Cytokine Profile Changing in Pregnant Women with Chorioamnionitis
During our research, we had studied the level of serum proinflammation and anti-inflammation cytokines in 25 women in the third trimester of pregnancy with premature rupture of membranes and in 29 patients with premature rupture of membranes (PROM) complicated by chorioamnionitis. The control group consisted of 28 women with physiological pregnancy in the third trimester and 27 women with onset of labor. There was a difference in the synthesis of cytokines during pregnancy in the third trimester from the level of cytokines at the onset of labor. In women with PROM and chorioamnionitis with gestational age
Introduction
Premature rupture of membranes is the outflow of amniotic fluid from the space around the fetus at any time before the onset of labor. Labor often begins soon after rupture of the membranes. If labor does not begin within 6-12 hours, the risk of infection for the woman and the fetus increases [1, 2].
Chorioamnionitis is usually results of infections caused by bacteria, which enter from the vagina into the uterus, but it is also associated with premature or prolonged labor. It triggers an inflammatory response by releasing various inflammatory signaling molecules, which leads to an increase in the release of prostaglandins and metalloproteases. These substances contribute to the contraction of the uterus and the maturation of the cervix, which causes premature birth [3, 4].
It was noted that more active reproduction of opportunistic and pathogenic microorganisms occurs during weakness of the body’s defences. The provoking factors of immune deficiency are colds, exacerbations of extragenital pathology, prolonged or intense physical and mental stress, taking medications with a direct or secondary immunosuppressive effect [5, 6].
The dynamics of any disease with an immunopathogenetic basis should be considered from the point of view of the interaction of the immune system effector links, which participation in pathological processes is largely due to the cytokine cascade [7, 8]. The role of immune component is greatin the pathogenesis of PROM with chorioamnionitis, which triggers the entire cascade of pro- and anti- inflammatory cytokines (IL-1β, IL-4, IL-6, IL-8, TNF α). A number of authors believe that a high concentration of cytokines reflects the activity and severity of the pathological process [9, 10].
Aim
The aim of this study was to study levels of IL-1β, IL-4, IL-6, IL-8, IFNγ, TNFα in the serum in women with PROM with and without chorioamnionitis.
Materials and Research Methods
The study of the cytokine profile in blood serum was carried out in 54 pregnant women. 25 of them had PROM and 29 had PROM combined with choriamnionitis. The control group consisted of 28 women with physiological pregnancy in the third trimester of gestation and 25 women with onset of labor. The age of the women ranged from 20 to 35 years, which averaged 26.5 ± 0.6 years. The gestation period ranged from 37 to 40 weeks. 55.8% of them were primiparous, 44.2% were multiparous, which the total number of pregnancies were not more than five. Of the concomitant diseases, chronic diseases of the urinary system, diseases of the thyroid gland, and the cardiovascular system were more often diagnosed. Complications of the first half of pregnancy were noted in 33.3% of women, in 29.4% of women, the first half of pregnancy was complicated by early toxicosis, the frequency of threatened abortion was 17.6%, and 15.6% of women had complications in the second half of pregnancy.
The level of cytokines IL-1β, IL-4, IL-6, IL-8, IFNγ, TNFα in the blood serum was determined using the test systems of “Vector Best”, (Russia), by the method of the “sandwich”- option of the immune-enzymatic solid-phase assay with the help of double antibodies, according to the manufacturer’s recommendations. The indicator component of the reaction was a streptavidin-HRP conjugate. In each reaction recombinants IL-1β, IL-4, IL-6, IL-8, IFNγ, TNFα, were used as a standard for comparison, which are part of the test systems. Based on the titration data of standard samples, calibration curves were constructed for each of the cytokines, which were used to determine their level in the test fluid in the range of detectable clone concentrations from 10 to 2000 pg / ml.
Statistical processing of the obtained results was carried out with the calculation of the arithmetic mean (M), its error (m), Student’s test (t).
Results and its Discussion
The results of the study of the level of pro- and anti-inflammatory cytokines in women with PROM and chorioamnionitis showed that there are changes in the concentration of the studied cytokines (Table 1).
| Immunological Indicators, pg/ml | Control group. Women in labor, n=27 | PROM n=30 | Chorioamnionitis, n=29 |
|---|---|---|---|
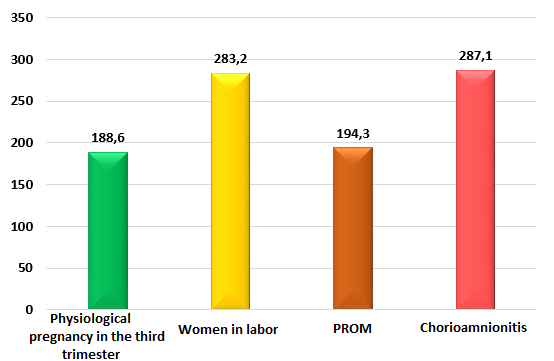
| IL-1β | 283,2 ± 14,1 | 194,3 ± 16,5* | 287,1 ± 23,1** |
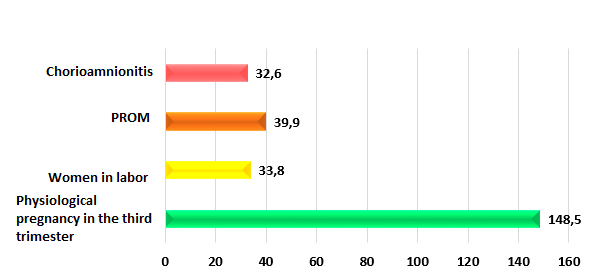
| IL-4 | 33,8 ± 2,4 | 39,9 ± 2,8 | 32,6 ± 3,8 ** |
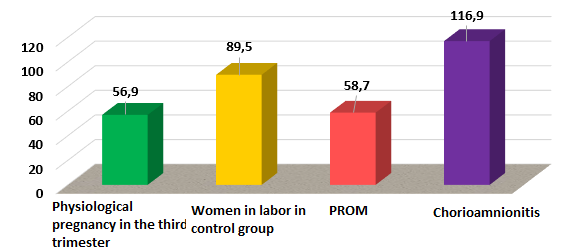
| IL-6 | 89,5 ± 5,9 | 58,7 ± 2,6* | 116,9 ± 13,4 * ** |
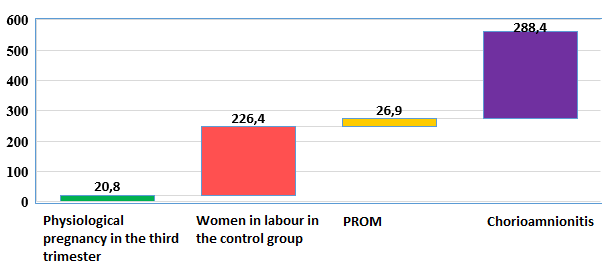
| IL-8 | 226,4 ± 17,3 | 26,9 ± 1,8* | 288,4 ± 18,3* ** |
| IFNγ | 32,8 ± 2,7 | 49,2 ± 2,4* | 62,6 ± 8,4* |
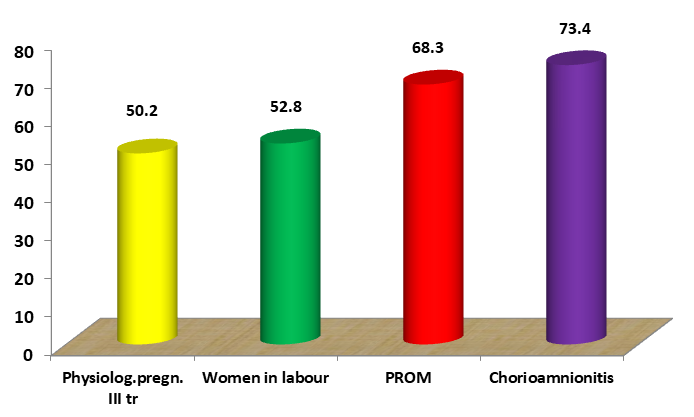
| TNFα | 52,8 ± 2,9 | 68,3 ± 3,8* | 73,4 ± 4,3 |
In women with PROM, there was a tendency to an increase in the level of IL-1β compared with those of women with physiological pregnancy in the third trimester, which averaged 194.3 ± 16.5 pg / ml versus 188.6 ± 13.5 pg/ ml. However, when compared with the data of women with the onset of labor, the level of IL-1β in women with PROM was almost 1.5 times lower (P <0.05). In women with chorioamnionitis, the level of IL-1β was significantly higher than in women with PROM, averaging 287.1 ± 23.1 pg / ml, (P <0.05) and 1.5 times higher than in women with physiological pregnancy in the third trimester (P <0.01), but was at the level of values of women with the onset of labor (Figure 1).
According to S.A. Ketlinsky and A.S. Simbirtseva (2008), IL-1β is secreted by producing cells not by the classical pathway of protein secretion. The formation of biologically active secretory forms occurs in a similar way to IL-18 and IL-33. It has been shown that the level of secretion of IL-1β, from which the cascade of production of immunoregulatory cytokines begins, changes during the physiological course of pregnancy during critical periods of fetal development [8]. According to a number of authors, increased secretion of IL-1 can play an important role in the pathogenesis of pregnancy complications, which can lead to fetal rejection.
The IL-4 level in women with PROM is significantly lower than the values of pregnant women in the third trimester (39.9 ± 2.8 pg / ml, P <0.001) and slightly lower than the values of women with onset of labor (33.8 ± 2.4 pg / ml). In women with chorioamnionitis, the level of IL-4 is lower than in women with PROM (32.6 ± 3.8 pg / ml, P <0.05) and women with physiological pregnancy in the third trimester of gestation (P <0.001), (figure 2).
IL-4 has a wide spectrum of biological effects, the most famous are suppression of the inflammatory response and an increase of humoral immunity [10]. This cytokine is involved in the activation of T-suppressors, the expression of receptors for steroid hormones [3, 5]. According to N.K. Tetruashvili (2000), in women with pregnancy pathology, a strong direct correlation was found between a high level of IL-6 and preterm birth [7, 9]. It has been shown that the level of IL-6 in the amniotic fluid is a sensitive test and can reveal the presence and severity of intrauterine infection of the fetus.
In our studies, when comparing the concentration of IL-6 in the examined women, was found that with PROM the level of this cytokine averaged 58.7 ± 2.6 pg / ml, i.e., whereas in women with physiological pregnancy in the third trimester it was at the level of values and 1.5 times lower than in women with the onset of labor (P <0.05). While in women with chorioamnionitis, the level of this cytokine was 2 times higher than the values of women with PROM, (P <0.01), averaging 116.9 ± 13.9 pg / ml, (Figure 3) and 1.3 times higher than in women with the onset of labor (P <0.05).
IL-6 includes various mechanisms, in particular, in synergism with TNFα stimulates the production of IL-1β and IL-8 [6, 8]. The main producers are Th2, macrophages, neutrophils, fibroblasts, endothelial cells.
Chemotactic and activating factor for neutrophils - IL-8 plays an important role in pregnancy, as it actively participates in all processes of the reproductive system [9, 10]. In our study, the level of this cytokine in women with PROM averaged 26.9 ± 1.8 pg / ml, which is significantly higher than the values of pregnant women in the third trimester of gestation (P <0.05) (Figures 3,4). And in women with chorioamnionitis, the level of IL-8 was significantly higher than in women in labor in the control group and averaged 288.4 ± 30.3 pg / ml, (P <0.001). IL-8 has been found in the cervix, placenta, and endometrium. According to P. Caballero-Campo (2002), IL-8 is secreted by endometrial cells in the region of the implantation window, inducing leukocyte recruitment and expression of adhesion molecules. It is assumed that there is a double regulation of chemokine production: hormonal (progesterone) and the implanting embryo.
IL-8 is produced during physiological pregnancy, but its production is increased in chorioamnionitis. According to several authors, placental cells with multiple endocrine functions exhibit immunological functions through the production of IL-1 and TNFα, which stimulate the release of placental IL-8. The diversity of the discovered and already studied functions of IFN attests to its control-regulatory role in maintaining homeostasis [7, 8].
The results of the studies conducted to study the level of IFNγ in pregnant women with PROM showed that, on average, its content was 49.2 ± 2.4 pg / ml, which was 1.5 times higher than the values of women in labor in the control group, (P <0.01), (Figure 5). While in women with chorioamnionitis, the level of IFNγ was higher than in women with PROM and averaged 62.6 ± 7.4 pg / ml (P <0.01).
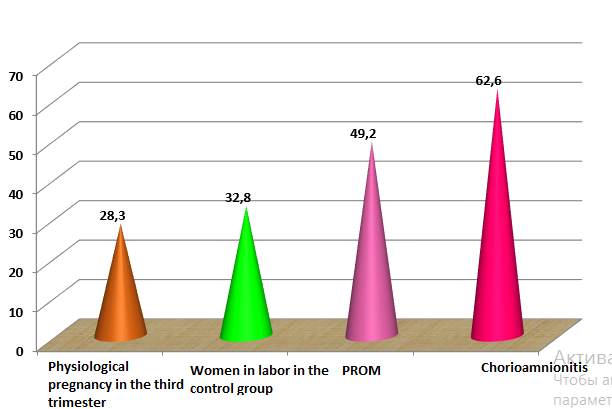
According to the literature, excess production of interferons inhibits the secretion of factors necessary for the growth and differentiation of the trophoblast. IFNγ activates NK cells and cytotoxic T lymphocytes to form lymphokine activated killer cells with the potential to damage the trophoblast. In this case, high doses of IFNγ initiate platelet aggregation up to the development of thrombocytopenia. Despite the absence of interferon-binding receptors on these cells, this cytokine clearly activates the production of thromboxanes in leukocytes, cells of the reticuloendothelial system and endothelial cells [10]. The increased production of interferon in infectionin pregnant women indicates the activation of maternal Th1 cells, which mediate the most dangerous cellular immune response for the fetus [8, 10].
TNF is one of the most pleiotropic cytokines affecting all cells, altering their growth, differentiation and survival, plays an important role in the dynamics of pregnancy [7, 8]. M.L. Casey and other authors (1989) found that TNF is not detected in amniotic fluid during normal pregnancy in the second trimester, before or after the onset of labor; but were present at premature birth.
In our study, the level of TNFα in women with PROM averaged 68.3 ± 3.8 pg / ml, which is 1.3 times higher than in women in labor - 52.8 ± 2.9 pg / ml (P <0 , 05), (Figure 6), while in women with chorioamnionitis, the concentration of TNFα averaged 73.4 ± 4.3 pg / ml (P <0.1). According to some authors, the formation of cytokines in macrophage- like cells of decidual tissue may play a fundamental role in the pathogenesis of premature labor. Decidual macrophages spontaneously synthesize significant amount of TNF.
Thus, our research about the study of cytokines showed that during physiological pregnancy, there is an activation of such cytokines as IL-1β and IL-4, which contribute to the immunosuppression of the maternal organism relative to the semi-allogeneic fetus. A radical change in the level of these cytokines is observed during the development of labor, when immunosuppression is removed and the mother’s body is ready to reject the fetus. Analysis of the study results of the cytokine status in women with PROM with and without chorioamnionitis showed that the nature of changes in the level of cytokines in this pathology corresponds to the indicators of women with the onset of labor. Premature
rupture of membranes leading to labor is associated with increased levels of pro-inflammatory cytokines. The reasons for the increase can be various factors, including infections that cause chorioamnionitis.
Findings
- In women with premature rupture of membranes (PROM), the concentration of cytokines - IL-1β, IL-6 and IL-8 is approximately at the level of the values of women with physiological pregnancy in the third trimester, the level of IL-4 is slightly higher than the values of women with the onset of labor activities.
- Women with PROM and chorioamnionitis are characterized by a sharp increase in pro-inflammatory (IL-1β, IL-6, IL-8, TNFα and IFNγ) cytokines and a decrease in anti-inflammatory (IL-4) cytokine.
References
-
Arango DG, Descoteaux A (2014) Macrophage cytokines: involvement in immunity and infectious diseases. Front Immunol 5(491): 1-12.
-
Ikhtiyarova GA, Tosheva II, Aslonova MJ, Dustova NK (2020) Prenatal Rupture of Amnion Membranes as a risk of development of obstetrics pathologies. European Journal of Molecular & Clinical Medicine 7(7): 530-535.
-
Ikhtiyarova GA, Tosheva II, Nasrullayeva NS (2017) Causes of fetal loss syndrome at different gestation times. Asian Journal of Research 3(3): 13-30.
-
Tosheva II, Ikhtiyarova GA, Aslanova MJ (2019) Introduction of childbirth in women with the discharge of amniotic fluid with intrauterine fetal death. Journal of Problems and solutions of advanced scientific research 1: 417-424.
-
Tosheva II, Ikhtiyarova GA (2019) Obstetric complications in pregnant women with premature discharge of amniotic fluid. Problems of biology and medicine 115: 146-149.
-
Ikhtiyarova GA, Dustova NK, Kurbonova ZSH (2020) Modern methods for diagnostics and prevention of thromboembolic complications in pregnant women with ectasia of the pelvic vines. New Day in Medcine 1(29): 211-215.
-
Tosheva II, Ikhtiyarova GA (2020) Pregnancy outcomes with premature rupture of membranes. Journal of RMZh. Mother and child 1: 16-20.
-
Tosheva II, Ashurov NG, Ikhtiyarova GA (2020) Rupture of membranes in prematurity as a factor in the development of obstetric complications. Journal of Problems of Biology and Medicine 1: 76-79.
-
Tosheva II, Ashurova NG (2019) Labor outcomes in pregnant women with premature rupture of amniotic fluid. Bulletin of the Dagestan State Medical Academy 4(33): 34-38.
-
Ikhtiyarova GA (2019) Optimization of diagnostics and methods of termination of pregnancy at different periods of gestation in women with antenatal fetal death. Monograph Durdona, pp: 136.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’