement of innate immunity of the neonate. Also, reports suggest that 1 neonate, born to COVID-19 infected mothers, tested positive for SARS-CoV-2 postpartum.
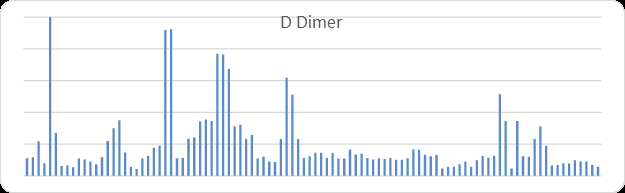
The principal for obstetric management of COVID-19 include rapid detection, isolation, and testing, profound preventive measures, regular monitoring of fetus as well as of uterine contractions, peculiar case-to-case delivery planning based on severity of symptoms, progression of disease, changes in blood reports like CRP, D Dimer, Coagulation Profile and Appropriate post-natal measures for preventing infection. Transmission during birth via contact with infectious vaginal secretions and after birth via respiratory secretions is a concern. Thus, a mother who has confirmed COVID-19 or is a person under investigation should be isolated from her baby until the mother is free from any possible transmission danger.
Result
The presentation of the Categorical variables was done in the form of number and percentage (%). The data normality was checked by using Kolmogorov -Smirnov test. The following statistical tests were applied for the results:
1. The association of the variables which were quantitative and not normally distributed in nature was analyzed using Mann-Whitney Test (for two groups) and Independent t-test was used for association of normally distributed data. 2. The association of the variables which were qualitative in nature was analyzed using Fisher’s exact test as at least one cell had an expected value of less than 5.
For statistical significance, p value of less than 0.05 was considered as significant.
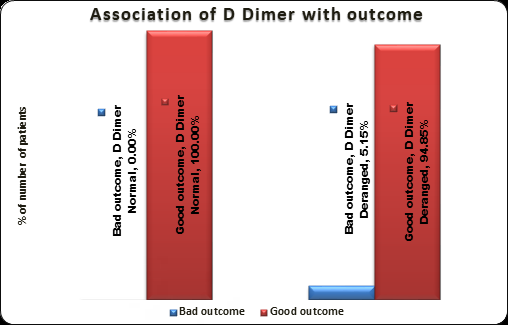
| D Dimer | Bad outcome(n=5) | Good outcome(n=95) | Total | P value |
|---|---|---|---|---|
| Normal | 0 | 3 | 3 | 1‡ |
| 0% | -100% | -100% | ||
| Deranged | 5 | 92 | 97 | |
| -5.15% | -94.85% | -100% | ||
| Median(25th-75th percentile) | 9189 (7685-9238) | 1162 (900-2041.5) | 1201 (957.25-2314) | 0.0003† |
Table 1: Association of D Dimer with outcome, Mann Whitney test, ‡ Fisher’s exact test
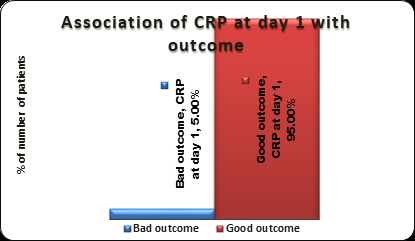
| CRP at day 1 | Bad outcome(n=5) | Good outcome(n=95) | Total | P value |
|---|---|---|---|---|
| Deranged | 5 | 95 | 100 | No p value |
| -5% | -95% | -100% | ||
| Mean ± SD | 113.8 ± 88.87 | 143.47 ± 62.12 | 141.99 ± 63.45 | 0.31* |
Table 2: Association of CRP at day 1 with outcome, *Independent t test
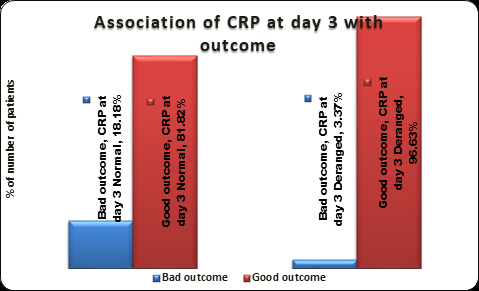
| CRP at day 3 | Bad outcome(n=5) | Good outcome(n=95) | Total | P value |
|---|---|---|---|---|
| Normal | 2 | 9 | 11 | 0.092‡ |
| -18.18% | -81.82% | -100% | ||
| Deranged | 3 | 86 | 89 | |
| -3.37% | -96.63% | -100% | ||
| Mean ± SD | 29.8 ± 36.69 | 44.77 ± 24.93 | 44.02 ± 25.6 | 0.204* |
Table 3: Association of CRP at day 3 with outcome, * Independent t test, ‡ Fisher’s exact test.
Discussion
Recent data demonstrated that pregnant women diagnosed with COVID-19 have an increased risk of ICU admission and mechanical ventilation as compared with non-pregnant women of childbearing age diagnosed with COVID-19.
OPD Basis patients asked to monitor SPO2 level every 4 hourly at home. Tab Azithromycin 500mg once a day for five days, Tab Zinc OD & Tab Vitamin C TDS given for 21 days. Follow up was done after 7 days in OPD, measurements checked were SPO2 & Pulse; SPO2 <95 percent or Tachycardia. Home quarantine for 14 days was advised.
We have categorized our patients in to mild, moderate & severe cases depending on RTPCR. Total 28 Mild cases with low viral load, 34 moderate cases with moderate viral load & 38 severe cases with high viral load were admitted. Out of severe cases 5 succumbed & in other patients with high viral load, use of early Remdesivir and early LSCS planned were advised for better outcome. We could successfully save severe cases of COVID19 with pregnancy.
Young patient had low platelet count in third trimester with very high D-Dimer & altered coagulation profile for which conservative management with injection leucovorin, injection vit.k given. On day 6 after admission patient had fetal distress for which emergency LSCS done after single donor platelets infusion, healthy baby delivered. Post- operative patient was stable, her platelet count drastically increased after delivery.
Young patient was admitted at full term with low oxygen saturation with very high D-Dimer & altered coagulation profile. After admission patient was on NRBM on which she maintained SPO2 -95%, injection remdesivir started, 4 FFP given. LSCS was done after giving 4 FFP infusions, a healthy baby was delivered. Post-operative, patient was stable.
Young patient was admitted on postoperative day 4 with complain of breathlessness for which patient kept on NRBM in ICU. On day 6 Patient had severe cough followed by burst abdomen with intestinal prolapse. Emergency resuturing was done. Stitch removal was done after 10 days of resuturing. Patient was stable.
Elderly patient was admitted at 36 weeks pregnancy with high D-Dimer & presented with SPO2-45% so patient was put on NRBM 15 liters, as patient’s condition worsened so emergency LSCS was done after giving 2 PCV & 4 FFP transfusions. On post-operative day 7 patients develop pancreatitis for which medical management was started. Patients’ condition detoriates continuously on day 9, patient went into cardiac arrest therefore patient was intubated in morning & in spite of this patient expired in evening.
Elderly patient with full term pregnancy was admitted at full term with low oxygen saturation with high D-Dimer & high CRP. LSCS was done, a healthy baby was delivered. On post-operative day 2 patients had very huge gaseous abdominal distension. Medical management was done. Post- operative patient was stable. Decisions regarding emergent delivery are individualized and require consideration of both maternal and fetal status.
Emergent cesarean delivery in ICUs is reserved for acute and severe maternal or fetal decompensation. We demonstrated that the pregnant women who are critically ill with COVID-19 can be managed in the ICU without the need for emergent delivery. Overall goal oxygen saturation was >95%, in order to ensure adequate fetal oxygenation; our most of the patient required non re breather , but never mechanical ventilation to maintain that oxygen saturation except 5 patients required mechanical ventilation.
Pregnancy is a hyper coagulable state with noted physiologic increases in D-Dimer. COVID-19 has been associated with elevations in D-Dimer and thrombus formation. Our patient had an elevated D-Dimer but no evidence of peripheral thrombi.
Given underlying hypercoagulability in pregnancy and known venous thromboembolic complications were associated with COVID-19, pregnant women who were positive for SARS-CoV-2 are placed on antepartum and postpartum venous thromboembolism prophylaxis.
Elevated CRP is also physiologic during pregnancy. Population-based studies have reported median CRP values in uncomplicated pregnancy ranging from 3 to 6 mg/L.CRP may not be useful in determining the severity of COVID-19 illness in pregnant patients.
Remdesivir is a prodrug, intracellularly metabolized into an adenosine triphosphate analog that inhibits viral RNA polymerase. After the emergence of SARS-CoV-2, in vitro testing demonstrated that remdesivir has activity against that virus; however, data on its use in pregnancy are limited. Manufacturer safety data indicate no reproductive developmental toxicity in animals at clinically relevant doses; embryonic toxicity was only noted when systemically toxic doses were administered to female animals before conception (Remdesivir Investigator’s Brochure, Gilead Sciences). Initial analysis of patients treated with compassionate use remdesivir demonstrated a low rate of adverse effects and possible mortality benefit.
The National Institutes of Health Adaptive COVID-19 Treatment Trial-1 (ACTT-1) study demonstrated that remdesivir was superior to placebo in decreasing time of recovery in hospitalized adults and may have mortality benefit. However, neither of these studies included pregnant women. Our patient will be included in a forthcoming analysis of patients receiving remdesivir via an updated compassionate use protocol. Before COVID-19, an Ebola treatment study included remdesivir as 1 of 4 arms. 6 of the 175 patients enrolled in that arm had a positive pregnancy test at the time of enrollment. No specific adverse outcomes in pregnant women were recorded in this arm of the study; however, the study report does not provide specific information regarding outcomes in these patients. In this case, our patient tolerated the medication well.
One of the noted side effects of remdesivir is transaminitis [9, 10]. Remdesivir may further complicate interpretation of elevated liver enzymes in a population where they could represent pre-eclampsia, viral effect, or physiologic elevation. Our patient did develop an increase in her transaminases while on remdesivir; whether this was due to COVID-19 or to remdesivir is not clear. Infected mother can transmit the virus via respiratory droplet not through breast feeding.
For statistical significance, p value of less than 0.05 was considered as significant. Elderly patients with high D Dimer, high CRP with comorbidities had bad outcome. Young Patients with high D Dimer, high CRP without comorbidities had good outcome. Steroids, higher antibiotics & multivitamins were given to patients [8].
Limitation
- This was a single-center; metaanalysis study
- We included all pregnant women with RT-PCR positive for COVID-19 irrespective of any previous illness present
- CRP may not be useful in determining the severity of COVID-19 illness in pregnant patients.
Conclusion
COVID-19 has been proven to be a deadlier infection. Pregnancy is a state of immuno suppression and thus pregnant women are more susceptible to complications of COVID-19, as compared to a non-pregnant woman. COVID-19 has adverse effects on both mother and neonate. Considering the reported fetal complications, it can be hypothesized that vertical transmission of COVID-19 is possible across the materno-fetal interface. Obstetric management of COVID-19 in positive pregnant women is a critical process, which is essential in procuring a good prognosis for the mother and preventing infection in the neonate. Early detection & proper management of patients were required for better outcome. Elderly Gravida with Comorbidities with high D-Dimer & CRP had bad outcome. There is more need of ICU stay, ventilator support, oxygen requirement & mortality rate. Young Gravida without Comorbidities with high D-Dimer & CRP had good outcome. Maternal & fetal outcome was good. Our patients highlight several important aspects of care. A number of studies have discussed COVID-19 in pregnant women.
References
-
Zaigham M, Andersson O (2020) Maternal and perinatal outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet Gynecol Scand 99(7): 823-829.
-
(2020) COVID-19 Map. Johns Hopkins Coronavirus Resource Center.
-
Breslin N, Bapatientiste C, Miller R, Fuchs K, Goffman D, et al. (2020) Coronavirus disease 2019 in pregnancy: early lessons. Am J Obstet Gynecol MFM 2(2): 100111.
-
Liu Y, Chen H, Tang K, Guo Y (2020) Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy. J Infect 2020.
-
Grein J, Ohmagari N, Shin D, Diaz G, Chen D, et al. (2020) Compassionate Use of Remdesivir for Patients with Severe COVID-19. N Engl J Med 382(24): 2327-2336.
-
Ellington S, Strid P, Tong VT, Woodworth K, Anderson K, et al. (2020) Characteristics of women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status- United States, January 22-June 7, 2020. MMWR Morb Mortal Wkly Rep 69(25): 769-775.
-
Murphy N, Broadhurst DI, Khashan AS, Kenny LC, Gilligan O, et al. (2015) Gestation-specific D-dimer reference ranges: a cross-sectional study. BJOG 122(3): 395-400.
-
RECOVERY Collaborative Group, Horby P, Lim WS, Fel- ton T, Jeffery K, et al. (2020) Dexamethasone in hospi- talized patients with COVID-19. N Engl J Med 384(8): 693-704.
-
Beigel JH, Tomashek KM, Dodd LE, Kalil AC, Finburg RW, et al. (2020) Remdesivir for the Treatment of COVID-19 - Preliminary Report. N Engl J Med 383: 1813-1826.
-
Mulangu S, Dodd LE, Davey RT Jr, Holman W, PALM Writing Group PALM Consortium Study Team, et al. (2019) A randomized, controlled trial of Ebola virus disease therapeutics Engl J Med 381(24): 2293-2303.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’