Assessment of Antibiotic Administration and its Interaction with other Biological Factors during Pregnancy among Pregnant Women in Sudan
Objective: The objective of this study was to provide information on the prevalence of use of antibiotics to Sudanese pregnant women, some of which may have feto-toxic or teratogenic effects, in the outpatient setting. Materials and Methods: This was a descriptive retrospective cross sectional hospital based study, which carried out in Military Hospitals and Khartoum Teaching Hospital (Sudan) from Jan. 2014 to Jan. 2015. Data collection was used to extract the information from 650 pregnant patient’s files. The information recorded included: age, trimester, medical history and administered antibiotic. Data was analyzed using SPSS16 software on the Microsoft Windows 7 Professional Operating System, with p <0.05 considered statically significant, using Chi square test. Results: About 76% of women (N = 494) were dispensed an antibiotic medications and the consumption was significantly higher in the second trimester (4-6 months) 41.5% of women (N = 205) than first trimester (1-3 months) 33.2% of women (N = 164) and third trimester (7-9 months) 25.3% of women (N = 125). The most common antibiotic dispensed during pregnancy were Amoxicillin (No=182; 28%), Cephalexin (No=148; 22.7%), Cefixime (No= 37; 5.7%), Erythromcin (No=29; 4.46%), Cefopodoxim (No= 28; 4.3%), Benzyl penicillin (No= 27; 4.15%), Clotrimazole-V (No= 22; 3.38%), Clotrimazole+betamethazone (No= 16; 2.46%) and Metronidazole (No= 5; 0.77%). Amoxicillin is the most commonly dispensed antibiotic in the third trimester (7-9 months) No= 47, Cephalaxin is the most commonly dispensed antibiotic drugs in the second trimester (4-6 months) No= 84 and Metronidazole is used by three pregnant women during second trimester. In hypertensive and diabetic pregnant women, the most common used drug is Amoxicillin and Cephalexin. Conclusions: Antibiotics are highly prescribed to pregnant Sudanese women. The prevalence of usage of antibiotics that are suspected to be feto-toxic or teratogenic especially in first trimester (Metronidazole) was low in this cohort of pregnant women. The prescription of drugs during pregnancy must be evaluated carefully, weighing the risks versus benefits for both fetus and mother. Antibiotics with possible toxic potential should therefore be prescribed by the physician and checked by clinical pharmacists only if the infectious disease is life-threatening and there is no other choice for its treatment.
Introduction
The usage of antimicrobials has increased steadily since the discovery of penicillin. Numerous drugs have been developed since then, few of which were considered potentially toxic [1, 2, 3]. In the twenty-first century, serious infectious diseases have developed resistance to routinely used antibiotics and have become a major worldwide healthcare issue, which are not only more severe, but they are also costlier to detect and cure [4]. Moreover, antibiotic development is slowing down. When compared to the era (1983–1987), the approval of novel antibacterial medicines by the US Food and Drug Administration (FDA) dropped by 56% from 1998 to 2002. As a result, unless alternative antimicrobials are developed, such as the use of natural molecules high in antimicrobials, the supply of new effective antibiotics is anticipated to decrease in the future [5]. Interest in studies of the teratogenic effects of drugs during pregnancy has increased since 1961, when the high incidence of phocomelia among patients treated with thalidomide was discovered [6] although teratogenicity has long been known, pregnant women are still exposed to this risk [3]. Previous studies have found that 99% of pregnant women were prescribed at least one drug during pregnancy. The average consumption of drugs, excluding vitamins and supplements, is estimated to be 1.3 drugs per woman [6, 7].
Considering carefully the advantages and the possible damage related to drug usage, antibiotics in particular well illustrate the situation of the prescriber First we should remember the frequency of anomalies of the fetus. The frequency of idiopathic or spontaneous malformations of the fetus amounts to 2%. About 30% of all observed congenital malformations are related to chromosomal anomalies etc., and the frequency of other (often unknown) related factors, e.g. drugs, is as high as about 60% [8]. Among the antibiotics, only a few classes of compounds have been convincingly shown to be completely harmless when used during pregnancy. However, our knowledge of most antibiotics is limited, as can be seen from the warnings of antibiotic manufacturers not to administer that particular drug during pregnancy, especially in the first trimester. It is now evident that any substance present in the maternal blood should be able to cross the placenta to an extent which is dependent on drug metabolism or other factors such as concentration gradients, lipophilicity, molecular size and binding effects etc. However, as mentioned above, the currently available information on the pharmacokinetics of many antibiotics in the maternal fetal unit is fragmentary [9]. Therefore, this study aimed to provide information on the prevalence of usage of antimicrobial medications, some of which may have fetotoxic or teratogenic effects, in the outpatient setting among pregnant women at Military Hospitals and Khartoum Teaching Hospital (Sudan).
Materials and Methods
This is a descriptive retrospective cross sectional hospital based study which carried out in military hospitals from Jan 2014- Jan 2015. Data collection form was used to extract the information from pregnant patient’s files. The information records included: age, trimester, medical history, hemoglobin values and antibiotic administered.
Study Design
Up to 650 patient’s files of pregnant women were included in this study, the target age was from 15 to 45 years old from the Hospital-goers in Military Hospitals and Khartoum Teaching Hospital (Sudan) from Jan. 2014 to Jan. 2015.
Ethical Approval
Ethical approval was obtained after the research protocol was checked by the Institutional Review Board (IRB) at the department of Clinical Pharmacy and Pharmacy Practice - Karary University, Sudan, following the Helsinki Declaration principles, before data collection. Information that identifies patients have been removed or pseudonymised.
Statistical Analysis
Data was analyzed using SPSS16 software on the Microsoft Windows 7 Professional Operating System, with p <0.05 considered statically significant, using Chi square test.
Results
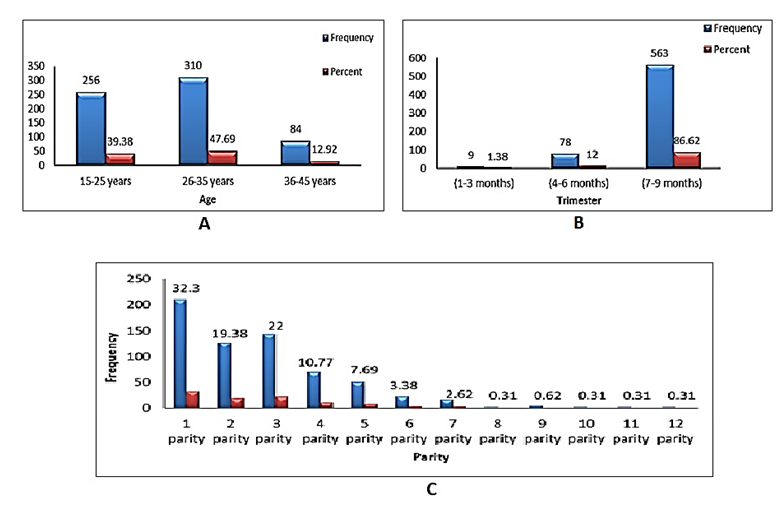
Figure 1, represents some biological factors during pregnancy among pregnant women in Sudan (age, trimester and parity). Results revealed that, of a total of 650 pregnant women included in this study we found that the age of 256 patients (39.38%) was between (15-25 years), 310 patients (47.7%) was between (26-35 years) and 84 patients (13%) was between (36-45 years). The trimester bar-wise, 9 (1.38%) were in the first trimester (1-3 months), 78 (12%) were in the second trimester (4-6 months) and 563 (86.62%) were in third trimester (7-9 months). Regarding parity, the primigravida were 210 (32%) while multigravida was 440 (67.7%).
Regarding Maternal Disorders, one hundred and fifty- four (23.7%) of the pregnant women had maternal disorders, however, most of them 15(2.3%) had hypertension during pregnancy; this is shown in (Table 1).
| Maternal Disorders | Frequency | Percent |
|---|---|---|
| Multiple pregnancy | 2 | 0.3 |
| Gastric hyperacidity | 4 | 0.7 |
| Nausea | 2 | 0.3 |
| Nausea+vomiting | 4 | 0.7 |
| Cough | 2 | 0.3 |
| Cough+ fever | 2 | 0.3 |
| Asthma | 4 | 0.7 |
| Pernicious anaemia | 2 | 0.3 |
| Venous thromboembolism | 7 | 1 |
| Pneumonia | 11 | 1.7 |
| Severe pneumonia | 2 | 0.3 |
| Heamophilus influenzea | 5 | 0.7 |
| UTI | 15 | 2.3 |
| Pneumonia+ Gastric hyperacidity | 2 | 0.3 |
| Pneumonia+ UTI | 2 | 0.3 |
| Superficial Fungal Infection | 2 | 0.3 |
| Superficial Fungal Infection+ Pneumonia+Amoebiasis | 2 | 0.3 |
| Hypertension | 15 | 2.3 |
| Hypertension during pregnancy | 22 | 3.3 |
| Diabetic | 5 | 0.7 |
| Diabetic during pregnancy | 11 | 1.7 |
| Severee pneumonia+ Diabetic | 2 | 0.3 |
| Congenital adrenal hyperplasia | 5 | 0.7 |
| Severee anaphylactic shock | 5 | 0.7 |
| Congenital hyperadrenalism | 2 | 0.3 |
| Brain cancer | 2 | 0.3 |
| Chorea disease | 2 | 0.3 |
| Hypothyroidism | 2 | 0.3 |
| Anemia | 11 | 1.7 |
| Total | 154 | 23.7 |
| Missing system | 496 | 76.3 |
| Total | 650 | 100 |
Table 1: Study of Maternal Disorders.
Figure 2, showed the administered antibiotics to pregnant women and trimester versus antibiotics. Regarding showed the administered antibiotics, four hundred and ninety-four of pregnant women (76%) were on an antibiotic drug. Regarding trimester versus antibiotics, there were
164 (33.2) of pregnant women in the first trimester (1-3 months), 205(41.5%) in the second trimester (4-6 months), 125 (25.3%) in the third trimester (7-9 months) had received antibiotics and it was significant with p<0.0001 at 95% confidence (0.000-0.01)
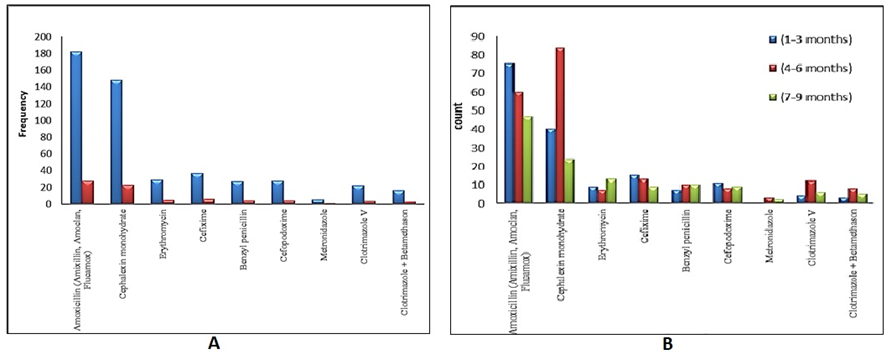
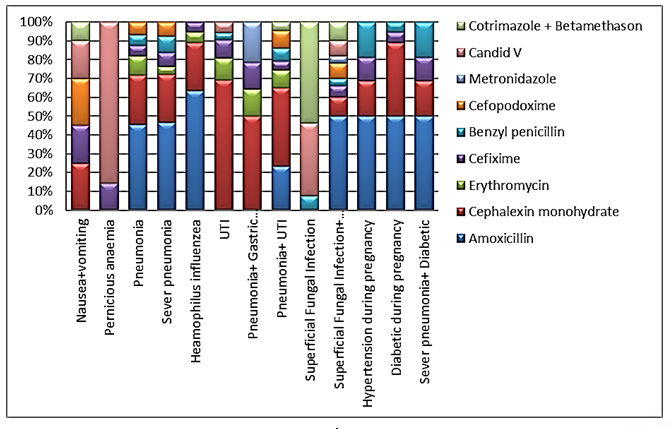
Figure 3, demonstrates the maternal Disorders versus antibiotics, there were 494(76%) of the pregnant women had received antibiotics for their maternal disorders, which was significant with p<0.0001 at 95% confidence (0.000- 0.01).
Discussion
Based on the findings of this study, up to 76% of women were dispensed an antibiotic medications and the consumption was significantly higher in the second trimester (4-6 months) 41.5% of women than first trimester (1-3 months) 33.2% of women and third trimester (7-9 months) 25.3% of women. Previous studies reported that antibiotics are often extensively used during pregnancy, accounting for over 80% of all prescription medicines, and around 20–25% of women taken antibiotics throughout their pregnancy [10, 11]. Antibiotics have a number of physiological concerns, therefore their use during pregnancy requires careful consideration and a discussion of the risks against benefits to the mother in the short and long term is necessary [12]. Our study also revealed that, the most common antibiotic dispensed during pregnancy were Amoxicillin, Cephalexin, Cefixime, Erythromcin, Cefopodoxim, Benzyl penicillin, Clotrimazole-V, Clotrimazole+betamethazone and Metronidazole, respectively. It is obviously here that; antibiotics are extensively prescribed for Sudanese pregnant women. This is a serious situation, when compare it with the status of pregnant women in some developed countries; In the Netherlands, only one in five women was prescribed at least one antibiotic during pregnancy, this ration is acceptable and in accordance with European health recommendations [13]. In UK, during pregnancy, only one-third of pregnant women received at least one antibiotic prescription. At least one antibiotic was given to only 14 percent of women in each trimester [14].
Some of the frequently prescribed antibiotics will be distributed below into three groups according to their rational use during pregnancy: 1. Antibiotics belonging to the first group: which should not be administered to pregnant women (e.g. Aminoglycoside, Antimycotics, 5-nitroimidazoles, Polymyxin, Tetracyclines and Vancomycins) [7]. The 5-nitroimidazoles are generally well tolerated. The warnings with respect to administration during pregnancy are the results of increased mutation rates found in vitro in bacteria [15]. Of twenty-six reports that examined a total of 1,323 pregnant women, only four found evidence of congenital anomalies in infants exposed to metronidazole during the first trimester. Among these four studies, no consistent pattern of congenital malformations is found. Furthermore, previous studies found congenital malformations including coronal hypospadius, syndactyly, calcaneous valgus, hydrocele, and pyloric stenosis, which may not necessarily be related to the first trimester. Given the limited information available, and no conclusive human studies, there is probably no increased risk of birth defects due to exposure to metronidazole during pregnancy [2, 8, 15]. In this study metronidazole is used by 3 pregnant women during second trimester and 2
during third trimester. Vancomycin: is a glycopeptide antibiotic used in the prophylaxis and treatment of infections caused by Gram-positive bacteria and MRSA infections (e.g. staphylococcus species, staphylococcus endocarditis, pseudomembranous colitis etc…). Used only after treatment with other antibiotics had failed. Common (adverse drug reactions) include: local pain, which may be severe and/or thrombophlebitis ,anaphylaxis, toxic epidermal necrolysis, erythema multiforme, red man syndrome, super infection, thrombocytopenia, leucopenia, tinnitus, dizziness and/ or ototoxicity [1, 2, 6]. 2. Antibiotics belonging to the second group: which are to be used only at certain stages of pregnancy (e.g. Trimethoprim, Pyrimethamine, Chloramphenicol, Rifampicin and Sulphonamide) 3. Antibiotics belonging to the third group: In contrast to the antibiotics listed above, which should be excluded from therapy during pregnancy or at certain stages of pregnancy, this group of antibiotics (Penicillin, Cephalosporin, Erythromycin and Lincomycin) could be administered at any time [15].
Penicillins are bactericides that belong to the betalactamic group. Their mechanism of activity is based on the inhibition of bacterial cell wall synthesis through inactivation of the transpeptidase enzyme [16]. It must be noted that all penicillins may produce anaphylaxis during pregnancy or immediately after delivery. If anaphylaxis is severee and uncontrolled, it could result in compromising placental circulation, and cause fetal damage or death. Betalactamase- resistant penicillin: oxacillin, cloxacillin, methicillin; and aminopenicillin: ampicillin, amoxicillin [17, 18]. With regard to their activity spectrum, they generally act on Gram-positive rods. Oxacillin, methicillin and dicloxacin, and also larger spectrum penicillin (such as amoxicillin associated with clavulanic acid and ampicillin associated with sulbactam) are effective on Gram-negative microorganisms [16, 17, 18, 19]. Undoubtedly this antimicrobial drug (penicillin) is the most indicated for pregnant women, since it has highly selective toxicity [15, 18]. Penicillin can be described as safe and is classified as category B by the FDA. Few side effects are described, and the most important reactions are gastrointestinal disorders and hypersensitivity [20]. The occurrence of hypersensitivity reactions may vary from 1% to 10% of patients and may be fatal for 0.02% of cases. Acute reactions occur after 22 minutes following intake, and are characterized by urticaria, angiodema, bronchospasm, hypotension or anaphylactic shock. Immediate reactions occur between 30 minutes and 48 hours after penicillin intake and are represented by urticaria, angiodema, bronchospasm, wheezing and local inflammation. Late reactions occur after 72 hours of penicillin intake, with characteristic symptoms:
skin reactions, exfoliative dermatitis, serious stomatitis and acute glossitis [20, 21]. In this study, amoxicillin was the common used drug (No=182; 28%) among pregnant women especially in the third trimester to treat severe pneumonia, Heamophilus influenzea and Superficial Fungal Infection.
Cephalosporins: These drugs also belong to the betalactamic group and show similar activity and resistance mechanisms as those of the penicillin’s. They are subdivided into generations: First generation: cefazolin, cefalexin, cefadroxil, and cefradine; Second generation: cefuroxime, cefprozile, and cefmetazol; Third generation: cefotaxime, cefdinir, ceftriaxone, cefoperazone and ceftazidime; fourth generation: cefepime, and cefpiroma [21]. Ceftriaxone is a third-generation cephalosporin antibiotic. It is indicated for septicemia, pneumonia, surgical prophylaxis, meningitis and many more. Adverse effects include: diarrhea, nausea, rash, electrolyte disturbances, hepatoxcity and/or pain and inflammation at injection site. Infrequent ADRs include: vomiting, headache, dizziness, oral and vaginal candidiasis, pseudomembranous colitis, super infection, eosinophilia, and/or fever [19]. The cephalosporins, in addition to penicillin, are one of the antimicrobial drugs most frequently indicated during pregnancy and are classified as category B by the FDA [16, 18]. Like penicillin, cephalosporins show low occurrence of adverse reactions, except for hypersensitivity, which affects 10% of patients with hypersensitivity to penicillin due to cross-hypersensitivity [1, 2, 15]. In this study, Cephalexin was used in (No=148; 22.7%), Cefixime (No= 37; 5.7%), Cefopodoxim (No= 28; 4.3%) pregnant women especially in the third trimester to treat Pneumonia, Pernicious anaemia and urinary tract infections.
Macrolides: Erythromycin, clarithromycin, roxithromycin, and azithromycin are macrolides that interfere with the bacterial synthesis of leucine, by their action on 50S subunits of ribosomes, inhibiting the translocation of t-RNA [22]. They are bacteriostatic, but may be bactericide, depending on the microbial species and inoculums microorganisms involved in the infectious process, as well as the drug concentration in the infected area [23]. They show similar spectrum of activity as that of penicillin. They are effective against Gram-positive, anaerobic and a wide spectrum of Gram-negative microorganisms. Their toxicity is low due to the absence of subunit 50S in human cells. However, erythromycin may cause cholestatic hepatitis, general hepatoxicity and gastrointestinal alterations, mainly in estolate form. The FDA classifies erythromycin as category B and the base form considered the best form for use during pregnancy. Erythromycin in our study was used in (No=29; 4.46%) pregnant women only in third trimester to treat Pneumonia and urinary tract infections in penicillin sensitive woman.
Meropenem is an ultra-broad spectrum injectable antibiotic used to treat a wide variety of infections, including meningitis, pneumonia, intra-abdominal infections etc. The most common adverse effects are diarrhea, nausea vomiting, headache, rash, thrombophlebitis, hypokalaemia, apnea, sepsis, septic shock .It is unlike penicillin, cephalosporins, it shows high occurrence of adverse reactions. The FDA classifies Meropenem as category B for use during pregnancy [13]. As a general principle, pregnant women should try to avoid taking medications, but if an antibiotic must have prescribed, the physician should choose one from the third group of antibiotics (e.g. Penicillin, Cephalosporin, Erythromycin and Lincomycin); because it could be administered at any time and it has the minor harmful adverse effects. In hypertensive and diabetic pregnant women, the most common used drug was amoxicillin but benzyl penicillin used in severe pneumonia diabetic’s woman.
Conclusion
The prevalence of usage of antimicrobial drugs that are suspected to be fetotoxic or teratogenic especially in first trimester (Metronidazole) was low in this cohort of pregnant women. As a general principle, pregnant women should try to avoid taking medications, but if an antibiotic must have prescribed, the physician should choose one from the third group of antibiotics (e.g. Penicillin, Cephalosporin, Erythromycin and Lincomycin); because it could be administered at any time and it has the minor harmful adverse effects. The prescription of drugs during pregnancy must be evaluated carefully, weighing the risks versus benefits for both fetus and mother. Antimicrobial drugs with toxic potential should therefore be prescribed by the physician and checked by clinical pharmacist if the infectious disease / patient’s condition is life-threatening and there is no other choice for its treatment to avoid drug related problems (DRPs).
References
-
Kimble MAK, Young LY, Alldredge BK, Kradjan WA, Corelli RL, et al. (2009) Applied Therapeutics. The Clinical Use of Drugs. 9th (Edn.), Lippincott Williams & Wilkins Press, US.
-
Malone PM, Malone MJ, Park SK (2016) Drug Information: A Guide for Pharmacists 6th(Edn.), Access Pharmacy.
-
Roda RP, Bagan JV, Bielsa JMS, Pastor EC (2007) Antibiotic use in dental practice. A review. Med Oral Patol Oral Cir Bucal 12(3): E186-E192.
-
Alanis AJ (2005) Resistance to antibiotics: are we in the post-antibiotic era? Arch Med Res 36(6): 697-705.
-
Abdallah EM (2011) Plants: An alternative source for antimicrobials. Journal of Applied Pharmaceutical Science 1(6): 16-20.
-
Arcy PF, Griffin JP (1994) Thalidomide revisited. Adverse Drug React Toxicol Rev 13(2): 65-76.
-
Andrade SE, Gurwitz JH, Davis RL, Chan KA, Finkelstein JA, et al. (2004) Prescription drug use in pregnancy. Am J Obstet Gynecol 191(2): 398-407.
-
Lacroix I, Michel CD, Mestre ML, Montastruc JL (2000) Prescription of drugs during pregnancy in France. Lancet 356(9243): 1735-1736.
-
Tondury G (1967) Die Entstehung angeborener MiBbildungen. Wien Med Wschr 117(1967): 376-379.
-
Heikkila AM (1993) Antibiotics in pregnancy–a prospective cohort study on the policy of antibiotic prescription. Ann Med 25(5): 467-471.
-
Jonge LD, Bos HJ, Langen IMV, Berg LTWDJVD, Bakker MK (2014) Antibiotics prescribed before, during and after pregnancy in the Netherlands: a drug utilization study. Pharmacoepidemiol Drug Saf 23(1): 60-68.
-
Petersen I, Gilbert R, Evans S, Ridolfi A, Nazareth I (2010) Oral antibiotic prescribing during pregnancy in primary care: UK population-based study. J Antimicrob Chemother 65(10): 2238-2246.
-
Yoshioka H, Monma T, Matsuda S (1972) Placental transfer of gentamicin. J Pediatr 80(1): 121-123.
-
Voogd CE, Stel JJVD, Jacobs JJ (1974) The mutagenic action of nitroimidazoles. I. Metronidazole~ nimorazole, dimetridazole and ronidazole. Mutat Res 26(6): 483- 490.
-
Muller AE, DeJongh J, Oostvogel PM, Voskuyl RA, Dörr PJ, et al. (2008) Amoxicillin pharmacokinetics in pregnant women with preterm premature rupture of the membranes. Am J Obstet Gynecol 198(1): 108.
-
Martínez AB, Urízar JMA, Fenoll AB, Carrión AB, Escoda CG, et al. (2004) Consensus statement on antimicrobial treatment of odontogenic bacterial infections. Med Oral Patol Oral Cir Bucal 9(5): 369-376.
-
Nahum GG, Uhl K, Kennedy DL (2006) Antibiotic use in pregnancy and lactation: what is and is not known about teratogenic and toxic risks. Obstet Gynecol 107(5): 1120-1138.
-
Walker CB (1996) Selected antimicrobial agents: mechanisms of action, side effects and drug interactions. Periodontol 2000 10: 12-28.
-
Gruchalla RS, Pirmohamed M (2006) Antibiotic allergy. N Engl J Med 354(21): 601-609.
-
Mensa J, Vázquez EG, Vila J (2003) Macrolides, ketolides and streptogramins. Enferm Infecc Microbiol Clin 21(4): 200-207.
-
Chow AW, Jewesson PJ (1987) Use and safety of antimicrobial agents during pregnancy. West J Med 146(6): 761-764.
-
DiPiro JT, Wells BG, Schwinghammer TL, DiPiro CV (2009) Pharmacotherapy Hand book. 7th (Edn.), McGraw- Hill Companies, Inc, New York.
-
WHO Model List of Essential Medicines. World Health Organization.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’