A Study of Comparison of Effectiveness of Letrozole (5mg) Versus Clomiphene Citrate (100 Mg) by Using Injection Human Placental Extract (HPE) for Ovulation Induction among Infertile Women
Aim & Objective: To compare the efficacy of letrozole and clomiphene citrate (CC) by using injection of Human placental extract (HPE) for ovulation induction in infertile women. Introduction: Human placental extract (HPE) is a product of aqueous extraction from the biochemically enriched fresh human placenta which contains nucleotides, amino acids, peptides and vitamins in natural form. It is available as 2 ml ampule. Each ml. is derived from 0.1 gm. of fresh human placenta. Injection of HPE is used in infertility treatment for its anti-inflammatory property, due to which tubal inflammation is decreased and tubal motility increases which is useful for fertility. This is the hypothetical theory behind use of Injection of HPE for infertility treatment in infertile women. Clomiphene citrate has been traditionally used as drug of the choice for treatment of women with infertility. In the last decade, an aromatase inhibitor, letrozole has emerged as an alternative ovulation induction (OI) agent in anovulatory women with polycystic ovarian syndrome. Letrozole has a definitive role in anovulatory women who have not responded to clomiphene citrate therapy and this is confirmed by literatures. Background: Anovulatory dysfunction is a common problem and is responsible for about 40% of female infertility and among causes; PCOS (polycystic ovarian syndrome) is the leading cause. HPE is a product of aqueous extraction from the biochemically enriched fresh human placenta which contains nucleotides, amino acids, peptides and vitamins in natural form. HPE injection- properties: • Specific anti – inflammatory • Tissue repair–wound healing • Immunomodulatory • Melanopoetic • Debridement action It is useful in ovulation induction among infertile women who are infertile due to pelvic inflammatory disease (PID) or due to polycystic ovary syndrome (PCOS) because of its anti-inflammatory property which leads to reduction in tubal inflammation and increased tubal motility. Clomiphene citrate is considered as the first line of treatment for anovulatory dysfunction for a various reason, however Clomiphene citrate has some drawbacks like multi-follicular ovulation and Peripheral anti-estrogenic effect are areas of concern and desire for an effective alternative is need of the hour. An aromatase inhibitor, letrozole, was introduced into infertility practice in the year 2000 and is regarded as a second line option, particularly in women with clomiphene resistance and it has found acceptance in various clinical situations and the indications for its use have expanded. Design: Randomized double blind study. Setting: Scientific Research Institute, Surendranagar, Gujarat, India and a private practice setting. Patients & Methods: The study included 100 women who presented with infertility and were having polycystic ovary syndrome (PCOS). The study participants were divided into 2 groups of 50 each. With these injections, 1 group was given clomiphene citrate (100 mg daily) and another group was given; letrozole (5 mg daily), started from day 3 to day 5 of the menstruation cycle and continued up to 5 consecutive days. Both the groups have received Estradiol Valerate 4 mg. on the 12th day of menstruation until 16th day of menstruation; with visits to determine ovulation and pregnancy, followed by tracking of pregnancies. Selected participants were of age between 20 to 39 years, had normal uterine cavity and had intercourse with male partner with a sperm concentration of at least 14 million per millilitre; and during the study the women and their partners agreed to have regular periodical intercourse with the intent of successful conception. The live birth of baby during the treatment period was the primary outcome. Second Outcome Measures: Follicular growth, endometrial thickness, pregnancy outcome. Results: Women who received Letrozole had more cumulative live births than those women who had received Clomiphene Citrate, (38 out of 50 [76%] vs. 29 out of 50 [58%]) after giving Injection of HPE with these ovulation induction drugs, without significant differences in overall congenital anomalies, with letrozole, as compared to clomiphene, the cumulative ovulation rate was higher. Clomiphene was associated with more numbers of episodes of hot flushes while letrozole was associated with fatigue and dizziness. Rates of other adverse effects were almost similar between these 2 groups. A significant difference in the follicular and endometrial development was evident between these 2 groups. Conclusion: Treatment with Injection of HPE with 2 ovulation induction drugs, Letrozole & Clomiphene Citrate - as compared to clomiphene, letrozole - an aromatase inhibitor, was associated with higher live-birth and ovulation rates in infertile women. The results of the study demonstrated that letrozole is non inferior to clomiphene citrate in the maintenance of endometrial thickness.
Introduction
Millions of women of reproductive age were affected by infertility worldwide. In India among married women the rough prevalence of infertility is 8%. Most of them (5.8%) were secondary infertile [1, 2, 3, 4].
Among infertile women, PCOS (Polycystic ovarian syndrome) has remain the most common female endocrine disorder. Characteristics of PCOS are anovulation, infrequent, irregular or prolonged menstrual periods, clinical or biochemical hyperandrogenism and presence of polycystic ovaries [5]. In the fertile age, it affects 5% to 10% [6, 7], while as per recent studies reporting even higher rates [8]. Ovulation induction is the cornerstone for treatment of women with PCOS suffering from infertility, because about 80% of women with PCOS have anovulation or oligo- ovulation [9].
Human placental extract (HPE) is a product of aqueous extraction from the biochemically enriched fresh human placenta which contains nucleotides, amino acids, peptides and vitamins in natural form.
Each ml of injection contains: 0.1 gm. of fresh healthy human placentae NADPH: not less than 10 µg/ml Total peptides: not less than 90 µg/m Total Nitrogen content: not more than 0.08% w/v Benzyl Alcohol I.P. (As preservative) :1.5% w/v Water for injection IP qs Presence of glutamic acid and Polydeoxyribonucleotides.
It is available as an ampule of 2 ml and of intramuscular usage only.
It is free from HIV antibody, HCV antibody, and hepatitis – B surface antigen.
Human placental extract (HPE) injection has following properties:
- Specific anti – inflammatory
- Tissue repair–wound healing
- Immunomodulatory
- Melanopoetic
- Debridement action The active ingredients of placenta are: DNA, RNA, and nucleotide, amino acids – Glutamate, tyrosine & tryptophan, vitamins - in natural form, minerals, and peptides.
It is useful in following conditions by its anti- inflammatory property:
- Pelvic inflammatory disease (PID)
- Polycystic ovary syndrome (PCOS) This is the hypothetical theory - due to its anti- inflammatory property it reduces tubal inflammation and increases tubal motility which leads to increase in good pregnancy outcome [10].
Clomiphene citrate (CC) belongs to a selective estrogen receptor modulator drug classification, has traditionally been used as the drug of first-choice for ovulation induction or superovulation in women with PCOS [11]. Mechanism of action of CC is depicted in Figure 1. CC has an anti-estrogenic effect, which results in estrogen receptor (ER) deletion, and has long half-life; therefore, it accumulates in the body causing long lasting ER depletion [12].CC lasts for a long time in the body and may be due to this it has an adverse effect on cervical mucus and uterine lining, such as endometrial proliferation leading to thinning of endometrium. The endometrial thickness is one of the significant parameters affecting pregnancy. The pregnancy rate can be very low, if endometrial thickness is less than 6-8 mm [13]. Clomiphene citrate is one of the treatment modalities which reduce endometrial thickness [14], so we should adjust endometrial thickness and proliferation during induction of ovulation to avoid this.
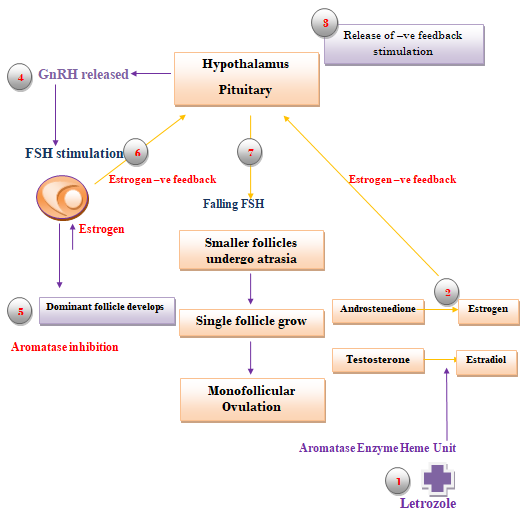
Letrozole is an aromatase inhibitor, has also been recommended as a first-line drug therapy for improvement of the fertility outcomes in women with PCOS [15, 16]. Aromatase - an enzyme responsible for the production of estrogen in human body. Letrozole works by inhibiting aromatase by completely binding to it, which results in a reduction of estrogen biosynthesis in all the tissues [1]. Mechanism of action of the letrozole is depicted in figure-2. It has a short half-life, thereby it rapidly eliminated from body within 42 hours, with less risk of ovarian hyperstimulation [17]. The mechanism of clomiphene citrate is to block estrogen receptors and produce more of hormones from pituitary gland which are required to stimulate the ovaries. FSH and LH, these hormones can cause the development of ovulation in women who are anovulatory or increase the number of eggs developing in ovaries of women who already ovulate [18]. The endometrial response of Letrozole while being compared to clomiphene citrate is significantly better.
Drugs like Letrozole and clomiphene citrate are used for inducing ovum and to release ovum in women who are not ovulating on their own. This is known as ovulation induction. In super ovulation, these drugs can be used to increase the chances of pregnancy in women who are already ovulating. As per study done by Wang et al., the network meta-analysis showed that letrozole is the only treatment showing a significant higher rate of live birth, as compared with CC alone [19]. Although multi-follicular growth can be aim in women with an unexplained infertility while stimulating ovary but in women with an anovulation who are undergoing for ovulation induction, mono-follicular growth can suffice the purpose [15]. In order to study the efficacy and safety of different ovulation induction protocols with minimum of side effects and higher pregnancy rates in women with PCOS treated with clomiphene citrate and letrozole to assess the mono- versus multi- follicular growth, we compared the successful live pregnancy rates among women with who had ovulation induction with CC and letrozole at a Scientific Research Institute, Surendranagar, Gujarat, India.
Here are some recommendations of different societies for letrozole as a 1st line treatment option in ovulation induction: As per American College of Obstetrics and Gynaecologists [20] (2016) society, letrozole should be considered as 1st line therapy for OI in patients with PCOS and BMI >30 because of increased live birth rate (LBR) compared to clomiphene citrate; as per Australian National Health and Medical Research Council (NHMRC) guidelines [21] (2015), letrozole, under caution, could be offered as pharmacological treatment for OI indicated for infertile anovulatory women with PCOS with no other infertility factors.
![Figure 1: CC has an anti-estrogenic effect, which results in estrogen receptor (ER) deletion, and has long half-life; therefore, it accumulates in the body causing long lasting ER depletion [12].CC lasts for a long time in the body and may be due to this it has an adverse effect on cervical mucus and uterine lining, such as endometrial proliferation leading to thinning of endometrium. The endometrial thickness is one of the significant parameters affecting pregnancy. The pregnancy rate can be very low, if endometrial thickness is less than 6-8 mm [13]. Clomiphene citrate is one of the treatment modalities which reduce endometrial thickness [14], so we should adjust endometrial thickness and proliferation during induction of ovulation to avoid this.](/fulltextimages/8540/fig_1.png)
Methodology
Study Oversight
The rationale for trial and a detailed protocol summary of study participants, as well as study methods and the full baseline characteristics of the study participants has been discussed earlier. We used here injection of HPE with 2 ovulation induction drugs- clomiphene citrate and letrozole for treatment of infertile women to get good pregnancy outcome. The Enrolment of study participants was started in October 2019 and completed in October 2021. All the data entry, data management, and analyses were performed at the Scientific Research Institute, Surendranagar, and Gujarat, India.
Patients
A total of 100 women with the problem of infertility, of having age in a range of 20 to 39 years, who had no major medical problems and who were not taking confounding medications as described in study protocol (other fertility drugs, sex steroids, insulin sensitizers), their male partners, and their neonates were also part of the study. Additional eligibility criteria included a normal uterine cavity, or evidence of an intrauterine pregnancy within previous 3 years; a male partner with a sperm concentration of at least 14 million/millilitre, as per WHO cut-off points criteria with the documented motility, with at least one ejaculation episode during the previous year and a commitment on the part of women as well as their partners to have a regular intercourse during the study with the purpose of pregnancy.
Exclusion Criteria
• Patients with hyperprolactinemia
• Thyroid disorder
• Male factor infertility
Study Overview
Total 100 women were randomly assigned and given injection of HPE (2 ml) 1 ampule IM started from day 3 to 5 of menstrual cycles on alternate day until total 10 injections’ course completed and they were divided into 2 groups of 50 in each group. 1st group was given clomiphene citrate (100 mg daily) and 2nd group was given; letrozole (5 mg daily), started from any day between 3 to 5 of the menstrual cycle and continued up to 5 consecutive days (Table 1).
This is followed by giving Estradiol Valerate 4 mg on the 12th day of menstruation until 16th day of menstruation in both groups. Couples were instructed to have a regular intercourse under ultrasound guidance for peri- follicular flow and endometrial vascularity with confirmation of rupture of follicles. Participants who successfully conceived were taken a follow up until a viable intrauterine pregnancy was observed (on ultrasonography- fetal heart motion visualized) and prenatal care given to them. The outcome of the study was tracked through the review of maternal and infant medical records.
- Letrozole with HPE injection group
- Clomiphene citrate with HPE injection group
- The patients were given HPE Injection (2 ml) 1 ampule IM started from day 3 to 5 of menstrual cycles on alternate day until total 10 injections’ course completed; they were orally administered 5.0 mg/day Letrozole starting between the
- 3rd to 5th days of menstrual cycle for five consecutive days.
Table 1: Treatment methods in study group.
Outcomes
The live birth of baby during the treatment period was the primary outcome; secondary outcomes which included were ovulation, pregnancy loss, singleton birth, and congenital anomalies. The follicular development, growth and endometrial thickness were also calculated to see difference between the 2 groups.
Results
Characteristics of the Patients
A total of 100 women who have problem of infertility were randomly assigned to treatment group and they were divided into 2 groups; both the groups were well matched at baseline. Study participants are having age range between 20-39 years. Study was begun in October 2019 with 1st patient recruitment and was completed in October 2021 with last patients out.
Live Births and Secondary Outcomes
Women who received letrozole, as compared to those who received clomiphene citrate, had more cumulative live births when given along HPE injection IM 1 ampule on alternate day, total 10 injections were given ((38 out of 50 [76%] vs. 29
out of 50 [58%]) (Table 2). The successful ovulation (%) was significantly higher with letrozole compared to clomiphene citrate. Among the study participants who ovulated, there was a Lower multiple pregnancy rate with letrozole compared to clomiphene citrate.
| Parameters | Letrozole 5 mg | Clomiphene citrate 100 mg |
|---|---|---|
| No. of patients | 50 | 50 |
| Women who ovulated- number (%) | 46 (92%) | 40 (80%) |
| Live birth- number/total number (%) | 38/50 (76%) | 29/50 (58%) |
| Conception- number of women (%) | 38(76%) | 29 (58%) |
Table 2: Outcomes regarding the ovulations, live birth and pregnancy.
In letrozole group, the mean number of dominant follicles (≥18 mm) was 1.4±0.58 while in clomiphene citrate group it was 1.1±0.86 (P-value= <0.05). The significant difference in the follicular and endometrial development was evident between letrozole and clomiphene citrate treated cycles (Table 3).
| Parameters | Letrozole 5 mg | Clomiphene citrate 100 mg | P value |
|---|---|---|---|
| Number of follicles ≥ 18 mm | 1.4±0.58 | 1.1±0.86 | P<0.05 |
| Size of follicular development by day 14 (mm) | 17.6±2.92 | 15.8±3.84 | P<0.05 |
| Endometrial development by day 14 (mm) | 7.2±0.77 | 6.8±0.92 | P<0.05 |
| Pregnancy (among ovulated patients) | 38/50 | 29/50 | - |
Table 3: Ovulation induction outcomes of letrozole and clomiphene citrate groups.
The live birth rates after cycles induced with clomiphene citrate and letrozole were 58%, 76% respectively after using these ovulation induction drugs with HPE. Multiple pregnancies were recorded in 2 women who had given clomiphene citrate. Out of them1 woman had twin pregnancy and another woman had triplet pregnancy; both women have delivered full term and healthy babies; there were no maternal or neonatal complications present.
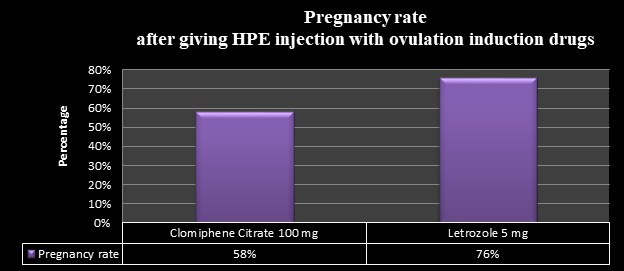
Figure 3: Pregnancy outcomes and gestation rates with 2 ovarian stimulation treatment methods with addition of HPE extract. Adverse Effects and Pregnancy and Neonatal Complications There were no side effects noted with Injection of HPE. During infertility treatment, two adverse events related The number of patients reporting side effects who had given letrozole were 3 and who had given clomiphene citrate were 6.
The most common neonatal complications which noted were jaundice, respiratory distress, a condition requiring hospitalization for more than 3 days, and intrauterine growth restriction, with not much of significant differences between treatment groups.
The endometrial thickness was higher with letrozole when compared to clomiphene citrate. The comparison of ovulation induction among clomiphene citrate and letrozole is given below:
| Ovulation induction with Clomiphene citrate(CC) [22,23,24] | Ovulation induction with Letrozole [22,23,24] |
|---|---|
| Multi-follicular ovulation | Mono-follicular ovulation |
| Peripheral anti-estrogenic effect | No anti-estrogenic effect |
| Causes endometrial thinning | Better endometrial thickness |
| Thick cervical mucus | Better cervical mucus quality |
| Longer half-life of 5-7 days | Shorter half-life of 45 hours |
| Higher miscarriage rate | Improved implantation |
| Higher multiple pregnancy rate | Lower multiple pregnancy rate |
| High rates of resistance in PCOS | Effective in CC-resistant PCOS |
| Lower live birth rate | High live birth rate |
Discussion
In our knowledge, this is first of its kind publication pertaining to role of human placental extract (HPE) in improving birth outcome and in treatment of infertility but here we used it with 2 ovulation induction drugs- clomiphene citrate and letrozole and got good pregnancy outcome. Placenta extract has anti-inflammatory property, using which it reduces tubal inflammation, increases tubal motility, cures pelvic inflammatory disease, reduces ovarian cysts formations and thereby helpful in infertility treatment.
For many years, clomiphene citrate has remained as the first line therapy in women with infertility for ovulation induction. Historically, Clomiphene citrate having classical antiestrogenic effect as it induces prolonged estrogen receptors depletion with an estrogen target tissues especially in endometrium. Several studies showed that with clomiphene there can be deleterious effect on endometrial development resulting in endometrial thin layer, luteal phase effect, decreased uterine flow, and failure to implantation. So, we added Estradiol Valerate 4 mg on the 12th day of menstruation until 16th day of menstruation per oral to prevent detrimental effects of clomiphene on the endometrium.
As per the study outcome endometrial thickness was higher in letrozole group than clomiphene group. This is also supported by previous studies carried by Hendawy et al. [24] in which they compared the effects of letrozole and clomiphene citrate on ovulation induction and the result was in favour of letrozole as it had a better effect on endometrial thickness and pregnancy rate than clomiphene citrate. Mitwally and Casper found that letrozole was associated with greater endometrial thickness [17] when they give aromatase inhibitor (letrozole) to patients with anovulatory infertility; all of them had previously received clomiphene with an inadequate outcome.
As per our study it’s been found that letrozole was non inferior drug as a fertility treatment than clomiphene citrate in women with both of the problems of infertility and polycystic ovary syndrome. These factors were significantly more likely occur in letrozole group as compared with clomiphene citrate group: ovulation, conception, pregnancy, and live birth. The mean duration of pregnancy, birth weight, and rates of neonatal complications did not differ significantly between two treatment groups. Although multiple pregnancy (twins, triplets) rate noted with clomiphene citrate group was higher.
Although no FDA approved as a fertility medication, letrozole is one of the first choices for fertility treatment. The successful live-birth rate was higher with letrozole than with clomiphene citrate among women with infertility and polycystic ovary syndrome in our study. In our study we have applied protocol of adding Human placental extract (HPE) injection in both arm due to its anti-inflammatory, immunomodulatory and debridement action but there is scarcity of direct evidence of its role in ovulation induction among infertile women.
Conclusion
Injection of Human placental extract (HPE) used with 2 ovulation induction drugs-clomiphene citrate and letrozole for treatment of infertility. It acts by its anti- inflammatory property and helps in reducing formation of polycystic ovaries, reduces tubal inflammation, treats pelvic inflammatory disease (PID) and gives good pregnancy outcome.
Letrozole- an aromatase inhibitor was associated with higher live-birth and ovulation rates among infertile women as compared to clomiphene. The results of the study have demonstrated that letrozole is non inferior to clomiphene citrate in the maintenance of endometrial thickness.
Clomiphene citrate has some limitations; including its overall poor efficacy (56% rate of live birth), a comparatively high multiple pregnancy rate, and side effect profile which includes mood changes and hot flushes. The important objective and public health goal is to develop the effective, simple yet safe treatments modality for infertility.
Letrozole-an aromatase inhibitor, which blocks estrogen synthesis, can directly affect hypothalamic-pituitary- ovarian-uterine function and theoretically might increase chances of pregnancy rates. Potential advantages of letrozole when being compared to clomiphene citrate include a more physiological hormonal stimulation of endometrium, a lower chances of multiple pregnancy rate through single-follicle recruitment, lesser vasomotor and mood symptoms, and rapid clearance, thus reducing chances of exposure in period of periconception.
References
-
Mitwally MF, Casper RF (2001) Use of an aromatase inhibitor for induction of ovulation in patients with an inadequate response to clomiphene citrate. Fertil Steril 75(2): 305-309.
-
Al Omari WR, Sulaiman W, Al Hadithi N (2004) Comparison of two aromatase inhibitors in women with Clomiphene resistant polycystic ovary syndrome. Int J Gynecol Obstet 85(3): 289-291.
-
Azim A, Oktay K (2007) Letrozole for ovulation induction and fertility preservation by embryo cryopreservation in young women with endometrial carcinoma. Fertil Steril 88(3): 657-664.
-
Goswami SK, Das T, Chattopadhyay R, Sawney V, Kumar J, et al. (2004) A randomised single- blind controlled trial of letrozole as a low-cost IVF protocol in women with poor ovarian response: a preliminary report. Hum Reprod 19(9): 2031-2035.
-
Fauser B, Tarlatzis B, Chang J, Azziz R, Legro R, et al. (2003)The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group; (2004) Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 81(1): 19-25.
-
Asunción M, Calvo RM, San Millan JL, Sancho J, Avila S, et al. (2000) A prospective study of the prevalence of the prevalence of the polycystic ovary syndrome in unselected Caucasian women from Spain. J Clin Endocrinol Metab 85(7): 2434-2438.
-
Li R, Zhang Q, Yang D, Li S, Lu S, et al. (2013) Prevalence of polycystic ovary syndrome in women in China: a large community-based study. Hum Reprod 28(9): 2562-2569.
-
Copp T, Jansen J, Doust J, Mol BW, Dokras A, et al. (2017) Are expanding disease definitions unnecessarily labelling women with polycystic ovary syndrome? BMJ 358: j3694.
-
Kousta E, White D, Franks S (1997) Modern use of clomiphene citrate in induction of ovulation. Hum Reprod Update 3(4): 359-365.
-
Fauser BC, Tarlatzis BC, Rebar RW, Legro RS, Balen AH, et al. (2012) Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil Steril 97(1): 28-38.e25.
-
Mikkelson TJ, Kroboth PD, Cameron WJ, Dittert LW, Chungi V, et al. (1986) Single-dose pharmacokinetics of clomiphene citrate in normal volunteers. Fertil Steril 46(3): 392-396.
-
Cetinkaya K, Kadanali S (2012) The effect of administering vaginal estrogen to clomiphene citrate stimulated cycles on endometrial thickness and pregnancy rates in unexplained infertility. J Turkis German Gynaecol Assosc 13(3): 157-161.
-
Nakamra Y, Ono M, Yoshida Y, Sugino N, Ueda K, et al. (1997) Effects of Clomiphene citrate on the endometrial thickness and echogenic pattern of the endometrium. Fertil. Steril 67(2): 256-260.
-
Legro RS, Brzyski RG, Diamond MP, Coutifaris C, Schlaff WD, et al. (2014) Letrozole versus clomiphene for infertility in polycystic ovary syndrome. N Engl J Med 371(2): 119-129.
-
Balen AH, Morley LC, Misso M, Fraks S, Legro RS, et al. (2016) The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update 22(6): 687-708.
-
Dowset M (1999) Drug and hormone interactions of aromatase inhibitors. Endocr Rel Cancer 6(2): 181-185.
-
Randy Morris (2009) Letrozole Co-treatment not better for Infertile Women Over 40.
-
Birch Petersen K, Pedersen NG, Pedersen AT, Lauritsen MP, la Cour Freiesleben N (2016) Mono-ovulation in women with polycystic ovary syndrome: a clinical review on ovulation induction. Reprod Biomed Online 32(6): 563-583.
-
Wang R, Kim BV, van Wely M, Johnson NP, Costello MF, et al. (2017) Treatment strategies for women with WHO group 2 anovulation: systemic review and network meta-analysis. BMJ 356: j138.
-
ACOG (2016) Committee Opinion No. 663: Aromatase Inhibitors in Gynecologic Practice. Obstet Gynecol 127: 170-174.
-
(2015) Australian National Health and Medical Research Council (NHMRC) guideline.
-
Mitwally MF, Casper RF (2006) Review: aromatase inhibitors for ovulation induction. J Clin Endocrinol Metab 91(3): 760-771.
-
Sunita S, Sanghamitra G, Soma S, Astha C, Ashalatha G, et al. (2014) Congenital malformations among babies born following letrozole or clomiphene for infertility treatment. PLoS One 9(10): e108219.
-
Hendawy SF, Samaha HE, Elkholy MF (2011) Letrozole versus clomiphene citrate for induction of ovulation in patients with polycystic ovarian syndrome undergoing intrauterine insemination. Clin Med Insights Reprod Health 5: 11-6.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’