What is the Impact of Mosaicism for Embryo Selection: Experience Obtained Subsequent to the 1000 Mosaic Embryo Transfer- A Mini Review
Chromosomal mosaicism, implying the co-occurrence of cells having possession of separate Chromosomal amount, has got illustrated in human embryos for the past3 decades. The initial versions that were generated with regards to preimplantation genetic testing for aneuploidy (PGT-A) did not estimate mosaicism, in view of classically just the evaluation of a single cell was carried out or the approach did not possess the capacity of precise Identification. Despite, a straight forward diagnosis was yielded (an embryo got the label of normal or abnormal, thus just evading the topic, with now as hindsight might have been resulting in umpteen mistakes in the diagnosis that caused negative clinical outcomes .The modern PGT-A estimates a multicellular trophectoderm biopsy sample with the methodology possessing the capacity of recognition of intermediate copy number signals for the chromosomes or the subchromosomal areas. Thus we get faced with the topic of mosaicism in addition to thehurdles with regards to the management of the embryos that generate such outcomes in the clinical scenario. Here we conducted a systematic mini review utilizing search engine pubmed, google scholar; web of science; embase; Cochrane review library utilizing the MeSH terms for this mini review like PGT-A; aneuploidy; euploidy; mosaicism; implantation; ongoing pregnancy; spontaneous abortions; 100-1000mosaic embryo transfer study/studies; self-correction of mosaic embryos; multipolar mitosis; tripolar mitosis; low mosaic; high mosaic; final outcomes from 1990 to 2021 till date. We found a total of 500 articles out of which we selected 38 articles for this mini review. No meta-analysis was done. Here we have tried to detail the that demonstrated that mosaicism besides in general, however particular characteristics picked up with PGT-A are correlated with differing clinical outcomes. Thus requirements are there regarding mosaicism to get considered in the context of greater informed in addition to embryo selection in the clinical scenario.
Introduction
In the 1990’s investigators, with the utilization of giving a label to the chromosomes with the aid of fluorescence in situ hybridization (FISH) probes on the total humans preimplantation embryos documented findings that invoked interest with regards to rarely single embryos possessed a cell mixture with varying chromosomal counts [1]. Prior to that mosaicism had been revealed with regards to other aspect of animal in addition to humans physiology [2], however in the first instance, visually it was illustrated that humans embryos might be in possession of a combination of chromosomally normal along with cells with aberrations.
In the last 3 decades these findings were validated. These were inclusive of FISH studies that implicated full embryos [3, 4, 5, 6]; further involved contrasting of specimens that were obtained by serial biopsies from separate embryos, irrespective of DNA quantification, technique where utilization of (FISH, quantitative polymerase chain reaction (PCR), Single nucleotidepolymorphisms (SNP) array (array comparative Genomic hybridization], or next generation sequencing (NGS) [7, 8], in addition to evaluation of single cell RNA sequencing results that documented chromosome wide changes in gene expression [9, 10]. The mistakes with regards to post mitotic segregation that results in mosaicism have further been seen live just the way they takes place in murine in addition to bovine embryos with the utilization of fluorescent reporters [11]. Thus the presence of mosaicism in the form of a biological event in embryos gets corroborated with adequate exhaustive proof.
Hence it is not astonishing that existent preimplantation genetic testing for aneuploidy (PGT-A) in routine where assessment of the collective chromosomal quantity of the multi cellular biopsy specimens of the trophectoderm (TE), should rarely catch cases of mosaicism. Platforms considered to be the state of the –art with regards to PGT-A yields high resolution in addition to wide dynamic range that promotes the estimation of mosaicism as presented by intermediate copy numbers (ICNs) of chromosomes or sub chromosomal areas. These outcomes agree with mosaicism along with blastocysts that have been sampled are known as, ‘’mosaic’’ with total insight that the biopsy specimen is just a sample of the embryo (i.e. a5-10 cell ‘’window’’ with regards to the chromosomal status of about 200 cell blastocys). Thus the query remains –what is the approach as to the management of ‘’mosaic’’ embryos in the clinical scenario?
Methods
Here we conducted a systematic review utilizing search engine pubmed, google scholar; web of science; embase; Cochrane review library utilizing the MeSH terms for this mini review like PGT-A; aneuploidy; euploidy; mosaicism; implantation; ongoing pregnancy; spontaneous abortions; 100-1000 mosaic embryo transfer study/studies; self- correction of mosaic embryos; multipolar mitosis; tripolar mitosis; low mosaic; high mosaic; final outcomes from 1990 to 2021 till date.
Results
We found a total of 500 articles out of which we selected 38 articles for this mini review. No meta-analysis was done.
Transfer of Embryo that Belong to the Mosaic’ Type
The initially description of embryo transfer (ET) being conducted with the possession of knowledge earlier with regards to the mosaic diagnosis with the utilization of modern PGT-A was documented in 2015 [12].
Greco, et al. [12], detailed the transfer of embryo that had been labelled as mosaic for 18patients, who did not possess the euploid embryos for transfer that ultimately caused 6 babies that appeared healthy apparently.
Subsequently various centres in addition to clinics have revealed their own encounter regard to the transfer of mosaic embryos [13, 14, 15]. The total studies, reached an agreement that healthy pregnancy in addition to live births were feasible, however they caused lesser clinical success rates in contrast to euploidembryos [12, 13, 14, 15, 16]. In particular, mosaic embryos possessed lesser rates of implantation, ongoing pregnancy in addition to birth as well as escalation of, the incidence, of spontaneous abortions, which was presented by a meta-analysis of these documentations [17].
Nevertheless, a conflict was there with regards to if particular characteristics, of mosaicism as estimated by PGT-A were correlated with different clinical results. This is a crucial point since such correlations possessed the capacity of potentially passing information guidelines with regard to embryos prioritization in the center. Two characteristics, of mosaicism can be obtained from the PGT-A outcomes is the mosaic level or the deciphered percentage of aneuploid cells that is existent in the sample with regards to disomy 2 cases , PGT-A generates an outcome that pointed to a chromosomal copy number of2,for trisomy a copy number of3 etc. Like a chromosomal copy number of 2.4 pointed to 40% of cells being trisomic, in addition to 60% are disomic, with the sample labeled to possess, a mosaic trisomy at the 40% level. On the other hand a chromosomal copy number of 1.3 pointed to 70% of the cells are monosomic, with 30% being disomic, with the sample labeled to possess a mosaic monosomy at the 70% level. Usually such outcomes do not get documented in so much quantification detailing, with grouping of mosaic level as ‘’high’’ as well as ‘’low’’ categories with the utilization of a cutoff like 50%. From the biological angle, these mosaic level get impacted by the timing in addition to mode of chromosomal segregation. In particular, the mitotic mistakes ,that takes place at the time of early post zygotic divisions would progress to a greater percentage of daughter cells, although it is posited that following events of natural selection might change this ratio [18].
The other characteristic of mosaicism can get estimated from the PGT-A outcomes is the ‘’kind’’. This represents the type of aneuploidy: segmental, 1 chromosome (monosomy or trisomy), 2 chromosomes or complicated aneuploidies that influence 3 or greater chromosomes. Despite mistakes like mitotic nondisjunction in addition to anaphase lag might classically influence 1 or 2 chromosomes greater disastrous modes, like multipolar mitosis (alias aberrations in mitotic figures with chromosomal material pulled to greater than 2 poles as well as more than 1 centrosome with greater than 3 daughter cells instead of 2 with tripolar spindle in case of tripolar mitosis originating aid to the complicated as well as haywire types of mosaicism [19].
Despite, certain studies have documented that there exists a correlation with the level with regards to mosaicism along with the result of mosaic ETs, the other groups have arrived at a contradictory conclusion. Furthermore, no agreement with regards to any kind of mosaicism possess better clinical results. These type of variable results might be secondary to utilization of various PGT-A platforms, different definitions of mosaic outcomes, or smaller sample sizes across the separate studies in separate single studies.
The Study Involving 1000 Mosaic Embryos
For getting an answer in the context of mosaicism a collaboration of certain clinics in addition to PGT-A centres conducted a collective study with these objectives i) Attaining a big size of sample for the escalation of the power in the context of evaluation, ii) Utilization of a standardized PGT-A platform that was dependent on NGS, the state of the-art for evaluation of mosaicism [20]. iii) Utilization of a common definition of mosaic outcomes dependent on earlier posited thresholds amounts [20-80%) [13], corraborate the estimation of mosaicism in each laboratory as well as iv) Regulation for the parameters, which might become the confounding factors for the retrospective contrasting amongst the mosaic along with euploid group .The outcomes of this study where evaluation of transfers of 1000 mosaic embryos had been published in the recent past [16] in contrast to the clinical results with regards to a control group that comprised of 5000 euploid embryos,the mosaic group possessed a significantly lesser implantation rates that was correlated with a significantly lesser ongoing pregnancy (when evaluation, was conducted, or birth, in addition to an escalation of rates of spontaneous abortions (figure 1) [rev in ref 21,22]. Each variation was highlighted greater when just embryos that had mosaicism which influenced whole chromosomes had been taken into account that implies that segmental mosaic embryos got excluded (figure 1). These parts of the study were in agreement with earlier outcomes that emphasized on the worst results of the embryos which had received the classification of mosaicism. In case of maximum studies that were existent, there was insight with regards to the outcomes of PGT-A prior to transfer, that affected in deciding if these mosaic embryos transfer should be undertaken in contrast to the other embryos that might be existent which adds to a bias in the context of selection (like if transfer of mosaic embryos undertaken without proportion as a last attempt. For amelioration of this bias, a sub group evaluation in the 1000 mosaic embryos study concentrated on utilization of mosaic embryos at the 1st transfer, that still possessed lesser success rates as compared to the euploid group. With regards to an extra 164 of these 1000 mosaic embryos no information existed at the time of conducting an embryo transfer. Thus what was labelled as the non-selection aspect of study evaluation, the clinical results in that group also were worst significantly in contrast to euploid group that acted as controls (Figure 1).
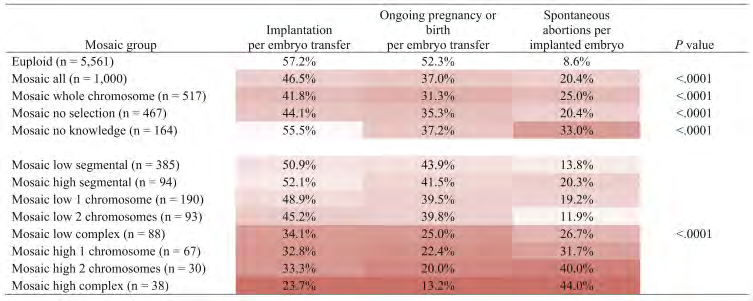
Figure: 1 Mosaic- Let Data Talk [21].
The combination of the transfer mosaic embryos group results got further broken down as per the mosaic characteristics, keeping in mind the different permutations of mosaic level as well as kind .This stratification demonstrated that variety of mosaic embryos groups possessed various clinical results as compared to the euploid control group. On further sorting the sub groups with regards to non- embryo culture. Mosaics labeled as low level ones (<50% aneuploid cells) had a correlation with greater advantageous results in contrast to those labeled as high level ones (≥50% aneuploid cells), in addition to amongst these groups, the kind of mosaicism was clarified, hence from those that were maximum advantageous to the ones that were least namely - 1 chromosom>2 chromosomes>complicated (figure1). The worst success rates were correlated with high level complicated mosaics, however rarely these caused a live births as well. In toto these observations might act as a template for hierarchization in the center.
Since selection of embryo further implicates, morphology to be taken into account, the results got further influenced via the assimilation of the PGT-A sub goup in addition to embryo stage as well as group . Repeatedly future trends became clarified within different groups. The resultant matrix of these results might act prospectively in the center scenario with regards to ranking of embryos [16]. An online tool that can get accessed with ease for the clinician with regards to giving input of the properties of 2 or greater embryos besides estimation of their apparent chances of yielding clinical success dependent on the practice gained from this 1000 mosaic embryos study.
The Resultant Pregnancies along with Live Births from the Mosaic Embryos Transfer
The reluctance of transfer of embryos where mosaicism gets picked up is justifiable. It is known that chromosomal mosaicism is one of the reasons that accounts for human problems in addition to placental mosaicism that might result in placental impairment [2].
Out of the 247 births from these 1000 mosaic embryos study, neither of the baby possessed any kind of congenital abnormalities [16]. A greater full outcome that were obtained with regards to the 162 new borns, every one of which was matched with a birth from the euploid embryo transfer group. On an average the weight of the babies in addition to gestation age were equivalent amongst the 2 groups, with no manifested symptomatology that was correlated with chromosomal as well as congenital abnormalities got documented from the new borns from the mosaic embryos cohort [23]. Subsequent mosaic embryo transfers that were conducted in >100 amniocentesis outcomes along with >
200prenatal evaluations that was over each platform that was inclusive of amniocentesis, chorionic villus sampling in addition to noninvasive prenatal evaluations, 5 cases of congenital aberrations were reported [16, 24]. Each of these 5 were from the amniocentesis group, that isolated segmental imbalances that were lesser in contrast to the resolution that was achieved by present PGT-A, NGT platforms that were not associated with mosaicism which got picked up by PGT-A. Hence in this particular sample) group, the mosaicism that was detected at the blastocyst stage did not persist right through pregnancy.
The query arises how does one anticipate the disappearance of the blastocyst stage mosaicism? The outcomes from the mosaic embryo transfers yield an indirect clinical proof with regards to auto correction with the utilization of a mode of clonal depletion [25], in which aneuploid cells of mosaic embryos get over competed by euploid cells via differential proliferation in addition to/or directed apoptosis. Actually an association that is well proven amongst aneuploidy along with ameliorated cell proliferation in humans as well as other organisms [26] (with a noticeable deviation of cancer in which case aneuploidy takes place as a common occurrence, however, escalation of proliferation is basically secondary to mutations in oncogenes in addition to tumor suppressor genes). Hence, mosaic embryos might generate into healthy babies if the aneuploid cells dilution occurs enough throughout pregnancy , ensuring that by the time of delivery reaches (or much prior to that ,as judged by the prenatal evaluation outcomes) no decipherable trace . With regards to more corraboration of this evidence, a study by Esteki etal. [27], where the genomic landscape with regards to fetal and placental tissues at postpartum in case of both In vitro fertilization (IVF) in addition to those that were natural conceptions illustrated that mosaicism conservation was not observed in the later aspects of prenatal generation in addition to occurence of de novo numerical abnormalities or large structural DNA imbalances was at akin rates of prenatal generation in IVF as well as natural conceptions [27]. Escalation of experimental proof with regards to auto correction of embryonic mosaicism. Single cell RNA sequencing in case of mosaic embryos pointed that aneuploid cells resulted in down regulation of proliferation genes, besides a constant reduction amongst cleavage stage along with blastocyst stage of generation [9, 10]. Extended In vitro culture assays, as demonstrated by Popovic etal. [28], that mosaic blastocysts possess a tendency to get transformed towards totally euploid which is equal to the early stages post implantation [29]. Human gastruloids (implying models of gastrulation stage embryos which get obtained from embryonic stem cells) where mosaicism got chemically induced possess a susceptibility towards deletion of the aneuploid compartment as illustrated by Yang etal. [10], with passage of time secondary to apoptosis [10]. Mouse chimeric blastocysts that are made up of euploid in addition to aneuploid cells commonly get transformed to totally euploid if initially the aneuploid: euploid ratio is equal/low, however, they possess a susceptibility towards death if this ratio is high [29]. This particular mouse model of mosaicism illustrated ameliorated proliferation in addition to preference of apoptosis of aneuploid cells, that gets compensated by an escalation of proliferation of euploid cells [29]. Actually experiments where utilization of Immunofluorescence was done by Victor etal. [14] in a prospective study demonstrated significant separate patterns of mitosis along with cell demise amongst human embryos where classification was euploid or aneuploid in a study involving 100 mosaic embryo transfer [14].
Hence it becomes significant that a differentiation needs to be there amongst mosaicism at the blastocyst stage along with the (classically normal) karyotype later in pregnancy. Just one documentation is existent till date with regards to amniocentesis that pointed to the mosaicism that got picked up via PGT-A [30]. This pregnancy caused a live birth, besides the phenotypically healthy baby illustrating mosaicism in a blood sample (however not in a buccal swab). The estimated amount of mosaicism underwent a reduction with the passage of time from 35%with PGT-A to 2% with amniocentesis as well as 2% in one tissue at birth. This case warrants for continuous escalation of, watching pregnancies from mosaic embryo transfers by strict surveillance of fetal growth in addition to prenatal evaluation. With time along with extra results will let us know if this Single case represents an outlier, or if continuation of mosaicism right through pregnancy is commoner in contrast to the bulk of results pointed here.
Further Definition besides Expansion of Embryo Categories in PGT-A
With regards to the results, the initial binary classification system of embryos in the form of ‘’normal’’ as well as ‘’abnormal’’ appears redundant .In case this gets continued, embryos where classification requirements, is as mosaic would get classified in ‘’normal’’ or “abnormal” group that either gives overvaluation or undervaluation of their generational capacity, respectively. Inability to differentiate amongst euploid along with aneuploid might influence their clinical success rates, having possession of their worst results. On the other hand if we group the mosaic category with the aneuploid one would imply discarding of the viable embryos , as well as if there is non-availability of euploid embryos that pointed that patients have a prevention of a capacity of a normal pregnancy. Further stratification of mosaic embryo into sub groups as per the mosaicism level in addition to kind ,thus having a choice. The embryo that , possesses maximum chances of clinical success might get priority.
It is further significant to differentiate amongst auto correction in case of a mosaic setting in addition to cell intrinsic forms of auto correction (the so called labeled rescue from aneuploidy). In this latter instance aneuploidies would get rectifiedor auto corrected amongst cells, that would aid a totally aneuploid embryo (which arose from a meiotic mistake) to rectify itself, at least partly. This might result in the thought of embryo transfer which gave a result that pointed to totally aneuploidy, hoping that auto correction would occur. Nevertheless, the proof for this mode in human IVF is minimal. Intracellular rectification by endoreplication (with regards to monosomy) or rescue from trisomy [31], mostly resulted in uniparental disomy, which is occasional in case of IVF-developed blastocysts [32]. If there has not been any rectification of aneuploidy by that stage, it is not feasible that the embryo would cause a healthy pregnancy. Actually embryo transfers of the embryos on classification assigned to be aneuploid uniformly (non mosaic) with PGT-A possess practically no expectation of causing a healthy pregnancy, leave a normal pregnancy alone [33]. Hence in no condition embryo carrying a mosaic outcome be combined with those with an aneuploid outcome into a single abnormal group. Separate PGT-A Methods –Akin Outcomes It becomes key that evaluation of the precision of every PGT-A platform for it to be known as mosaicism. Particularly the corroboration of platform needs to be conducted in a method that specific properties of mosaicism (level in addition to kind) can get precisely evaluated. For achievement of this experiments where cells/DNA extraction of euploid as well as aneuploid control sample are mixed in proportions that are known earlier that is subsequently followed by a total PGT-A protocol with the outcomes that are contrasted with the anticipation the reaction is required to possess 5-10 cells or DNA quantity that is equivalent to that cell range, thus simulation of a clinical trophectoderm (TE), biopsy sample . With the utilization of cell lines with separate aneuploidies (whole chromosome as well as segmental aberrations) in addition to preparation of mixture ratios (1:9,2:8,3:7 etc) aids for detailed evaluation of estimation precision. Various groups have proved with success that NGS-dependent PGT-A platforms for precise ICN isolation with these mixing experiments [13, 14, 20, 34, 35]. A contrasting of 2 commonly utilized platforms that get used commercially, verified high resolution amongst mosaic intervals (20% for Veriseq [Illumina from San Diego, CA/Vitrolife, Gothenburg, Sweden] as well as 30% for Reproseq [Thermofisher , Waltham, MA]) [36]. This illustrated the degree of precision contradicted the belief that the intermediate results for mosaic embryos seen in clinical studies might be secondary to their being a combination of wrongly diagnosed uniform euploid in addition to aneuploid embryos (this is a belief that further ignores that large quantity of results which demonstrate the common occurrence of existence of mosaicism in embryos). Equal significance is there with regards to every PGT-A platform as well as center to give the definition of the precise quality regulation cut offs with the noise-quantification metrics with regards to the evaluation software for prevention of a confusing karyotype profiles (secondary to noise due to technique) from them getting a classification of mosaic just as the values fall amongst the ICN range. In these cases, the blastocysts that are the source are required to get to be handles in the form of undiagnosed embryos or a consideration for a repeated biopsy.
Thus the conclusions drawn are a high complicated mosaic sample, like needs to generate a kin outcomes across various laboratories for every mosaic sub group. Any kind of PGT-A methodology that rightly isolates mosaicism would finally generate clinical results correlations akin to those found in the 100 mosaic embryo study, thus the ranking system could be transferable from clinic to clinic.
The Embryo Biopsy Sample-Despite not Perfect, a Useful Replacement for Embryos
With regards to the anticipation significance of the embryo biopsy sample, PGT-A is markedly separate from its so called cousin, diagnostic pre implantation genetic testing (PGT) for monogenic disorders (PGT-M). In case of PGT-M, the biopsy sample acts as an optimal genetic representation of the rest of the blastocyst, in addition to the future fetus. While with regards to chromosomal evaluation with PGT-A, the process of mosaicism makes the part of the biopsy sample as illustrative become complicated. Aneuploidies that get obtained from meiotic mistakes are existent in the oocyte (or rarely in the sperm), influence the zygote that results, hence uniformly influences all the cells that belong to the blastocyst (other than in the rare occasion of rescue of the aneuploidy). Actually, totally euploid or aneuploid PGT-A outcomes from a trophectoderm biopsy sample have a predisposition to be well harmonious with the outcomes from the rest of the blastocyst [8, 37, 38], despite meiotic/mitotic mistakes are not conflicting as well as might coexist. Conversely, an outcome that pointed that mosaicism is existent in the trophectoderm biopsy sample is a bad anticipator of the embryos chromosomal make up [8], in view of the randomness in the sample collection of cells. Moreover, in view of the auto correction of as detailed earlier, an outcome of mosaicism in the blastocyst stage will occasionally (if anytime) be able to anticipate the karyotype of the placenta or fetus in the latter part of pregnancy .Thus it might appear to be counter productive that mosaicism estimated in the biopsy sample should be anticipative in any way.
However, the outcomes of the 1000 mosaic embryo transfer study are incontrovertible – mosaic profiles , in addition to greater than that levels as well as kinds of mosaicism estimated via PGT-A possessed a robust correlation with particular results [16]. Hence while agreeing with the restrictions as well as challenges totally with regards to biopsy, the outcomes pointed that it would be significant not to ignore the knowledge in context of mosaicism that the biopsy yields for the decision making as per the priority of the embryo for transfer as per the chances of clinical results yielding success.
Now the subsequent, query arises what is the frequency of embryonic mosaicism? Is it feasible to decide the incidence of mosaicism from the outcomes obtained from the biopsies? That is without the engineering of the mathematical interpolate. The biopsy just possesses the capacity of directly providing information with regards to the embryos percentage that has received the classification of being mosaic (in contrast to the euploid or aneuploid). Like if 15% of the embryos get the classification of belonging to the mosaic category as per evaluation that is conducted by the PGT-A it does not detail the actual incidence of mosaicism in all the blastocysts that get obtained from IVF,although still 2 reports are considered to be the same. For getting the knowledge with regards to the real incidence of mosaicism one needs to disassociate the unique blastocysts in addition to evaluate the ploidy at the level of single one in relation to all their cells. An experiment that is akin to that has not got conducted systematically with regards to large samples of blastocysts with the modern DNA copy number quantification strategies in view of the clear cut restrictions that are correlated with techniques, economic viability, in addition to sample that is available. The outcomes developed from the whole embryo FISH studies as well as evaluation, of single cell RNA sequencing knowledge pointed that, low level mosaicism (even to the extent that there is existence of only a single aneuploid cell amongst euploid cells) is very common in case of early embryos, besides might be existent in most of the human embryos. Nevertheless, such invisible (i.e ultra) low amounts of mosaicism possesses the least probability of getting picked up by PGT-A, in view of the random aspect of sampling in addition to does not hold any significance with regards to the embryo viability. This varies with from patient to patient with proof of high level mosaicism in the trophectoderm biopsy sample, which suggests an early mitotic mistake process with the following, progression to the cells that have descended.
Then the query arises is the utilization of the term ‘’mosaic’’ embryo appropriate, besides can we utilize it in any case? Repeatedly we need to get insight that the subgroups where we categorize the embryos with the aid of PGT-A are just dependent on the biopsy sample as well as not on the global evaluation, of the whole embryo. This implies that on labeling the embryo mosaic we are actually meaning that the embryo generated a PGT-A outcome that concordant with mosaicism. In the similar light, euploid embryo is the one with the biopsy outcomes that concordant with euploidy as well as aneuploid embryo is the one with the biopsy outcomes that concordant with aneuploidy. Thus the implication being that these labels are the shorthand with the idea of classification in addition to the management of embryos in the clinical scenario.
Conclusions
Thus the advancements in the modern PGT-A have resulted in stimulation in of a debate hat revolves around mosaicism in embryos-does it require to get a diagnosis in addition to the method of management of embryos in the clinical scenario? A lot of thoughts, viewpoints, predilections have been aired with regards to this topic. The existent outcomes pointed that the embryos with a diagnosis of mosaic possess, worst outcomes of properties in contrast to those where diagnosis is a euploid embryo, characteristic of mosaicism estimated by PGT-A are correlated with particular clinical results, besides babies whose birth take place from embryo transfer subsequent to a diagnosis of mosaicism by PGT-A are mostly impossible to differentiate babies whose birth take place from embryo transfer subsequent to a diagnosis of euploidy.
We are in the requirements of outcomes as early as feasible to confirm, further escalate its genuineness or totally discredit that data which the existence observations prove or to try to get greater insight towards the next few queries that are followed by like i) Is the existence of mosaicism in separate chromosomes correlated with varying clinical success outcomes? ii) What is the significance of the genomic amount of mosaic segmental imbalances to be able to influence? Is there any variation with regards to properties of mosaicism amongst the cell kinds as well as tissues? Is there any kind of chromosomal abnormalities display by the products of conception that got a miscarriage subsequent to a mosaic embryo transfer? The exact follow up work, separate from one done till now needed in the neonates?
An International registry of mosaic embryo transfers, recording the results in addition to if existent the prenatal evaluation besides the knowledge with regards to neonate would be of lots of help in this arena. Once there are new outcomes these existent quotations/ recommendations would either stand as it is or would require modification as per those outcomes. This holds true for any aspect of science, with same being true with regards to embryo mosaicism. Thus it is the data that needs to be allowed to do their talking for itself rather than our speculations.
References
-
Griffin DK, Handyside AH, Penkerth RJ, Winston RM, Delhanty JD (1991) Fluorescence in situ hybridization to interphase nuclei of humans preimplantation embryos with X and Y chromosome specific probes. Hum Reprod 6(1): 101-105.
-
Biesecker LG, Spinner NB (2013) A Genomic view of mosaicism and human disease. Nat Rev Genet 14(5): 3307-20.
-
Bieslanska M, Tan SL, Asangla A (2002) Chromosomal mosaicism throughout humans preimplantation development in vitro: incidence, type and relevance to embryo outcomes. Hum Reprod 17(2): 413-419.
-
Sandalinas M, Sadowy S, Alikani M, Tomkin G, Calderon G, et al. (2001) Developmental ability of chromosomally abnormal human embryos to develop to blastocyst stage. Hum Reprod 16(9): 1954-1958.
-
Delhanty JD, Harper JC, Asangla A, Handyside AH, Winston RM (1997) Multicolour FISH detects frequent chromosomal mosaicism and chaotic division in normal preimplantation embryos from female patients. Hum Genet 99(6): 755-760.
-
Munne S, Alikani M, Tomkin G, Grifo J, Cohen J (1995) Embryo morphology, developmental rates and maternal age are corrected with chromosomal abnormalities. Fertil Steril 64(2): 382-391.
-
Capalbo A, Poli M, Cimadomo D, Benini F, Patassin C, et al. (2020) Multicenter prospective non-selection study of blastocyst transfer of low-medium grade mosaicism. Fertil Steril 114(3): e414.
-
Marin D, Xu J, Treff NR (2021) preimplantation genetic testing for aneuploidy: A review of published blastocyst reanalysis of concordance data. Prenat Diagn 41(5): 545-53.
-
Starostik MR, Sosina OA, McCoy RC (2020) Single cell analysis of human embryos reveals diverse patterns of aneuploidy and mosaicism. Genome Res 30(6): 814-825.
-
Yang M, Rito T, Metzger J, Naftaly J, Soman R, et al. (2021) Depletion of an euploid cells in human embryos and gastruloids. Nat Cell Biol 23: 314-321.
-
Cavazza T, Takeda Y, Politi AZ, Aushev M, Aldag P, et al. (2021) Parental genomic unification is highly error prone in mammalian embryos. Cell 184(11): 2860-2877.
-
Greco E, Minasi MG, Fiorentino F (2015) Healthy babies after intrauterine transfer of mosaic aneuploid blastocysts. N Engl J Med 373(21): 2089-2090.
-
Munne S, Blazek J, Large M, Martinez-Ortiz MA, Nilson H, et al. (2017) Detailed investigation into the cytogenetic constitution and pregnancy outcome of replacing mosaic blastocysts detected with the use of high resolution and next generation sequencing. Fertil Steril 108(1): 62-71. e8.
-
Victor AR, Tyndall JC, Brake AJ, Lepkowsky LT, Murphy AE, et al. (2019) One hundred mosaic embryos transferred prospectively in a single clinic: exploring when and why they result in healthy pregnancies. Fertil Steril 111(2): 280-293.
-
Zhang L, Wei D, Zhu Y, Gao Y, Yan J, et al. (2019) Rates of live births after mosaic embryos transfer compared with euploid embryo transfer. J Assist Reprod Genet 36(1): 165-172.
-
Viotti M, Victor A, Barnes F, Zouves C, Besser A, et al. (2021) Using outcome data from One thousand hundred mosaic embryos transfer to formulate an mosaic embryo ranking system for Clinical use. Fertil Steril 115(5): 1212-1224.
-
Zhang YX, Chen JJ, Nabu S, Yeung OS, Li Y, et al. (2020) T he pregnancy outcome of mosaic embryos transfer:a prospective multicenter study and meta-analysis. Genes (Basel) 11(9): 973.
-
Singla S, Iwamoto Stohl LK, Zhu M, Zer- nicke Goetz M (2020) Autophagy mediated apopto- sis eliminate aneuploid cells in a mouse model of chro- mosomal mosaicism. Nat Commun 11: 1-15.
-
McCoy RC, Newnham LJ, Ottolini CS, Hoff- mann ER, Chazimetatiou K, et al. (2018) Tripo- lar chromosme segregation drives the association be- tween maternal genotypeatvariants spanning PLK4 and aneuploidy in human preimplantation embryos. Hum Mol Genet 27(14): 2573-2585.
-
Maxwell SM, Colls P, Hodes-Wertz B, McCulloh DH, McCaffrey C, et al. (2016) Why do euploid embryos miscarry? A case control study comparing rate of aneuploidy within presumed euploid embryos that resulted in miscarriage or live birth using or next generation sequencing. Fertil Steril 106(6): 1414-1419.
-
Viotti M, McCoy RC, Griffin DK, Madjunkov M, Madjunkov S, et al. (2021) Let the data do the talking: the need to consider mosaicism during embryo selection. Fertil Steril 116(5): 1212-1219.
-
Kulvinder KK, Allahbadia GN, Singh M (2021) “Can we resolve the controversy with regards to embryo transfer of blastocysts diagnosed as mosaic subsequent to PGT- A-A Short Communication’’ under review.
-
Viotti M, Victor A, Barnes F, Zouves C, Besser AG, et al. (2020) New insights from One thousand mosaic embryo transfers: features of mosaicism dictating rates of implantation, spontaneous abortions and neonatal health. Fertil Steril 114(3): e1-2.
-
Cram DS, Leigh D, Handyside A, Rechitsky L, Xu K, et al. (2019) PGDIS position statement on the transfer of mosaic embryos. Reprod Biomed Online 39(1): e1-4.
-
Catticchio G, Barne A, Lagalla C, Boini A, Fishel S, et al. (2021) Plasticity of the human preimplantation embryo development dogmas, variations on themes and self- correction. Hum Reprod Update 27(5): 848-865.
-
Sheltzer JM, Amon A. (2011) The aneuploidy paradox: costs and benefits of an incorrect karyotype. Trends Genet 27(11): 446-453.
-
Esteki MZ, Viltrop T, Tsuiko O, Tirats A, Koel M, et al. (2019) In vitro fertilization does not increase the incidence of de novo copy number alterations in fetal and placental lineages. Nat Med 25(11): 1699-1705.
-
Popovic M, Dhaenens I, Taelman J, Dheedene A, Bialecka M, et al. (2019) Extended In vitro cultures of human embryos demonstrates the complex nature of diagnosing chromosomal mosaicism from a single trophectoderm biopsy. Hum Reprod 34(4): 758-769.
-
Bolton H, Graham SJ, van der Aa N, Kumar P, Theuris K, et al. (2016) Mouse model of chromosomal mosaicism reveals lineage specific depletion of aneuploid cells and normal development potential. Nat Commun 7(1): 11165.
-
Kabraman S, Cetinkaya M, Yuskel B, Yesil B, Pirkevi Cetinkaya C (2020) The birth of baby with mosaicism from a known mosaic embryo transfer: a case report. Hum Reprod 35(3): 727-733.
-
Taylor TH, Gitlin SA, Patrick JL, Crain JL, Wilson JM, et al. (2014) The origin, mechanisms, incidence, and Clinical consequences of chromosomal mosaicism in humans. Hum Reprod Update 20(4): 571-581.
-
Gueye NA, Deskota B, Taylor D, Pfundt R, Scott RT, et al. (2014) Uniparental disomy in the human blastocyst is exceedingly rare. Fertil Steril 101(1): 232-236.
-
Tiegs AW, Tao X, Zhao Y, Whitehead C, Kim J, et al. (2021) A multicenter , prospective, blinded, nonselection study evaluating the predictive value of an aneuploid diagnosis using a targeted next-generation sequencing-based preimplantation genetic testing for aneuploidy assay and impact of biopsy. Fertil Steril 115(3): 627-637.
-
Popovic M, Dheedene A, Christodolou C, Taelman J, Dhaenens I, et al. (2018) Chromosomal mosaicism in the human blastocysts:the ultimate challenge of preimplantation Genetic testing? Hum Reprod 33(7): 1342-1354.
-
Zhou S, Xie P, Zhang S, Hu L, Luo K, et al. (2021) Complex mosaic blastocysts after preimplantation Genetic testing: Prevalence and outcomes after re- biopsy and re-vitrification. Reprod Biomed Online 43(2): 215-222.
-
Biricick A, Continnea E, Minasi MG, Greco PF, Bono S, et al. (2021) Cross validation of next generation sequencing technologies for diagnosis of chromosomal mosaicism, and segmental aneuploidies in preimplantation embryos model. Life (Basel) 11(4): 340.
-
Popovic M, Dhaenens I, Boel A, Menten B, Heindricks R (2020) Chromosomal mosaicism in the human blastocysts:the ultimate diagnostic dilemma. Hum Reprod Update 26(3): 313-334.
-
Victor AR, Griffin DK, Brake AJ, Tyndall JC, MurphyAE, et al. (2019) Assessment of aneuploidy concordance between Clinical trophectoderm biopsy and blastocysts. Hum Reprod 34(1): 181-192.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’