Types and Distribution of Fetal Congenital Anomaly and their Maternal Characteristics in High Risk Pregnancy Unit of Dhaka Medical College Hospital, Bangladesh
Introduction: Congenital anomaly is one of the important causes of perinatal mortality and morbidity. Proper information regarding its prevalence, distribution as well as risk factors can help policy makers to take appropriate steps for prevention. Materials and Methods: A hospital record based observational study was done in Obstetric department of Dhaka Medical College Hospital, Bangladesh during the year of 2020. The aim of the study is to evaluate the pattern of anomaly found in admitted patients in Maternal Fetal Medicine unit, along with the maternal demographic profile and associated diseases. After taking ethical clearance and permission from department detailed information was collected and analysis was done. Results: In the year 2020 total 6012 delivery was occurred and 4.42% of them were anomalous baby. The maternal characteristics showed that mean maternal age was 26.24(±5.25) years. 20.7% of mother had previous history of abortion, 7.7% has previous perinatal death and 3.3% have previous anomalous baby. 5.49% mother had Diabetic disorders and 4.39% had congenital heart disease. Associated poly hydramnios was found in 17.7% and oligohydramnios was found in 12.1% of cases. The distribution pattern of anomalies according to system involved showed that 41.7% was Central Nervous System anomaly, 8.7% was Renal anomaly, 6.5% was Musculoskeletal anomaly, 4.4% was Gastrointestinal anomaly,6.6% had body wall defect , 10.9 % was Non immune Hydrops, 3.3% was Syndromic baby and 13.1% had multiple congenital anomaly. Conclusion: It is a tertiary hospital based study. So it may not reflect the actual picture of population. So community based study is needed for further advancement.
Introduction
Congenital anomalies are also known as birth defects, congenital disorders or congenital malformations. Congenital anomalies can be defined as structural or functional anomalies (for example, metabolic disorders) that occur during intrauterine life and can be identified prenatally, at birth, or sometimes may only be detected later in infancy, such as hearing defects. An estimated 295000 newborns die within 28 days of birth every year, worldwide, due to congenital anomalies [1]. Congenital anomalies are a significant cause of disability, chronic illness, and childhood death in many countries and affect approximately 1 in 33 infants. They result in an estimated 3.2 million birth defect- related disabilities every year [2]. Although congenital anomalies may be the result of one or more genetic, infectious, nutritional or environmental factors, it is often difficult to identify the exact causes. Some congenital anomalies can be prevented. Vaccination, adequate intake of folic acid or iodine through fortification of staple foods or supplementation, and adequate antenatal care are just 3 examples of prevention methods [1]. The prevalence of congenital anomalies at birth varies greatly worldwide, ranging from 1.07% in Japan to 4.3% in Taiwan [2]. In Egypt it is found 2.06% [3] and in the United States, they occur in about 3% of newborns [4]. In Bangladesh the prevalence was found 2.03% in one study [5] and it is attributable for 12.7% of NMR in Bangladesh [6]. The prevalence rates of congenital anomalies recorded in developing countries are likely to be underestimated due to unavailability of diagnostic capabilities or accurate medical records, as well as underreporting [6]. Knowledge about the prevalence of congenital anomalies is useful to obtain baseline rates, documenting changes over time, and identifying clues to the etiology of conditions. For the above purposes a study on congenital anomalies was undertaken. Objectives of our study were to analyze the maternal demographic profile with associated medical and obstetrical conditions and to find out the distribution of congenital anomalies according to system involve.
Materials and Methods
The study was conducted at Maternal-Fetal Medicine unit (MFM unit) of Obstetrics and Gynecology Department, (which deals with the high risk pregnant patients) with joint collaboration of General Obstetric units and Dhaka Medical College Hospital (DMCH), Dhaka, Bangladesh from January 2020 to December 2020. It was a hospital record based retrospective observational study. The ethical clearance for this study was taken from the Ethical Review Committee (ERC) of Dhaka Medical College. The data were obtained from the admission book of Maternal-Fetal Medicine unit and record office of the maternity section of the Dhaka Medical College Hospital, Dhaka. The yearly birth records in various units (MAT-I to MAT- VI) in the General Obstetrics sections containing the number of babies born in each month was the source of information. The total number of births for the period of study was strictly noted and recorded. The hospital files of Maternal-Fetal Medicine Unit containing records of congenital malformations in detail. From these records maternal characteristics were analyzed in relation to age of the mother, parity of the mother, previous history of abortion, prenatal death and gestational age of the fetus at diagnosis. Influence of risk factors like maternal Diabetes and other associated medical and obstetrical complications on congenital anomaly was studied. Fetal malformations were grouped according to major system involved. Percentages and incidences were calculated and presented in tables. Quantitative variables were analyzed and presented by mean and standard deviations. SPSS version 16 was used for analyzing data.
Results
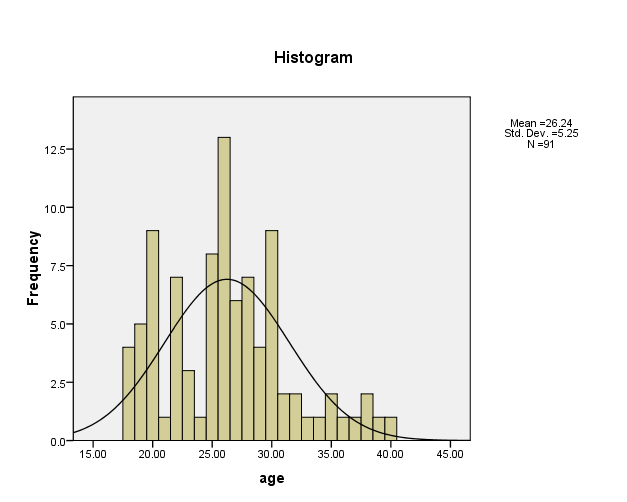
In the year 2020, DMCH Obstetrics and Gynecology Department (Six general Obstetric units and one Maternal- Fetal Medicine unit) had delivered 6012 patients. Out of them 266 deliveries were ended by production of congenital anomaly babies. The incidence of anomaly babies was 4.42% of total deliveries in DMCH. In Maternal Fetal Medicine Unit of DMCH 656 patients were admitted in 2020 and 91 of them (13.88%) were consisted of anomaly fetus [7]. Further analysis was done among these 91 patients with anomalous fetus because information of these patents was kept in detail. Total 91 patients came with anomaly fetus in MFM Unit, DMCH in 2020 (13.8% of total admission in high risk pregnancy unit). The mean age of the study population was 26.24(±5.25) years and the maximum number (50.54%) of patients were between 25 to 30 years of age. The age range is from 18 to 40 years (Figure 1).
| Maternal Characteristics | No of patients | Percentage | |
|---|---|---|---|
| Para | Primi para | 25 | 27.50% |
| Multi para | 66 | 72.50% | |
| H/O Abortion | Present | 19 | 20.90% |
| Absent | 72 | 79.10% | |
| H/O Previous peri-natal Death | Present | 7 | 7.70% |
| Absent | 84 | 92.30% | |
| H/O Previous Anomaly Baby | Present | 3 | 3.30% |
| Absent | 88 | 96.70% |
Table 1: Maternal characteristics. Obstetric events among 91 patients showed that 27.5% was primi gravida and rest are multi grav
| Disorders | Class | No of patients | Percentage |
|---|---|---|---|
| Diabetic Disorder | Present | 5 | 5.49% |
| Absent | 86 | 94.51% | |
| Heart disease | Present | 4 | 4.39% |
| Absent | 87 | 95.61% | |
| Hypertensive Disorder | Present | 4 | 4.39% |
| Absent | 87 | 95.61% | |
| Other (Bronchial Asthma) | Present | 1 | 1.09% |
| Absent | 90 | 98.91% |
Table 2: Associated maternal medical Disorder. In our study 5.49% patients had Diabetic disorder and 4.39% had Heart disease whic
| Disorder | Number of cases | Percentage |
|---|---|---|
| Oligohydramnios | 11 | 12.10% |
| Polyhydramnios | 16 | 17.70% |
Table 3: Associated amniotic fluid disorder.
Table 3 shows 12.1% of patients had associated oligohydramnios and 17.7% had polyhydramnios.
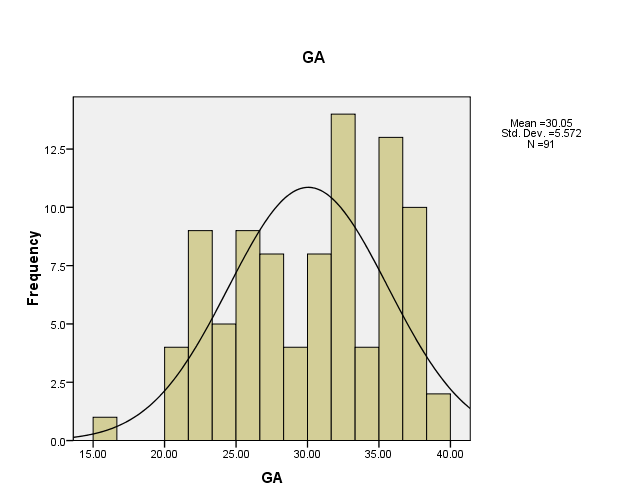
In this study mean gestational age of diagnosis of congenital anomaly was 30.05(±5.57) weeks. Only 1.1% of anomaly was detected before 20 weeks of gestation. In 42.85% of cases anomaly was found between 20 to 30 weeks and the rest of the cases (56.04%) were diagnosed after 30 weeks of gestation (Figure 2).
Discussion
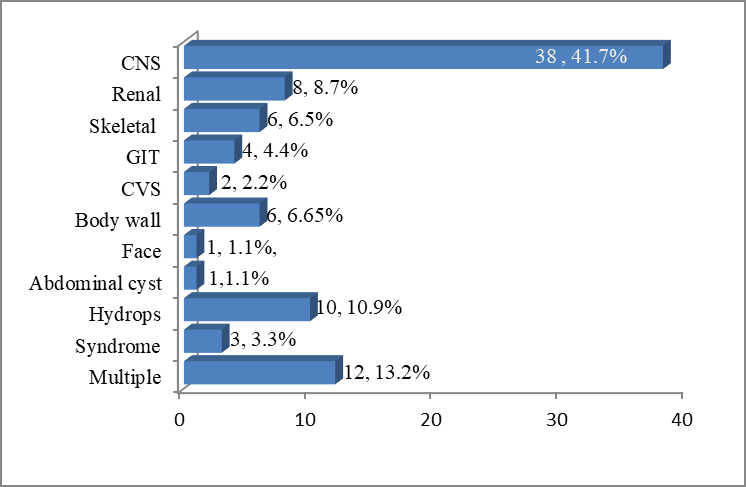
Dhaka Medical College Hospital (DMCH) is the largest hospital of Bangladesh and it is a tertiary care centre which is fully supported by government, so critical patients came here from all over the country for better treatment in low cost. In 2020 the percentage of congenital anomaly in DMCH was 4.42% of total obstetric patients which seems to be a little bit higher from the general population, as many primary health centers do not deal with anomaly fetus rather refer them. The incidence of anomaly among different countries varies in their hospital based studies from 0.36% in Iraq, 1.07% in Japan, 2.06% in Egypt, 2.15% in India, about 3% in USA, 4.03% in Taiwan, 4.4% in Uganda and 6.3% in Nigeria [2, 3, 4, 8, 9, 10]. Almost all of these studies are hospital based and are comparable to each other, but we have to admit that Hospital-based study cannot project the actual incidence among total population. Community based study should be ideal for true estimation of incidence of congenital anomalies in a population. Regarding maternal characteristics the mean maternal age in our study was 26.24(±5.25) years and the maximum number (50.54%) of patients were between 25 to 30 years of age group. Ameen, et al. [2] also showed that the mean maternal age of having anomaly fetus was 27.1(±6.6) which is very close to ours. Pandala, et al. [8] showed that the maximum patients were in age group of between 20-30 years. So it is noticeable that anomaly can occur in any maternal age, even as early as at 18 years (4.39%). Maternal obstetric events in our study showed that 27.5% of patents were primi gravid, 20.9% had previous one or more abortion, 7.7% had previous perinatal death and 3.3% have previous anomaly baby. Dewangan, et al. [11] showed 16.5% and Ameen, et al. [2] showed 10.8% of mothers having history of abortion which are a little less than our study. Pandala, et al. [8] and Ameen, et al. [2] also counted previous anomaly babies which were 9.7% and 20.8% respectively, a fur more than our count. Maternal medical disorders, specially Diabetic disorders and congenital heart disease of mother sometimes predisposes occurrence of anomalies. In our study 5.49% of mother had Diabetes and 4.39% had congenital heart diseases. Dewangan, et al. [11] found 3.5% of mother as Diabetic but Mahmood, et al. [3] found the percentage as high as 25.2%. Amniotic fluid disorders were found in association with anomaly frequently. It may be the effects of anomaly or may be the cause of anomaly. In our study 12.1% pregnancy was complicated with oligohydramnios and 17.7% were with poly hydramnios. Mahmood, et al. [3] found 10.7% polyhydramnios and 14.6% oligohydramnios in their study which is comparable with our study. Gestational age at which a congenital anomaly detected is important in respect of its management. The earlier it is diagnose, more options are available regarding intervention. In our study only 1.1% of anomaly was detected before 20 weeks of gestation. In 42.85% of cases anomaly was found between 20 to 30 weeks but a large proportion (56.04%) are diagnosed after 30 weeks of gestation. Westphal, et al. [12] conducted their study in a Fetal Medicine OPD and found that 8.5% of anomaly was detected before 14 weeks, 51.1% within 14 to 21 weeks, 28.7% within 22 to 28 weeks and only 11.7% after 28 weeks. So it can be said that high quality OPD service can ensure early detection and timely intervention. The percentage of anomaly that involves different system is varied widely in different study. As a major proportion of study were conducted in neonatal and pediatric department where lethally anomalous babies cannot reach, so they did not show percentage of those anomalies (eg. anencephaly, gross hydrops, etc). The studies in pediatric and neonatal departments commonly showed musculoskeletal abnormalities as leading one followed by cardiovascular, nervous system and gastrointestinal anomalies. But the findings are similar among studies in obstetrics department. In our study CNS anomaly found in 41.7%, Renal 8.7%, Musculoskeletal 6.5%, Gastrointestinal 4.4%, cardiovascular 2.2%, Hydrops 10.9% and Multiple anomaly in 13.2%. Ameen, et al. [2] found 37.7% CNS, 23.1% Musculoskeletal, 20.8% GIT, 5.4% cardiovascular and 4.6% Multiple anomaly. On the other hand Eluwa, et al. [13] showed 36.3% CNS, 18.1% Musculoskeletal, 31.83% GIT and 4.55% cardiovascular anomalies. So it noticeable that, anomalies of Central Nervous system are leading defect which are lethal in majority cases and leads to fetal and perinatal deaths.
Conclusion
Congenital anomaly possess a load in health system due to morbidity and mortality of neonate, infant and also sometimes in later life. Updated information about current situation will help to reduce this burden by more structured antenatal care and early detection of anomaly.
Acknowledgements: I like to express my gratitude and acknowledge the following persons for their active participation and inspiration through-out this research work:
- Prof. Dr. Salma Rouf, Head of Maternal Fetal Medicine Unit of Obs and Gynae department, Dhaka Medical College Hospital.
- Prof. Dr. Nilufer Sultana, Head of the department of Obs and Gynae, Dhaka Medical College Hospital.
- Brig. General A K M Nasir Uddin, Director, Dhaka Medical College Hospital.
- Prof. Dr. S.M. Shamsuzzaman, Chairman, Ethical Review Committee, Dhaka Medical College
- All Subspecialty trainee of Maternal Fetal Medicine, Dhaka Medical College Hospital. Conflict of Interest: There is no conflict of interest in this study.
Funding: Self-funding by authors.
Authors Contribution
- Dr. Mst Tajmira Sultana: Literature review , Protocol writing, Analysis of data, Report writing
- Dr. Jayanti Rani Dhar: Correspondence for data collection and compilation
- Dr. Tamanna Rahman: Correspondence for data collection and compilation
- Dr. Fahmida Byes Kakan: Literature retrieval and review
- Dr. Sanzida Mahmud: Result and Discussion review
- Dr. Israt Jahan: Compilation of data.
References
-
(2020) Congenital anomalies fact sheet. World Health Organization.
-
Ameen SK, Alalaf SK, Shabila NP (2018) Pattern of congenital anomalies at birth and their correlations with maternal characteristics in the maternity teaching hospital, Erbil city, Iraq. BMC Pregnancy Childbirth 18: 501.
-
Mahmood YA, Shawky RM, Soliman AAS, Ahmed MM (2011) Chromosomal study in newborn infant with congenital anomaly in Assiut University Hospital: cross sectional study. The Egyptian Journal of medical Human Genetics 12(1): 79-90
-
Christopher JLM (2015) Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385(9963): 117-171.
-
Siddika M, Sen S, Islam MN, Bhuiyan MK (2018) Pattern and Risk Factors of Congenital Anomaly in Newborn in a Tertiary Level Private Medical College Hospital, Bangladesh. Mymensingh Med J 27(4): 805-812.
-
(2016) WHO-MCEE estimates for child causes of death, 2000-2015, pp: 1-20.
-
Penchaszadeh VB (2002) Preventing congenital anomalies in developing countries. Community Genet 5(1): 61-69.
-
Pandala P, Kotha R, Singh H, Nirmala C (2019) Pattern of congenital anomalies in neonates at tertiary care centre in Hyderabad, India: a hospital based prospective observational study. Int J Contemp Pediatr 6(1): 63-67.
-
Ochieng J, Kiryowa H, Munabi I, Ibingira CBR (2011) Prevalence, Nature and characteristics of External Congenital anomalies of Mulago Hospital. East and Central African Journal of Surgery 16(1).
-
Ajao AE, Ikeola AA (2019) Prevalence risk factors and outcome of congenital anomalies among neonatal admissions in OGBOMOSO, Nigeria. BMC Pediatrics 19: 88.
-
Dewangan M, Ali SM, Firdaus U (2016) Pattern of Congenital Anomalies and Risk factors in Newborn in a city of a developing country: An Observational Study. International Journal of Medical pediatrics and Oncology 2(4): 152-155.
-
Westphal F, Fustinoni SM, Pinto VL, Melo PS, Abrahão AR (2016) Association of gestational age with the option of pregnancy termination for fetal abnormalities incompatible with neonatal survival. Einstein (Sao Paulo) 14(3): 311-316.
-
Eluwa MA, Aneosong SA, Akpantah AO, Ekong MB, Asuquo OR, et al. (2013) Congenital Malformations Recorded In four Hospitals In Central Part of Cross River State, Nigeria. International Journal of Pharmaceutical Science Invention 2(10): 27-30.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’