Retrospective Study on Fetomaternal Outcome in Gestational Diabetes Mellitus
Aims and Objectives: To evaluate the risk factors and feto-maternal outcome in mothers with Gestational diabetes mellitus. Materials and Methods: This is a retrospective analytical study conducted in the Department of Obstetrics and Gynaecology J. J. Hospital, Mumbai. Antenatal patients beyond 22 weeks of gestation with deranged sugars were included for the study. The diagnosis of GDM was made by Oral Glucose Tolerance test or by FBS, PPBS values. The diabetic mothers were started on diabetic diet and started on insulin or oral hypoglycaemic agents according to their requirement and monitored. The risk factors and effect on maternal and fetal outcome were thus compared among the groups. Results: Gestational diabetes mellitus has a higher incidence in mothers > 30 years (68%), with increased parity and increased pre-pregnancy BMI. It was observed that the babies born to GDM mothers have more incidence of being born preterm (32%) and increased in incidence of delivery by Caesarian Section (60%). The GDM babies have a higher mean birth weight (3.43 kg) and higher incidence of IUFD in mothers of GDM . Thus, the feto-maternal morbidity was significantly higher in patients with GDM. Conclusions: There was significant feto-maternal morbidity in patients with gestational diabetes mellitus. Hence, early detection by screening and timely intervention is necessary for a better feto-maternal outcome.
Introduction
Gestational Diabetes Mellitus (GDM) is the most common medical complication and metabolic disorder of pregnancy. It is a major and growing public health problem in most parts of the world, with a global prevalence of between 2% and
6%.). GDM is estimated to affect around 1 in 10 pregnant women worldwide.
Gestational diabetes mellitus (GDM) is defined as carbohydrate intolerance of variable severity with onset or first recognition during pregnancy (ACOG, 2017a). Normal pregnancy is a diabetogenic state characterised by hyperinsulinaemia and decreased sensitivity to insulin at cellular levels [1]. This progressive change in the maternal metabolism is due to the body’s effort to provide adequate nutrition for the growing foetus. As pregnancy progresses, the levels of a host of hormones such as of estrogen, progesterone, human placental lactogen, cortisol and prolactin increase and this leads to insulin resistance. The peak effect of these hormones is seen in the 26th to the 33rd week of gestation. Many of these hormones are insulin antagonists which causes insulin resistance in the mother and cause abnormal glucose tolerance in some women rendering them to develop gestational diabetes. Undiagnosed or inadequately treated GDM can lead to significant maternal and fetal complication. Women with GDM and their off springs are at increased risk of developing type 2 diabetes later in their life and recurrence of GDM is also seen in subsequent pregnancies. The incidence of DM in pregnancy is expected to increase to 20%. Approximately 8% of all pregnancies are complicated by GDM [2]. The prevalence may range from 1 to 14% of all pregnancies depending on the population studied and the diagnostic tests used5. Increasing levels of plasma glucose are associated with birth weight above the 90th percentile, primary caesarean deliveries, neonatal hypoglycaemia.
Risk factors for GDM includes history of macrosomia, strong family history of diabetes, obesity, undue weight gain, maternal age more than 25 years, persistent glycosuria, polycystic ovarian syndrome, significant past obstetrical history. Fetal complications likely to develop are macrosomia, IUD, malformation includes anencephaly, spina bifida, transposition of great vessels, VSD, renal agenesis, caudal regression syndrome, RDS, hypoglycemia, hypothermia, hyperbillirubinemia, hypocalcemia, hyperviscicity. Maternal complications includes a) Antepartum: abortion, preeclampsia, infection, polyhydroamnios, obesity macrosomic baby, b) Intrapartum: prolonged labour due to big baby, shoulder dystocia, PPH, increased incidence of caesarean section, c) Postpartum: Puerperal sepsis, increased maternal morbidity, diabetic retinopathy, diabetic nephropathy, diabetic ketoacidosis.
Improved outcome therefore depends on early diagnosis and good glycemic control [3].
Methods
A retrospective study was conducted at an urban tertiary care center (J. J. Hospital, Mumbai). During the period from October 2020 to July 2021, 50 cases of Diabetes in pregnancy who fulfilled the criteria were studied for feto-maternal outcome as compared to a control group of 50 non-diabetic patients [4]. Their detailed data was obtained and their age, obstetric history, gestational age, past history of DM, mode of delivery, outcome of pregnancy, fetal weight, maternal and fetal complications and requirement of oral hypoglycaemic agents or Insulin were taken into consideration for the study. A retrospective analysis was made based on these parameters.
Inclusion Criteria
Pregnant women > 22 weeks of gestation with blood sugar levels 140-200mg/dl after 2 hours of 75 g oral glucose (DIPSI).
Exclusion Criteria
Patients with chronic diabetes mellitus (before 22 weeks of gestation)
Results
- A positive correlation was seen in GDM mothers to increasing age, increasing BMI and positive family history
- GDM is associated with increased incidence of maternal, fetal and neonatal complications such as PIH, Preterm birth, IUFD, Macrosomia, hypoglycemia, hyperbilirubinemia, RDS.
- GDM increases the need for Caesarian Sections [5].
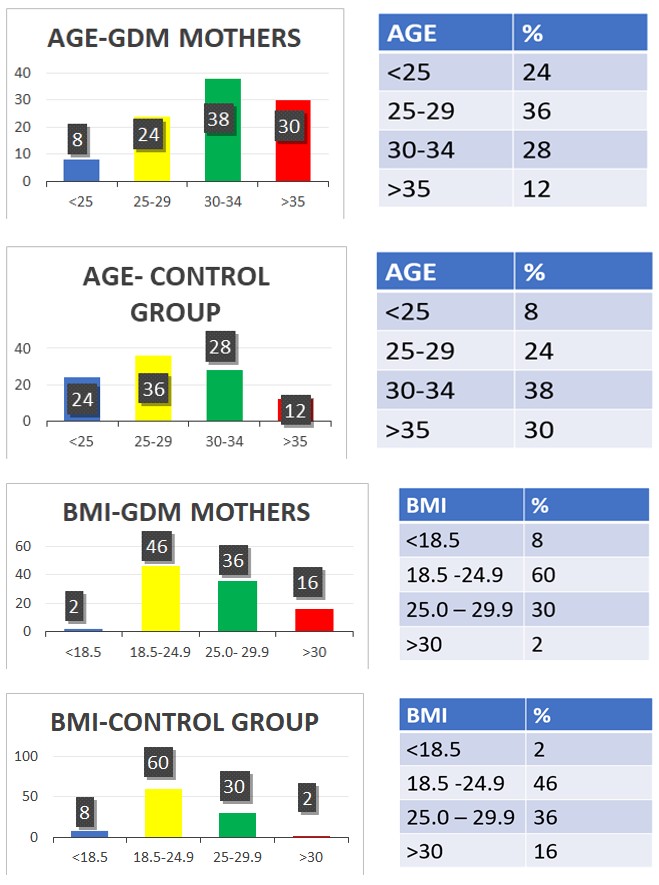
- 68% of GDM mothers are aged more than 30 years as compared to 40% in non-DM mothers
- Odds of a GDM mother being >30 years is 3.2 times that of a non-diabetic mother [6].
- Prevalence of obesity in GDM mothers is 16% and only 2% in non-GDM mothers
- Odds of a DM mother being obese is 9.33 times that of non-DM mothers
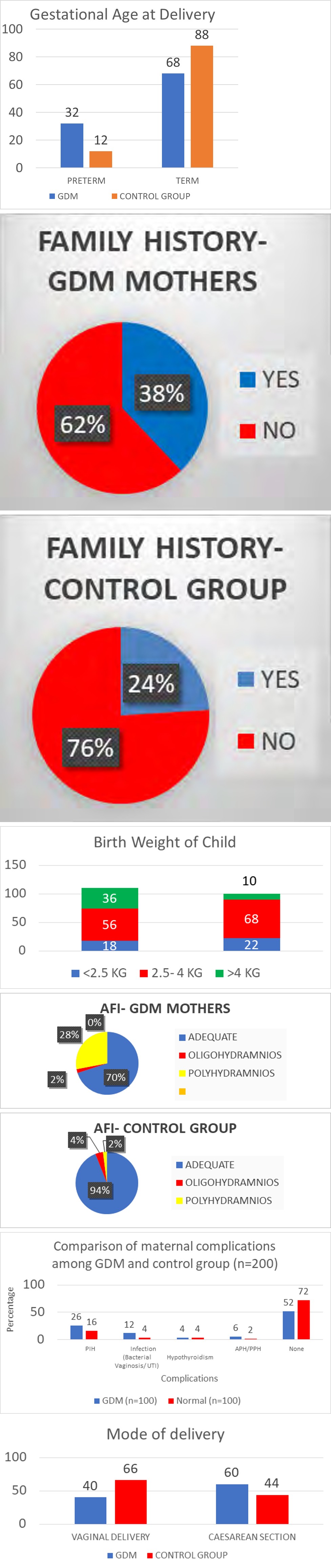
• 38% of GDM mothers had family history of DM as compared to only 24% of Control group
• Polyhydramnios was seen in 28% of GDM mothers, in comparison to 2% of mothers in Control group.
• 60% of GDM mothers delivered by Caesarean Section, compared to 44% in the control group.
• 32% of GDM mothers delivered preterm babies (< 37 completed weeks).
• In this study, 36% of babies born to GDM weighed > 4 kg.
• Maternal complications such as PIH, Bacterial vaginosis, UTI, Antepartum and Postpartum hemorrhage were seen associated with mothers with GDM.
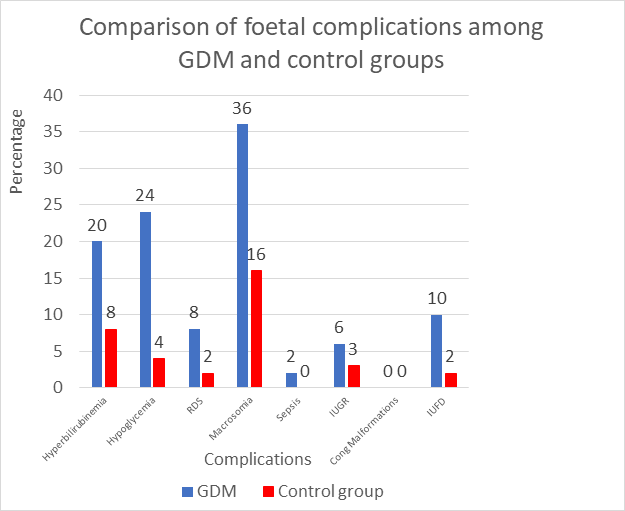
• GDM was also seen to be associated with fetal complications such as fetal hyperbilirubinemia, fetal hypoglycemia, Respiratory Distress Syndrome, Macrosomia, and IUFD.
Discussion
In the present study, GDM was seen to be associated with mothers of elder age group, overweight and obesity, and those with family history of GDM. Polyhydramnios, which is known to be the most common complication of GDM, was seen in 28% of GDM mothers in comparison to only 2% in the control group [7]. Mothers with GDM have been seen to have more chances of undergoing Caesarean section, owing to increased birth weight, fetal distress, obstructed labour and severity of maternal and fetal condition. Incidence of preterm birth was observed more in mothers with GDM due to maternal vaginal infections, PPROM, fetal distress or early intervention for termination of pregnancy to avoid further complications in the severity of maternal and fetal conditions. Babies born to GDM mothers were found to be having an increased birth weight as compared to the control group.
Conclusion
The study concluded that pregnancy with diabetes was more common in older age group. Rate of caesarean section was common in pregnancy with diabetes. IUFD, preterm delivery, admission in NICU were common in diabetic patients. Birth weight >3.5kg were also common in diabetic patients. Prepregnancy counseling in patients with overt diabetes with good glycemic control can reduce complications. Educating patients about regular antenatal care and proper monitoring of blood glucose level are important measures to reduce maternal and fetal complications. Universal screening and management by team approach of obstetrician, diabetologist, anaesthetist, physician, and neonatologist can reduce fetal- neonatal and maternal morbidity and mortality associated with pregnancy with diabetes.
References
-
Cunningham FG, Kenneth JL, Steven LB, Jodi SD, Barbara L, et al. (2018) Williams Obstetrics, 25e. McGraw Hill.
-
Shingala KD, Sapana RS, Rupa CV, Purvi MP (2019) Fetomaternal outcome in patients with diabetes mellitus in pregnancy. International Journal of Reproduction, contraception, Obstetrics and Gynecology 8(7): 2701- 2704.
-
Fareed P, Siraj F, Lone K (2017) Fetomaternal outcome in women with gestational diabetes mellitus. International Journal of Research in Medical Sciences 5(9): 4151-4154.
-
Groof Z, Garashi G, Husain H, Owayed S, AlBader S, et al. (2019) Prevalence, Risk Factors, and Fetomaternal Outcomes of Gestational Diabetes Mellitus in Kuwait: A Cross-Sectional Study. J Diabetes Res, pp: 7.
-
Odar E, Wandabwa J, Kiondo P (2004) Maternal and fetal outcome of gestational diabetes mellitus in Mulago Hospital, Uganda. Afr Health Sci 4(1): 9-14.
-
Seshiah V, Das AK, Balaji V, Joshi SR, Parikh MN, et al. (2006) Diabetes in pregnancy study group. Gestational diabetes mellitus-guidelines. J Assoc Physicians Ind 54: 622-628.
-
Hiralal K (2014) Dutta DC Text Book of Obstetrics. 9th (Edn.), JAYPEE- The Health Science Publisher, pp: 686.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’